ABSTRACT
Objective: Individuals with stroke frequently experience mobility deficits
and limited community reintegration. This study aimed to investigate life-space mobility
and relevant factors in community-living individuals with stroke. Methods:
This was a cross-sectional study of 46 community-dwelling individuals with chronic stroke
in Japan (mean age 72.7 ± 7.4 years; mean time post-stroke 63.6 ± 43.3 months; 26 men/20
women). We measured life-space mobility using a Japanese translation of the Life-Space
Assessment. The following factors that might affect life-space mobility were assessed: the
ability to perform activities of daily living, physical performance, fear of falling, and
cognitive function. Results: A total of 41 participants (89.1%) had
restricted life-space mobility (Life-Space Assessment score <60 points). A multiple
linear regression analysis showed that limitations in activities of daily living, walking
speed, and Falls Efficacy Scale-International scores were independently related to
Life-Space Assessment scores. This model explained 51.3% of the variance in Life-Space
Assessment scores. Conclusions: Most individuals with stroke had restricted
life-space mobility. Life-space mobility was associated with the ability to perform
activities of daily living, walking speed, and fear of falling. These findings could
contribute to the development of rehabilitation interventions for regaining life-space
mobility in individuals with stroke.
INTRODUCTION
Stroke is a major cause of disability worldwide and the leading cause of long-term care
needs in Japan.1) Mobility
limitation is one of the most common problems following stroke; 39.2–82.3% of individuals
with stroke have post-stroke limitations in community ambulation.2,3,4)
Furthermore, reduced mobility is predictive of the future risk of deteriorations in health
and functionality in community-living older adults.5,6) Therefore, the improvement of mobility is the primary
rehabilitation goal for individuals with stroke.
Several measures have been used to estimate community mobility among stroke survivors.
Self-reported mobility (which encompasses both mobility around the home and mobility in more
distant and challenging environments) is an effective and simple outcome measure for
clinical use.7) Life-space
mobility is quantified using self-report measures of the spatial extent (range), frequency,
and independence of mobility, from being confined to the bedroom to being able to access
community facilities. Life-space mobility is associated with quality of life8,9) and self-reported health.9) Life-space mobility is the most frequently used measure in
gerontology and is a valuable quantitative measure of social integration among
community-living stroke survivors. Consequently, the investigation of life-space mobility
after stroke and the identification of related factors could help clinicians to plan
therapeutic interventions for extending life-space mobility post-stroke.
Many previous studies have shown that life-space mobility is mainly linked to physical
performance,9,10,11) the ability to perform activities of daily living
(ADL),9,10,11) cognitive function,9,10) and mental health9,10) in community-living older adults. However, only one study has
examined in detail factors relevant to life-space mobility after stroke, demonstrating that
physical performance, cognitive function, and falls efficacy predicted life-space mobility
for stroke patients in Japan 2 months after hospital discharge.12) However, it is not known what factors are
associated with life-space mobility in individuals with chronic stroke receiving long-term
day care because of self-care disability. Thus, the principal aim of this study was to
investigate life-space mobility after stroke and examine the relationship between life-space
mobility and selected functionality and cognitive measures in community-living stroke
survivors who were receiving long-term day care.
METHODS
Study Design
This was a cross-sectional observational study conducted between June and August 2013 in
two daycare centers for older adults in Saitama, Japan. The study was approved by the
Ethics Committee of the Saitama Cooperative Hospital (approval number 13–1–2). All
participants gave informed consent prior to the study.
Participants
Community-living individuals with stroke who were receiving adult daycare services were
recruited. Inclusion criteria were that participants (1) had had a stroke at least 6
months before the study; (2) had no musculoskeletal or neurological disorders other than
stroke that affected their gait; and (3) could walk at least 16 m without physical
assistance. Exclusion criteria were that participants (1) were younger than 50 years and
(2) were unable to understand the instructions because of communicative or severe
cognitive dysfunction as indicated by more than 5 out of 10 errors on the Short Portable
Mental Status Questionnaire (SPMSQ).13) No statistical power calculation was performed prior to the
study: the sample size was determined by the number of stroke individuals using the
participating daycare services.
Procedure
Data on demographics and stroke-related characteristics were obtained from patients’
medical records. All clinical assessments were conducted by two trained physical
therapists. Scores for subjective performance measures were agreed upon by the two
assessors.
