Effects of the WISH-type S-form Hip Brace on Muscle Strength in Patients with Osteoarthritis of the Hip: A Short-term Longitudinal Study
2019 Volume 4 Article ID: 20190015
Details
2019 Volume 4 Article ID: 20190015
Background: The WISH-type S-form hip brace (WISH brace) has been shown to significantly improve hip function, functional mobility, and gait biomechanics in patients with hip osteoarthritis. The aim of the current study was to evaluate the effects of the WISH brace over time on the strength of muscles around the hip and knee joints. Methods: A prospective short-term longitudinal study with a 6-month follow-up was conducted. Muscle strengths were measured using a handheld dynamometer. Results: The muscle strengths of hip flexion, hip abduction, and knee extension were lower in the affected limb than in the unaffected limb, whereas hip adduction muscle strength was reduced to the same extent in both the affected and unaffected limbs. This short-term longitudinal study revealed that only hip adduction and knee extension exhibited significant interaction between legs and time when measurement was performed without the WISH brace. Furthermore, the inherent hip abduction muscle strength of the affected limb was improved by the WISH brace so that the strength became the same as the unaffected limb. Conclusions: Improvement in abduction muscle strength of the affected limb by daily walking exercise with the WISH brace, which occurred with little interaction with the unaffected limb, may improve hip function.
Osteoarthritis (OA) is the most common form of arthritis.1) It is a joint disorder that results in joint pain and stiffness2) and is the leading cause of disability in the elderly.2) The pain associated with OA of the hip is usually related to daily activities, such as climbing stairs, walking, and engaging in work.1) Clinical guidelines advocate a combination of conservative non-drug and drug therapies for optimal treatment of hip OA.3) However, the majority of treatments currently available for OA involve drugs and/or surgery.4) Conservative treatments include analgesics, physical therapy, and bracing. The surgical approach of total hip arthroplasty (THA) provides reliable outcomes for patients with end-stage degenerative hip OA, specifically pain relief, functional restoration, and overall improved quality of life. However, major complications may occur following THA; these include dislocation, periprosthetic fracture, aseptic loosening, wound complications, and prosthetic joint infection.5) For patients with less severe OA, conservative treatments play an important role, especially for younger patients.
We previously developed a hip brace, the WISH-type S-form hip brace (WISH brace), and reported its effects on hip-functional responses of patients with unilateral6) and bilateral7) OA. Pain relief on gait was observed after the initial use of the WISH brace.6) A series of studies has elucidated the biomechanical effects of the WISH brace. For hip OA patients fitted with the WISH brace, the average time to complete the Timed Up & Go Test was significantly shorter than for those without the brace, suggesting that the WISH brace improves hip function during external and/or abduction movements at the turning phase.8) In the cross test, augmentation of the power output of the adductor and flexor muscles by the brace may support the moment required for resistance against the upper body mass when leaning backward on the braced side, which may enable excursions of the center of pressure to be altered.9) Gait analysis revealed that application of the WISH brace resulted in a stronger vertical reaction force at the first peak during the early stance, and an earlier switch between backward and forward reaction force vectors.10) Moreover, daily walking exercise may also be associated with the improvement of hip function in patients with hip braces.6,9) However, the mechanisms underlying augmentation of the power output in muscles around the hip joint with the use of the WISH brace remain unclear.
Isometric hip abduction,11,12) adduction,11) flexion,11) and internal rotation12) strength were reduced in patients in the hip OA group when compared with a control group. However, isometric and isokinetic extension strength did not differ between the groups.11) There were no significant differences between groups in external hip rotation.12) On the other hand, comparisons between OA and healthy limbs in the patients, isometric hip extension,11,13) flexion,11,13) adduction,13) abduction,13) and knee extension13) strength were reduced in the OA limb as compared with the healthy limb. Furthermore, neither adduction nor abduction strength values differed between the affected and unaffected side in OA subjects.11) In patients with hip OA, the reduced hip abductor muscle strength mediates the relationship between avoidance of activity and limitations in activities.14) Thus the muscle strength around the hip joint may affect hip functions and play an important role in their improvement of those by the WISH brace.
