ABSTRACT
Objective: There are no reports describing in detail postoperative
rehabilitation after double-level osteotomy (DLO). Consequently, the establishment of a
safe and effective rehabilitation protocol is required.
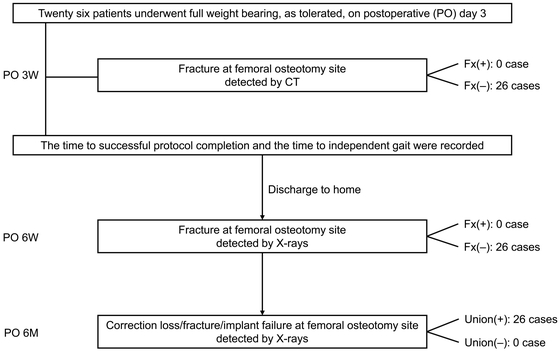
Methods: This retrospective study included 26 patients with varus knees who
underwent DLO. No patient had obvious fracture around the femoral osteotomy sites, as
evaluated using computed tomography (CT) 3 weeks postoperatively. From 3 days
postoperatively, gait training with early weight bearing was performed using our parallel
bar protocol. Range of motion exercises were permitted as tolerated. Radiological
evaluation was performed to confirm the presence or absence of fracture around the femoral
osteotomy sites using CT at 3 weeks and X-ray at 6 weeks postoperatively. X-ray imaging 6
months postoperatively indicated no femoral correction loss. Additionally, the time from
initiation to completion of the protocol and the time from initiation to achievement of
independent gait were recorded.
Results: No fractures around the femoral osteotomy sites in any patient were
found using CT 3 weeks postoperatively and X-rays 6 weeks postoperatively. There was no
correction loss at the femoral osteotomy site according to X-ray findings 6 months
postoperatively. The mean time until completion of the parallel bar protocol was 19.8 ±
6.2 (7–30) days, and that from the initiation of rehabilitation to the achievement of
independent gait was 26.8 ± 7.1 (16–45) days.
Conclusion: Patients without fracture around the femoral osteotomy site
during the rehabilitation period could achieve independent gait within an average of <1
month using the parallel bar protocol. Early weight-bearing walking and independent
walking could be achieved using this protocol.
INTRODUCTION
In patients with varus knee, both the femur and tibia are occasionally deformed. In such
cases, single osteotomy may result in extreme joint-line obliquity,1) thereby increasing the shear stress
at the joint surface2) and
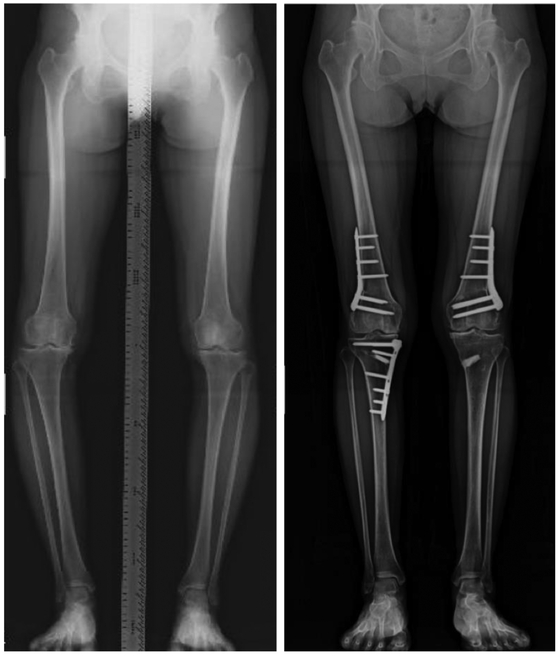
resulting in a new bony deformity. Consequently, in recent years, double-level osteotomy
(DLO) has attracted the attention of knee surgeons and has been reportedly useful in
preserving physiological articular surface tilt (Fig.
1).3,4,5)
Early weight bearing starting several days after medial, open-wedge, high tibial osteotomy
(MOWHTO) has become common and has proven to be safe.6,7,8,9) Additionally, several reports have described the timing for
initiating weight-bearing gait training in rehabilitation after distal femoral osteotomy
(DFO).10,11,12,13) In these studies, early weight-bearing gait training was not
recommended, and weight bearing was restricted for as long as 3–4 weeks after surgery.
Therefore, long-duration restricted weight bearing is an important issue.