Measurement
We assessed life-space mobility using a Japanese translation of the Life-Space Assessment
(LSA) (Table 1).14) The LSA was developed to measure the mobility
status in older people.9) Our
participants reported their mobility over the 4 weeks before assessment. Life space was
categorized using 6 levels: 0=bedroom, 1=home, 2=outside the home, 3=neighborhood, 4=town,
and 5=beyond the town. Participants were asked how often they spent time in locations at
each level (less than once a week, 1–3 times a week, 4–6 times a week, daily) and how
independent they were (whether they needed help from another person or used assistive
devices). The LSA score ranges from 0 (totally bed-bound) to 120 (able to travel out of
town every day without assistance). A score below 60 reflects restricted life-space
mobility and indicates that participants generally remained at home or in their
neighborhood.15) The LSA
has shown excellent test–retest reliability.9)
Table 1.
Elements of the Life-Space Assessment Score
| Life-space level |
× |
Frequency |
× |
Independence |
| 1: |
Home |
|
1: |
Less than 1/week |
|
1: |
Help from another person |
| 2: |
Outside the home |
|
2: |
1≤3/week |
|
1.5: |
Equipment only |
| 3: |
Neighborhood |
|
3: |
4 ≤6/week |
|
2: |
No equipment or personal assistance |
| 4: |
Town |
|
4: |
Daily |
|
|
|
| 5: |
Beyond the town |
|
|
|
|
|
|
We assessed each participant’s ability to perform ADL using the Barthel Index
(BI).16) This comprises
ten ADL items divided into three subgroups: (1) personal care, including eating, dressing,
personal hygiene, and bathing; (2) urinary and fecal continence; and (3) mobility,
including transfers to and from the bed and the toilet, walking, and using stairs. We
asked participants about their dependence level for each activity. This index has
excellent interrater reliability in persons with chronic stroke.17)
Motor function in the lower extremities of individuals with hemiplegia was assessed using
the Brunnstrom Recovery Stages (BRS).18) Participants were asked to perform voluntary movements of
their lower limbs, and motor function was categorized as indicating 1 of 6 stages. The BRS
has almost perfect interrater reliability in stroke patients.19)
Walking speed was measured using a 10-m walking test. Participants were asked to walk
16 m at their maximum speed using their usual assistive and orthotic devices. The time
taken to walk the middle 10 m of the 16 m was measured using a digital stopwatch to
calculate walking speed. This test has excellent test–retest reliability in persons with
chronic stroke.20)
We evaluated cognitive impairment using the SPMSQ,13) which is a widely used 10-item cognitive examination that
is useful for rapidly screening cognitive function. A score of 5 or more errors on the
SPMSQ indicates moderate to severe cognitive impairment; a score of 3–4 errors indicates
mild cognitive impairment; a score of 0–2 errors indicates cognitive intactness.14) The SPMSQ has shown good
reliability and validity.21)
Fear of falling was evaluated using a Japanese translation of the Falls Efficacy
Scale-International (FES-I).22) The FES-I is a 16-item questionnaire that asks respondents
to assess their confidence in performing basic and instrumental ADL, walking outdoors, and
going to social events or crowded places without falling.23) Each item is scored from 1 to 4 (1=not at all
concerned and 4=very concerned); the total score therefore ranges from 16 to 64. A higher
score indicates greater concern about falling. The FES-I has excellent internal and
test–retest reliability.23)
History of falling was self-reported by participants, based on their recall of falls in
the previous 12 months. Falls were defined as “an unexpected event in which the
participants come to rest on the ground, floor, or lower level.”24) We classified participants as either with or
without a history of falls.
Statistical Analyses
We analyzed the data using SPSS, version 19.0 (IBM Japan Ltd., Tokyo, Japan). The
Shapiro–Wilk test was used to examine the normality of variables. We used Pearson’s
correlation to examine the relationships between the LSA score and the independent
variables. For ordinal variables, including BRS of lower extremities, SPMSQ errors, and
FES-I score, we conducted Spearman’s correlation analysis. An unpaired t
test was used to assess the relationship between the LSA score and categorical
variables.
We used stepwise multiple linear regression analysis to examine whether the potential
factors were associated independently with the LSA score. Variables were entered into the
regression model if their P value was less than 0.10 in a univariate
analysis with the LSA score. The statistical significance level was P
<0.05 for all analyses.