In the present study, we examined the effects of the WISH brace on the strength of muscles around the hip joint by using a hand-held dynamometer (HHD) in patients with hip OA. A HHD is a portable measurement device often used for assessing hip muscle function.15) A high intra-class correlation coefficient was obtained for HHD measurements in patients with OA of the hip.9) In the current short-term longitudinal study, the muscle strengths of affected and unaffected limbs were compared.
Between August 2011 and March 2013, patients with symptomatic unilateral OA of the hip were referred to the outpatient clinic of Gunma University Hospital. Hip OA was defined according to the clinical criteria of the American College of Rheumatology.16) Patients in whom the hip pain induced by weight bearing during gait was notably reduced by manual pressure on the greater trochanter were recruited for this study.
Subjects who were on a waiting list for hip replacement or had previously undergone hip replacement were excluded. Subjects for whom a WISH brace was used for both hips were also excluded. The radiological grade of OA was estimated according to the grading system proposed by Crowe et al.,17) and patients with radiological grade III or IV were excluded.
The study was conducted after approval by the local Ethics Committee (Gunma University, Maebashi, Gunma, Japan), and informed consent for the study was received from each individual participating in the study.
Hip BraceThe WISH brace was based on the design concept of the Wakayama Medical College,18) and the effects of the WISH brace were previously reported.6) The pelvic portion of the hip brace holds it at the correct position against the pelvis to prevent rotation of the brace and provides a fulcrum for the lever though a lateral bar, possessing two single joints, the combination of which restricts only hip adduction. The greater trochanter pad is fixed directly to the upper extended bar attached to the lower hip joint bar, producing medial pressure on standing. Furthermore, an S-form bar holding the thigh is made of co-polymer polypropylene material with continuity to the greater trochanter pad. The brace weighs approximately 0.9 kg.
Exercise TherapyTo strengthen the muscles around the hip joint required for gait, patients equipped with the WISH brace were required to walk for at least 30 min every day. Home exercises consisting of hip muscle strengthening exercises with the use of a weight were suggested. Furthermore, gait exercise in water was additionally recommended.6)
Assessment of the Strength of Muscles Around the HipMuscle strength testing was performed with the patient lying on an examination table according to the method described by Thouborg et al.15) using the Power Track II Commander HHD (JTECK Medical, Midvale, UT, USA). The HHD was calibrated on each test day, and all test procedures were standardized. All strength tests were isometric strength tests. Each subject performed hip flexion (FLEX), abduction (ABD), adduction (ADD), and knee extension (K-EXT). FLEX and K-EXT were assessed in the sitting position, and ABD and ADD were assessed in the supine position, corresponding to HF-SIP, HIR-SIP, HABD-SUP, and HADD-SUP, respectively, in the report of Thouborg et al.15) The participants were asked to stabilize themselves by holding the sides of the table with their hands. The examiner applied resistance in a fixed position and the patient being tested exerted a 5-s isometric maximum voluntary contraction against the dynamometer and the examiner. In the present study, to avoid involvement of the knee joint, the examiner’s hand was set just above the knee for the hip movements. To assess K-EXT, resistance was applied at the level of the malleoli. Each individual test was administered three times to reduce possible learning effects. There was a 30-s rest period between two consecutive trials to avoid a decline in strength across trials due to fatigue in patients with spinal cord injury.19) The mean maximal torque values were divided by the patient’s body weight to calculate the relative muscle torque (Nm/kg).
Hip Function AssessmentsHip function was evaluated using the Harris Hip Score (HHS).20) The HHS was considered to be the primary outcome measure and consists of four variables: pain, functional capacity, range of motion, and deformity. The maximum HHS score is 100, and a score of less than 70 reportedly reflects poor functioning (poor category).20)
Statistical AnalysesTo compare HHS over months 0, 1, 3, and 6, we used repeated-measures analysis of variance (ANOVA), followed by post hoc comparisons with the Bonferroni correction. The average muscle strength was compared between the affected and unaffected sides using the paired t-test or the Wilcoxon signed-rank test after the Shapiro-Wilk test was performed to determine whether the data were normally distributed.