RESULTS
After excluding data from those participants aged less than 50 years (n=2) and those with
cognitive dysfunction (SPMSQ >5; n=4), we analyzed data from 46 participants (26 of which
were men). The average age of participants was 72.7 ± 7.4 years and the average time since
stroke was 63.6 ± 43.3 months (Table 2). Two
participants with double vision/spatial neglect were included in the statistical analysis
because excluding their data did not affect the results. The mean LSA score was 42.1 ± 14.4,
and 41 (89.1%) participants had restricted life-space mobility (Table 2 and Fig. 1).
Table 2.
Characteristics of the participants
|
Mean ± SD or n |
Median (interquartile range) |
| Age (years) |
72.7 ± 7.4 |
73.5 (67–77.75) |
| Sex, male/female (n) |
26/20 |
|
| BMI (kg/m2) |
24.0 ± 3.7 |
23.2 (21.6–26.1) |
| Type of stroke, ischemic/hemorrhagic (n) |
35/11 |
|
| Paretic side, right/left (n) |
23/23 |
|
| Time since stroke (months) |
63.6 ± 43.3 |
49.5 (32–90.5) |
| BI score (0–100) |
89.8 ± 10.1 |
90 (85–100) |
| BRS of lower extremity, 2/3/4/5/6 (n) |
2/16/8/3/17 |
4 (3–6) |
| Walking speed (m/s) |
0.70 ± 0.38 |
0.68 (0.38–0.94) |
| SPMSQ errors (0–10) |
1.8 ± 1.3 |
2 (1–3) |
| FES-I score (16–64) |
41.8 ± 10.7 |
43.5 (34–50) |
| Fall history, yes/no (n) |
19/27 |
|
| LSA score (0–120) |
42.1 ± 14.4 |
39 (29.5–51) |
| Life-space restriction (LSA score <60, n) |
41 |
|
BMI, body mass index; BI, Barthel Index; BRS, Brunnstrom Recovery Stages; SPMSQ, Short
Portable Mental Status Questionnaire; FES-I, Falls Efficacy Scale-International; LSA,
Life-Space Assessment.
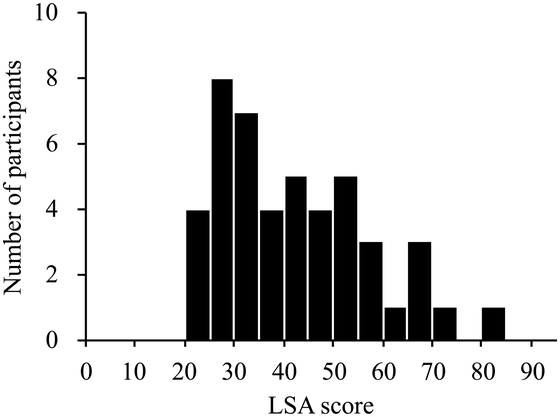
Table 3 shows the relationship between the LSA
score and the other variables. There was a significant correlation between the LSA score and
the BI score (r=0.715, P <0.001) and the LSA score and
walking speed (r=0.584, P <0.001). There were no
differences in LSA scores between men and women, the type of stroke, the side of hemiplegia,
and individuals with or without a history of falling.
Table 3.
Relationships between Life-Space Assessment score and other variables
|
Correlation coefficient |
P |
| Age |
0.129 |
0.392 |
| BMI |
0.085 |
0.576 |
| Time since stroke |
–0.037 |
0.806 |
| BI score |
0.715 |
<0.001 |
| BRS of lower extremity |
0.218 |
0.145 |
| Walking speed |
0.584 |
<0.001 |
| SPMSQ errors |
–0.125 |
0.408 |
| FES-I score |
–0.259 |
0.083 |
We performed multiple regression analysis to determine whether the BI score, the walking
speed, or the FES-I score were associated with the LSA score after stroke. The results are
shown in Table 4. The factors retained in this
model were the BI score (β=0.404, P=0.005), the walking speed (β=0.339,
P=0.017), and the FES-I score (β=–0.224, P=0.039).
Overall, 51.3% of the variance in the LSA score was explained by this regression model
(F2,45=16.776, P <0.001).
Table 4.
Factors associated with the LSA score identified using multivariate
analysis
|
B |
95% CI |
β |
P |
|
Lower limit |
Upper limit |
| BI score |
0.580 |
0.190 |
0.970 |
0.404 |
0.005 |
| Walking speed |
12.847 |
2.460 |
23.234 |
0.339 |
0.017 |
| FES-I score |
–0.303 |
–0.590 |
–0.015 |
–0.224 |
0.039 |
B, unstandardized regression coefficient; CI, confidence interval; β, standardized
regression coefficient
DISCUSSION
This study used a linear regression model to investigate the association between life-space
mobility and physical performance, cognitive function, psychosocial factors, and
sociodemographic variables in community-living stroke survivors who were receiving long-term
day care. Notably, the life-space mobility for most participants was restricted to the home
or immediate neighborhood. The main study finding was that the ability to perform ADL, the
walking speed, and the fear of falling were associated with life-space mobility in
individuals with stroke. These results indicate that community-living individuals with
stroke usually experience restricted life-space mobility. ADL ability, walking speed, and
fear of falling are factors that may be important when considering how to improve life-space
mobility in stroke survivors.
In this study, 89.1% of participants had restricted life-space mobility. This was higher
than that found in previous studies of community-living adults (including those who had a
stroke) aged 65 years or older (41.3%)25) and aged 75–90 years (41.0%).26) Moreover, the average LSA score for community
dwelling older adults in the USA is 64.1 ± 24.9,10) and for Japanese older adults using preventive health care
services, the average LSA score is 51.4 ± 25.2.14) The median score for stroke survivors 2 months after
hospital discharge in Japan was 64 (quartiles, 41.5–96),12) which is higher than that for our participants. However,
taken together, these findings indicate that most stroke survivors receiving long-term day
care have limited community mobility. The above-mentioned results may have arisen from
differences in the characteristics of the participants in that study;12) participants were younger (median
age, 65 years; quartiles, 58–73 years) and had better lower limb function (median BRS, 5;
quartiles, 4–6) than those in the present study. These factors may affect life-space
mobility directly and/or indirectly through physical depression. Overall, restricted
life-space mobility was a dominant factor for our participants, and the results suggested
that regaining the ability to walk outdoors and reintegration into the community are
important post-stroke rehabilitation goals even for individuals in the chronic stage of
stroke recovery who are receiving long-term day care.
We found that walking speed was associated with life-space mobility among stroke
individuals. Walking speed is a reliable, valid measure of mobility in individuals with
stroke7) and is strongly
associated with levels of community ambulation.2,3,27) Individuals with impaired walking ability resulting from
stroke exhibit neuromotor problems.28,29,30,31) Slower walking speed is one of the most common problems in
the stroke population32); this
was confirmed in our participants. Furthermore, walking speed has been used as an important
physical indicator of community ambulation levels of people with stroke.2,3,4,7)
Therefore, improving walking speed should be prioritized in efforts to extend life-space
mobility in stroke rehabilitation.
In this study, ADL performance was related to life-space mobility. This result is in accord
with reports that ADL disability is negatively associated with life-space mobility in older
adults.10,11) It is possible that ADL disability
was one reason why our participants were disinclined to leave their homes. One literature
review33) indicated
improvements in ADL in stroke survivors from 3 to 12 months post-stroke, but no significant
change in ADL from 1 to 3 years post-stroke. In addition, 12–40% of stroke survivors
retained some ADL disability.33) Most of our participants experienced one or more difficulties
with ADL, which may have reduced life-space mobility. We observed that an ability to perform
ADL tasks is necessary to extend life-space mobility.
Our regression model indicated that greater fear of falling was associated with restricted
life-space mobility. This result is in accord with previous findings that fear of falling
leads to unnecessary avoidance of activities and social participation among elderly
adults34,35) and among those with
stroke.35,36,37,38,39) Tsai et al.40) reported fear of falling in almost 70% of community-dwelling
stroke survivors, who also had related balance deficits41) and falls.40,41) Therefore, to optimize community reintegration, reduction of
fear of falling should be a focus in rehabilitation settings. Notably, none of our study
subjects stated that they were confident in carrying out all daily activities without
falling. It is not known whether reducing fear of falling is effective in extending
life-space mobility in community-living individuals with stroke. Future studies should
examine whether exercises may reduce fear of falling and the effects of such programs on
community reintegration.