There were two within-group independent variables: one with four conditions (FLEX, ADD, ABD, and K-EXT) and the other with two conditions (affected/unaffected). To evaluate the muscle strength longitudinally, data analysis was conducted using two-way ANOVA with repeated measures. The time effect, the leg × time interaction, and the leg effect were determined. In brief, the ANOVA procedure considered the with-brace and without-brace results to depend on two within-subject factors: the type of muscle and the affected leg or unaffected leg. One purpose of the ANOVA analysis was to establish whether the change in muscle strength between the affected and unaffected legs was dependent on each muscle. To single out individual effects of the muscle type and leg side, we considered whether such interactions were significant.
If the leg × time interaction was not significant, the characteristics of each leg (affected and unaffected leg) were analyzed using one-way ANOVA with repeated measurements. Dunnet’s post hoc analysis was used to compare each group’s muscle strength with that before the brace intervention was started.21) P-values of less than 0.05 were considered to be significant.
A total of 10 patients, all female, were recruited (Table 1). The patients ranged in age from 36 to 65 years, and the average was 51.6 years (SD, 9.5 years). Five patients had OA of the right hip and five patients had OA of the left hip. Seven patients were radiological grade I and three patients were grade II.
| Patient number |
Age | Sex | Radiographical gradea | Site of OA hip | HHS evaluated after use of the WISH brace | |||
| 0 monthsb | 1 month | 3 months | 6 months | |||||
| 1 | 49 | F | II | L | 50 | 70 | 73 | 76 |
| 2 | 38 | F | II | L | 47.7 | 77.7 | 94.7 | 82.7 |
| 3 | 54 | F | I | R | 65.7 | 75.7 | 95.7 | 95.7 |
| 4 | 51 | F | I | R | 66 | 76 | 81 | 94 |
| 5 | 36 | F | I | R | 63 | 73 | 85 | 75 |
| 6 | 57 | F | I | L | 61 | 73 | 73 | 69.0 |
| 7 | 65 | F | I | R | 59 | 76 | 72 | 72 |
| 8 | 52 | F | I | L | 76 | 76 | 76 | 91 |
| 9 | 50 | F | I | L | 76 | 93 | 91 | 91 |
| 10 | 64 | F | II | R | 62.7 | 75.7 | 95.7 | 91.7 |
| Mean±SD | 62.7±9.3 | 76.6±6.2* | 83.7±10* | 83.8±10.1* | ||||
F female, R right, L left.
aRadiological grade was evaluated according to Crowe et al.17)
bMonths after start of brace intervention.
*Significantly different from 0 months (P<0.05).
Eight hip joints had a poor hip function score (<70)20) on the first assessment. After the WISH brace was used, HHS improved in all patients, as shown in Table 1. However, in one patient, hip function was poor again after 6 months. One factor influencing the score reduction in this patient was the requirement of a cane when walking long distances. However, pain was improved at the 1-month follow-up assessment, and the pain improvement was maintained until the 6-month follow-up assessment. Significant improvements in the average HHS were observed at months 1, 3, and 6 compared with the initial assessment.
Comparison of Muscle Strength Between Affected and Unaffected LimbsBecause application of the WISH brace directly and significantly altered the strength of muscles around the hip,9) in the present study, longitudinal change in the affected and unaffected limbs was analyzed based on the presence (Fig. 1) or absence (Fig. 2) of the WISH brace at assessment.

Time course with the hip brace at assessment of the average muscle strengths of FLEX (A), ADD (B), ABD (C), and K-EXT (D) in the unaffected (open circles) and affected (solid circles) limbs. Bars indicate standard deviations. Asterisks indicate a significant difference (P<0.05) between the average muscle strength in the affected and unaffected limbs according to the paired t-test.
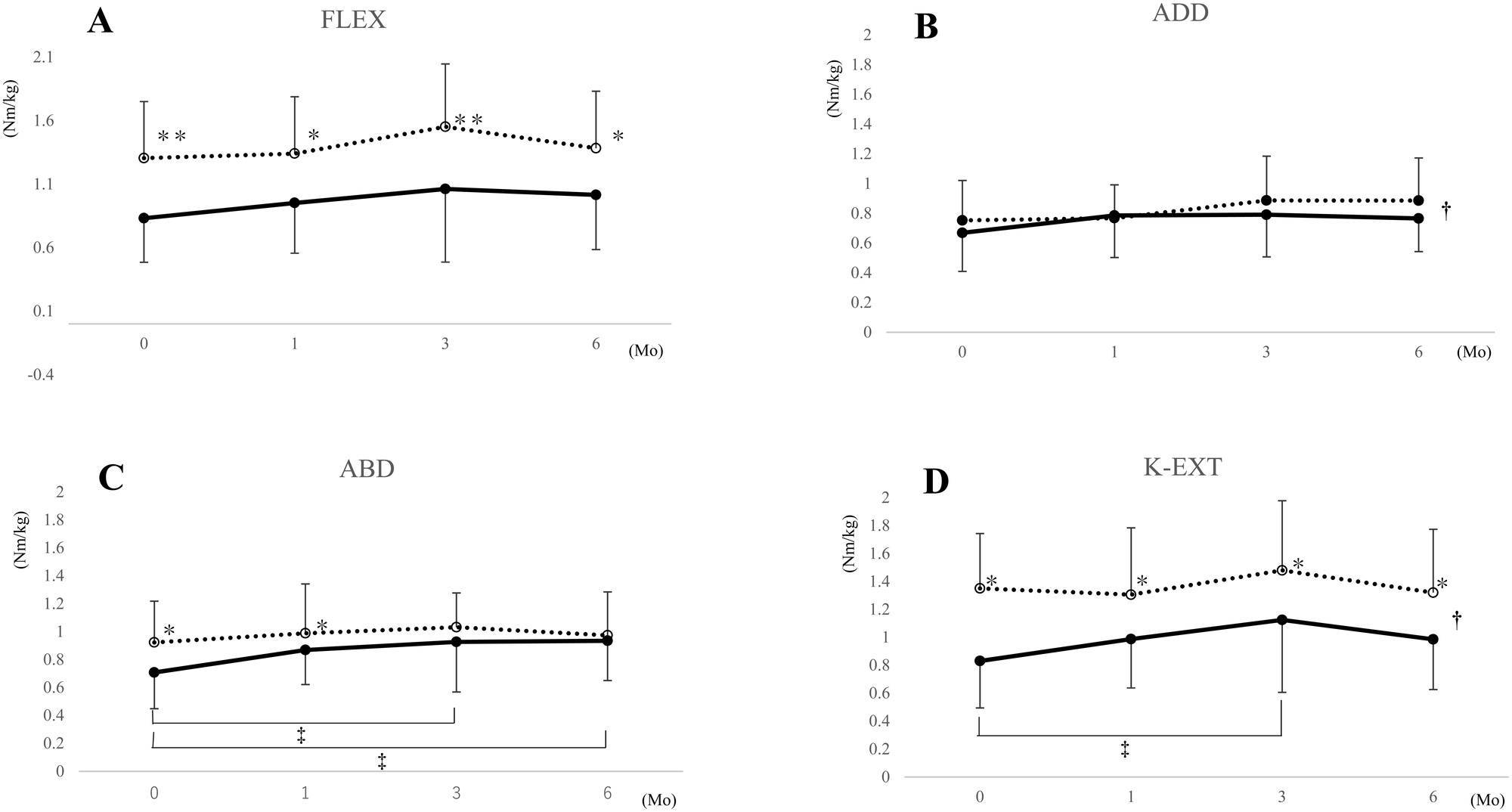
Time course without the hip brace at assessment of the average muscle strengths of FLEX (A), ADD (B), ABD (C), and K-EXT (D) in unaffected (open circles) and affected (solid circles) limbs. Bars indicate standard deviations. Asterisks indicate a significant difference between the average muscle strength in the affected and unaffected limbs according to the paired t-test (*) or the Wilcoxon signed-rank test (**). A single dagger indicates a significant difference according to the two-way repeated-measure analysis of variance (†). A double-dagger indicates a significant difference from the muscle strength at month 0 according to Dunnett’s post hoc analysis (‡).
In paired tests, the muscle strengths of FLEX and K-EXT were lower in the affected limb than in the unaffected limb for all evaluations whether measurement was performed with (Fig. 1) or without (Fig. 2) the WISH brace. The muscle strength of ABD without the WISH brace was lower in the affected limb than in the unaffected limb before bracing intervention, i.e. month 0. Although a significant difference was also observed at month 1, by month 3 the difference had disappeared (Fig. 2). No significant difference was noted in the ADD muscle strength between the affected and unaffected sides at any evaluation time with (Fig. 1) or without (Fig. 2) the WISH brace.