Overall, we found that the ability to perform ADL, the walking speed, and fear of falling
were associated with life-space mobility in individuals with stroke and accounted for 51.3%
of the variance in LSA score; these components and the associated variance are similar to
those identified in previous studies of community-dwelling elderly people10,11) and in stroke patients 2 months after hospital
discharge.12) These
findings could help therapists and community-dwelling individuals with chronic stroke to set
clear and appropriate rehabilitation goals to regain community mobility. Moreover, routine
monitoring of LSA and measurement of the relevant factors discussed here may help to
encourage and/or maintain community mobility in stroke survivors.
The present study has several limitations. First, the study design was cross-sectional;
consequently, we could examine only correlations between life-space mobility and the
independent variables. We could not clarify whether the time since onset or since hospital
discharge can affect life-space mobility in this population. Second, our sample comprised
only elderly adults with chronic stroke receiving daycare services. Our findings cannot
therefore be generalized to other populations of stroke survivors who are high functioning
and independently living in the community. Third, LSA, BI, and history of falling were
determined by retrospective self-reports. This method may have been affected by recall bias
because some participants had mild cognitive impairment. Additional studies encompassing
longitudinal analysis and involving more participants from a wider range of backgrounds are
needed to investigate the determinants of life-space mobility.
CONCLUSIONS
Most of our participants had restricted life-space mobility. The findings indicated that
restricted life-space mobility was associated with limitations in ADL, poorer physical
performance, and fear of falling. Our findings may contribute to the development of
comprehensive strategies to help individuals with chronic stroke reintegrate into the
community.
ACKNOWLEDGMENTS
The authors thank the participating facilities and their staff for cooperation and
assistance in data collection. We thank Diane Williams, PhD, from Edanz Group
(www.edanzediting.com/ac) for editing a draft of this manuscript.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
- 1.Ministry of Health, Labour and Welfare,
Government of Japan. Summary report of comprehensive survey of living conditions in 2013:
https://www.mhlw.go.jp/english/database/db-hss/dl/report_gaikyo_2013.pdf
- 2. Perry J, Garrett M, Gronley JK, Mulroy SJ:
Classification of walking handicap in the stroke population. Stroke 1995;26:982–989.
PMID:7762050, DOI:10.1161/01.STR.26.6.982
- 3. Lord SE, McPherson K, McNaughton HK, Rochester L,
Weatherall M: Community ambulation after stroke: how important and obtainable is it and
what measures appear predictive? Arch Phys Med Rehabil 2004;85:234–239. PMID:14966707,
DOI:10.1016/j.apmr.2003.05.002
- 4. van de Port IG, Kwakkel G, Lindeman E: Community
ambulation in patients with chronic stroke: how is it related to gait speed? J Rehabil Med
2008;40:23–27. PMID:18176733, DOI:10.2340/16501977-0114
- 5. Portegijs E, Rantakokko M, Viljanen A, Sipilä S,
Rantanen T: Identification of older people at risk of ADL disability using the Life-Space
Assessment: a longitudinal cohort study. J Am Med Dir Assoc 2016;17:410–414.
PMID:26805752, DOI:10.1016/j.jamda.2015.12.010
- 6. Shimada H, Sawyer P, Harada K, Kaneya S, Nihei K,
Asakawa Y, Yoshii C, Hagiwara A, Furuna T, Ishizaki T: Predictive validity of the
classification schema for functional mobility tests in instrumental activities of daily
living decline among older adults. Arch Phys Med Rehabil 2010;91:241–246. PMID:20159128,
DOI:10.1016/j.apmr.2009.10.027
- 7. Lord SE, Rochester L: Measurement of community
ambulation after stroke: current status and future developments. Stroke 2005;36:1457–1461.
PMID:15947265, DOI:10.1161/01.STR.0000170698.20376.2e
- 8. Rantakokko M, Portegijs E, Viljanen A, Iwarsson
S, Kauppinen M, Rantanen T: Changes in life-space mobility and quality of life among
community-dwelling older people: a 2-year follow-up study. Qual Life Res
2016;25:1189–1197. PMID:26407605, DOI:10.1007/s11136-015-1137-x
- 9. Baker PS , Bodner EV, Allman RM: Measuring
life-space mobility in community-dwelling older adults. J Am Geriatr Soc
2003;51:1610–1614.
- 10. Peel C, Baker PS, Roth DL, Brown CJ, Brodner EV,
Allman RM: Assessing mobility in older adults: the UAB Study of Aging Life-Space
Assessment. Phys Ther 2005;85:1008–1119.