The two-way ANOVA results are shown in Table 2. For FLEX, ABD, ADD, and K-EXT, the unaffected limb had a significantly higher muscle strength whether measurements were performed with or without the WISH brace. Time effects were not observed. Significant leg × time interactions were observed for ADD (F3,27=3.055, P=0.045) and K-EXT (F3,27=3.481, P=0.029) muscle strength only when measurement was performed without the brace.
| Muscle | With brace | Without brace | ||
| F | P value | F | P value | |
| FLEX | 0.79 | 0.51 | 1.213 | 0.324 |
| ADD | 1.034 | 0.393 | 3.055 | 0.045* |
| ABD | 2.814 | 0.058 | 2.675 | 0.067 |
| K-EXT | 0.488 | 0.694 | 3.481 | 0.029* |
* Significant difference (P<0.05).
The characteristics of each leg (affected and unaffected) were analyzed using one-way ANOVA with repeated measurements. There was a significant change in muscle strength in ABD (P=0.035) and K-EXT (P=0.029) when measurements were performed without the WISH brace. Dunnett’s post hoc analysis revealed a significant increase (P<0.05) in muscle strength without the WISH brace at months 3 and 6 for ABD (Fig. 2C), and at month 3 for K-EXT (Fig. 2D).
This short-term longitudinal study evaluated the effects of the WISH brace on the strength of muscles around the hip and knee joints. Consistent with previous studies, hip function was significantly improved by application of the WISH brace.6,8) It is uncertain why one patient (case 6) once again had poor hip function after 6 months. Patients equipped with the WISH brace were required to walk at least 30 min every day to strengthen muscles around the hip joint required for gait.6) It is possible that this daily exercise routine may not have been closely adhered to by this patient.
The FLEX muscle strength was significantly lower in the affected limb than in the unaffected limb at all time points whether assessed with or without the WISH brace. In general, the mean hip isometric flexion strength was lower in OA patients than in controls.11,22) Furthermore, the hip isokinetic flexion strength was lower in OA patients than in controls. In OA patients, the hip flexion isometric strength was lower in the affected hip than in the unaffected hip.11,13) Furthermore, there was no significant leg × time interaction for FLEX with or without the WISH brace. Therefore, the FLEX muscle strength may be lower in the affected limb than in the unaffected limb, and is not affected by the WISH brace.
There was no significant difference between the affected and unaffected limbs in ADD muscle strength before WISH brace intervention, i.e., at month 0. These results are consistent with a previous report that adduction strength values did not differ between the affected and unaffected side in OA patients.11) In the same report, the mean hip isometric adduction strength was found to be lower in OA patients than in healthy controls.11) In contrast, another report showed that hip adduction strength was reduced in the OA limb relative to that of the healthy limb.13) The reason for these inconsistent results is unclear at present. Reduction of the adduction strength was observed when hip forces were assessed in the standing position,13) but no significant reduction was observed when hip adductor torque was tested with the subject positioned supine on a table,11) as performed in the present study. Considerable variability in outcomes in the strength of muscles around the hip joint may be explained by the difficulty in isolating specific muscles during testing or related to the choice of testing positions.22) These results suggest that ADD muscle strengths on the affected and unaffected sides are reduced by equal amounts when the muscle strength is assessed by HHD with the subject in the supine position on a table. However, repeated-measures ANOVA revealed a significant leg × time interaction in unbraced ADD strength, but there was no significant leg × time interaction when the measurements were performed with the WISH brace. Moreover, there was no significant improvement in unbraced adduction strength during the evaluation period. Taken together, ADD muscle strength may be reduced to the same extent in both affected and unaffected limbs in OA patients, and the reduced strength may be little improved by the WISH brace.