- 11. Murata C, Kondo T, Tamakoshi K, Yatsuya H,
Toyoshima H: Factors associated with life space among community-living rural elders in
Japan. Public Health Nurs 2006;23:324–331. PMID:16817803,
DOI:10.1111/j.1525-1446.2006.00568.x
- 12. Nakao M, Izumi S, Yokoshima Y, Matsuba Y, Maeno
Y: Prediction of life-space mobility in patients with stroke 2 months after discharge from
rehabilitation: a retrospective cohort study. Disabil Rehabil 2019;24:1–8. PMID:30676134,
DOI:10.1080/09638288.2018.1550533
- 13. Pfeiffer E: A short portable mental status
questionnaire for the assessment of organic brain deficit in elderly patients. J Am
Geriatr Soc 1975;23:433–441. PMID:1159263,
DOI:10.1111/j.1532-5415.1975.tb00927.x
- 14. Harada K, Shimada H, Baker PS, Asakawa Y, Nihei
K, Kaneya S, Furuna T, Ishizaki T, Yasumura S: [Life-space of community-dwelling older
adults using preventive health care services in Japan and the validity of composite
scoring methods for assessment]. Nippon Koshu Eisei Zasshi
2010;57:526–537.
- 15.Baker PS, Allman RM: Resilience in mobility in
the context of chronic disease and aging: cross-sectional and prospective findings from
the University of Alabama at Birmingham (UAB) Study of Aging. Frontiers of resilient
aging: Life-strengths and wellness in late life 2010:310–339.
- 16. Mahoney FI, Barthel DW: Functional evaluation:
the Barthel Index. Md State Med J 1965;14:61–65.
- 17. Duffy L, Gajree S, Langhorne P, Stott DJ, Quinn
TJ: Reliability (inter-rater agreement) of the Barthel Index for assessment of stroke
survivors: systematic review and meta-analysis. Stroke 2013;44:462–468. PMID:23299497,
DOI:10.1161/STROKEAHA.112.678615
- 18. Brunnstrom S: Motor testing procedures in
hemiplegia: based on sequential recovery stages. Phys Ther 1966;46:357–375. PMID:5907254,
DOI:10.1093/ptj/46.4.357
- 19. Shah SK: Reliability of the original Brunnstrom
recovery scale following hemiplegia. Aust Occup Ther J 1984;31:144–151.
DOI:10.1111/j.1440-1630.1984.tb01473.x
- 20. Ng SS, Hui-Chan CW: The timed up & go test:
its reliability and association with lower-limb impairments and locomotor capacities in
people with chronic stroke. Arch Phys Med Rehabil 2005;86:1641–1647. PMID:16084820,
DOI:10.1016/j.apmr.2005.01.011
- 21. Foreman MD: Reliability and validity of mental
status questionnaires in elderly hospitalized patients. Nurs Res 1987;36:216–219.
PMID:3299279, DOI:10.1097/00006199-198707000-00004
- 22. Kamide N, Shiba Y, Takahashi K, Inaba Y, Haga H:
Reliability and validity of the Falls Efficacy Scale International in Japanese
community-dwelling elderly women. Sogo Rehabil 2010;38:1063–1069.
- 23. Yardley L, Beyer N, Hauer K, Kempen G,
Piot-Ziegler C, Todd C: Development and initial validation of the Falls Efficacy
Scale-International (FES-I). Age Ageing 2005;34:614–619. PMID:16267188,
DOI:10.1093/ageing/afi196
- 24. Gibson MJ. Falls in later life. In: Kane RL,
Evans JG, Macfadyen D, editors. Improving the health of older people: a world view. New
York: Oxford Univ Press; 1990. pp. 296–315.