The K-EXT muscle strength was significantly lower in the affected limb than in the unaffected limb before WISH brace intervention. Previous studies have shown that the mean hip isometric knee extension strength was lower in OA patients than in controls.22) Also, in OA patients, the knee extension isometric strength was lower in the affected hip than in the unaffected hip.13) In the present study, a significant leg × time interaction was observed for K-EXT. Moreover, a significant increase (P<0.05) in muscle strength was observed at month 3 in the unbraced K-EXT. There was a synergistic effect on K-EXT muscle strength in the affected and unaffected limbs. Therefore, the WISH brace temporarily improves the K-EXT muscle strength of the affected limb via interaction with the unaffected limb.
The ABD muscle strength was significantly lower in the affected limb than in the unaffected limb before WISH brace intervention when assessed without the WISH brace. However, there was no significant difference after brace application, confirming the direct effects of the brace on the output of muscle strength.9) The present result supports the finding that the ABD strength was lower in the OA limb than in the healthy limb.13) In contrast, Arokoski et al. demonstrated that the isometric hip abduction strength did not differ between the affected and unaffected limbs.11) However, in that study, the sample size was low and there was a significant difference in isometric abduction strength values between the radiographic OA subgroups.11) On the other hand, the mean hip isometric abduction strength was lower in OA patients than in controls.11,12) In another study, patients with hip OA demonstrated 17% less hip abductor strength than healthy controls, but the difference was not significant.22) Patients with hip OA also exhibited decreased hip abduction moments during the stance phase of gait.23) These results suggest that the hip abduction muscle strength was significantly reduced, and the reduction was significantly more marked in the affected limb than in the unaffected limb, at least in patients with radiological grade I or II OA and an HHS of approximately 60.
Of note, a difference in ABD strength assessed without the WISH brace was observed using one-way ANOVA with repeated measurements. Dunnett’s post hoc analysis revealed a significant increase in muscle strength at months 3 and 6 for unbraced ABD in the affected limb. However, the significant difference between the affected and unaffected limbs had disappeared at the 3-month and 6-month follow-up assessments. With this bracing approach, continuous daily walking exercise was associated with the final outcome of hip function, suggesting a virtuous cycle in which pain reduction by the hip brace increases the active performance of daily walking and vice versa.6) On the other hand, it should also be noted that the ABD muscle strength did not exhibit synergistic effects between the affected and unaffected limbs. These results suggest that the WISH brace may improve the inherent ABD muscle strength, which is reduced in the limb affected by hip OA, independently of the unaffected limb. Therefore, this improvement of abduction muscle strength may result in improvements in hip function,6) biomechanics,10) functional mobility,8) and postural control.9)
One limitation of the present study is the relatively short evaluation period. Improvement of hip function and functional mobility is maintained for at least 12 months.6,8) Careful comparative examination of the time course of change in the strength of muscles around the hip joint and functional status would be useful to elucidate in detail the mechanisms underlying the beneficial effects of the WISH brace on hip OA. Another limitation is the measurement methods used to assess muscle strength. To assess abduction muscle strength, for example, the supine position11) was used in the present study, whereas in other studies, the standing position13) and the side lying position12,22) were adopted. To discuss the effects of hip OA on muscle strength, the measurement method should be considered carefully.
As shown in Table 3, the FLEX, ABD, and K-EXT muscle strengths were lower in the affected limb than in the unaffected limb and in the limbs of control subjects without hip OA. The ADD muscle strength, however, was reduced to the same extent in both the affected and unaffected limbs. The present study revealed that only the inherent ABD muscle strength was improved by the WISH brace, and after 3 months, the strength equaled that in the unaffected limb. This improvement in ABD muscle strength may lead to an improvement of hip function.
| FLEX | ADD | K-EXT | ABD | ||
| Before intervention (starting point of the intervention) | |||||
| Reduction against normal controla | + | + | + | + | |
| Reduction against unaffected limbb | + | – | + | + | |
| After intervention of WISH brace | |||||
| Improvement of muscle strengthc | – | – | + (temporary) | + | |
| Interaction between affected and unaffected limbsd | – | + | + | – | |
aData from previous reports.11,12,22
bData from the present study and previous reports.11,13
cData from one-way ANOVA in the present study.
dData from two-way ANOVA in the present study.
This work was supported in part by a Grant-in-Aid for Young Scientists JP18K17710 (E.S.) from the Japan Society for the Promotion of Science.
All authors declare that there are no conflicts of interest.