- 25. Sheppard KD, Sawyer P, Ritchie CS, Allman RM,
Brown CJ: Life-space mobility predicts nursing home admission over 6 years. J Aging Health
2013;25:907–920. PMID:23965310, DOI:10.1177/0898264313497507
- 26. Rantakokko M, Iwarsson S, Portegijs E, Viljanen
A, Rantanen T: Associations between environmental characteristics and life-space mobility
in community-dwelling older people. J Aging Health 2015;27:606–621. PMID:25326130,
DOI:10.1177/0898264314555328
- 27. Viosca E, Martínez JL, Almagro PL, Gracia A,
González C: Proposal and validation of a new functional ambulation classification scale
for clinical use. Arch Phys Med Rehabil 2005;86:1234–1238. PMID:15954065,
DOI:10.1016/j.apmr.2004.11.016
- 28. Nadeau S, Arsenault AB, Gravel D, Bourbonnais D:
Analysis of the clinical factors determining natural and maximal gait speeds in adults
with a stroke. Am J Phys Med Rehabil 1999;78:123–130. PMID:10088586,
DOI:10.1097/00002060-199903000-00007
- 29. Dorsch S, Ada L, Canning CG, Al-Zharani M, Dean
C: The strength of the ankle dorsiflexors has a significant contribution to walking speed
in people who can walk independently after stroke: an observational study. Arch Phys Med
Rehabil 2012;93:1072–1076. PMID:22464738, DOI:10.1016/j.apmr.2012.01.005
- 30. Bohannon RW, Andrews AW: Correlation of knee
extensor muscle torque and spasticity with gait speed in patients with stroke. Arch Phys
Med Rehabil 1990;71:330–333.
- 31. Verheyden G, Vereeck L, Truijen S, Troch M,
Herregodts I, Lafosse C, Nieuwboer A, De Weerdt W: Trunk performance after stroke and the
relationship with balance, gait and functional ability. Clin Rehabil 2006;20:451–458.
PMID:16774097, DOI:10.1191/0269215505cr955oa
- 32. Dean CM, Richards CL, Malouin F: Walking speed
over 10 metres overestimates locomotor capacity after stroke. Clin Rehabil
2001;15:415–421. PMID:11518442, DOI:10.1191/026921501678310216
- 33. Wondergem R, Pisters MF, Wouters EJ, Olthof N, de
Bie RA, Visser-Meily JM, Veenhof C: The course of activities in daily living: who is at
risk for decline after first ever stroke? Cerebrovasc Dis 2017;43:1–8. PMID:27750246,
DOI:10.1159/000451034
- 34.Denkinger MD, Lukas A, Nikolaus T, Hauer K:
Factors associated with fear of falling and associated activity restriction in
community-dwelling older adults: a systematic review. 2015;23:72–86.
- 35. Auais M, Alvarado B, Guerra R, Curcio C, Freeman
EE, Ylli A, Guralnik J, Deshpande N: Fear of falling and its association with life-space
mobility of older adults: a cross-sectional analysis using data from five international
sites. Age Ageing 2017;46:459–465. PMID:28043980,
DOI:10.1093/ageing/afw239
- 36. Pang MY, Eng JJ, Miller WC: Determinants of
satisfaction with community reintegration in older adults with chronic stroke: role of
balance self-efficacy. Phys Ther 2007;87:282–291. PMID:17284545,
DOI:10.2522/ptj.20060142
- 37. Vahlberg B, Cederholm T, Lindmark B, Zetterberg
L, Hellström K: Factors related to performance-based mobility and self-reported physical
activity in individuals 1-3 years after stroke: a cross-sectional cohort study. J Stroke
Cerebrovasc Dis 2013;22:e426–e434. PMID:23721615,
DOI:10.1016/j.jstrokecerebrovasdis.2013.04.028
- 38. Liu TW, Ng SS, Kwong PW, Ng GY: Fear avoidance
behavior, not walking endurance, predicts the community reintegration of
community-dwelling stroke survivors. Arch Phys Med Rehabil 2015;96:1684–1690.
PMID:26002203, DOI:10.1016/j.apmr.2015.05.005
- 39. Robinson CA, Shumway-Cook A, Ciol MA, Kartin D:
Participation in community walking following stroke: subjective versus objective measures
and the impact of personal factors. Phys Ther 2011;91:1865–1876. PMID:22003172,
DOI:10.2522/ptj.20100216
- 40. Tsai S, Yin J, Tung T, Shimada T: Falls efficacy
among stroke survivors living in the community. Disabil Rehabil 2011;33:1785–1790.
PMID:21250868, DOI:10.3109/09638288.2010.546938
- 41. Schmid AA, Arnold SE, Jones VA, Jane Ritter M,
Sapp SA, Van Puymbroeck M: Fear of falling in people with chronic stroke. Am J Occup Ther
2015;69:6903350020p1. PMID:25871606, DOI:10.5014/ajot.2015.016253