According to our recent literature search, no reports have described postoperative
rehabilitation for DLO in detail. Therefore, a routine, safe, and effective rehabilitation
protocol is needed. In 2016, we established a standardized parallel bar protocol at our
hospital that can be used after osteotomy around the knee, including DLO. Early
weight-bearing gait rehabilitation is allowed in this protocol. Therefore, the purpose of
this study was to clarify the time required to complete our aggressive early rehabilitation
program and to clarify the time required to achieve independent walking for patients who
underwent DLO and suffered no postoperative correction loss using this rehabilitation
program.
MATERIALS AND METHODS
Patient Selection
This study was conducted at the Department of Orthopedic Surgery of Toyokawa City
Hospital. The Institutional Review Board of the Ethics Committee at our institution
approved the study protocol (approval number: 85), which was carried out in accordance
with the Helsinki Declaration, 1964. Written informed consent was obtained from all
individuals participating in this study.
Initially, 27 patients who underwent DLO between February 2016 and December 2018 were
included. However, one patient was excluded because fracture around the femoral osteotomy
site was detected by intraoperative fluoroscopy imaging and postoperative computed
tomography (CT). As a result, 26 patients were included in this study.
Indication of Surgery
The indications for DLO were patients with varus malalignment of the leg who, despite
conservative treatment, had persistent pain because of medial compartment knee
osteoarthritis. DLO combined with MOWHTO was determined when the planning of an MOWHTO
indicated a medial proximal tibia angle of more than 95° or when there was a deformity of
the lateral distal femoral angle of more than 90°. Patients with a history of infectious
knee disease, rheumatoid arthritis, or flexion contracture of more than 15° were
excluded.
Preoperative Evaluation
Patient demographics are shown in Table 1.
The severity of knee osteoarthritis was evaluated using the Kellgren–Lawrence radiographic
grading scale.14)
Table 1.
Patient demographic data
| Parameter |
All cases (n=26) |
| Sex (male/female) |
15/11 |
| Age |
60.2 ± 4.7 (53–68) years |
| Height |
159.7 ± 7.0 (148.9–179.8) cm |
| Body weight |
68.5 ± 11.0 (50.5–83.0) kg |
| Body mass index |
26.7 ± 2.9 (21.3–31.3) |
| Total correction angle |
14.2° ± 2.8° (11.2°–19.0°) |
| Femoral correction angle |
5.0° ± 1.2° (3.6°–8.2°) |
| Kellgren–Lawrence grade |
|
| Grade II |
3 cases |
| Grade III |
18 cases |
| Grade IV |
5 cases |
Values are expressed as mean ± standard deviation (range).
Surgical planning was performed with the postoperative hip–knee angle set to 2° valgus,
the medial proximal tibia angle in the range 90°–94°, and the lateral distal femoral angle
in the range 85°–89°. Routine arthroscopic debridement was performed before DLO in all
cases. No chondral transplantation was performed.
We performed lateral closed-wedge DFO first in all DLO cases using the biplanar technique
developed by a Dutch working group organized by van Brinkman et al.3,12) The contralateral side of a TomoFix Medial
Distal Femur plate (DepuySynthes; Solothrun, Switzerland) was bent to fit the lateral
femoral cortex after lateral closed-wedge DFO. This plate was
set beneath the vastus lateralis muscle, and bridging plating was performed. No suction
drain was placed, and the surgical incision was closed in layers. Following DFO, the
MOWHTO procedure described by Staubli et al. and Lobenhoffer et al.15,16) was performed to additionally correct the varus
deformity. Further, a block (Bonish, NGK SPARK PLUG, Nagoya, Japan) was prepared to fit
the pre-planned open-wedge site.
Postoperative Radiological Evaluation
Anteroposterior knee X-ray images were taken immediately after surgery to detect the
presence of any femoral osteotomy site fracture. CT (SOMSTOM Definition AS+, Siemens,
Erlangen, Germany) was performed 3 weeks after surgery to determine whether a fresh
fracture had occurred at the femoral osteotomy site. Routine radiological evaluation was
performed at 6 weeks and 6 months after surgery to assess the level of correction loss,
any newly developed fracture, or femoral implant failure (Fig. 2).
Postoperative Management
Active range of motion exercises and muscle strengthening were permitted, as tolerated,
on the first day after surgery. Early weight-bearing gait training was permitted using the
parallel bar protocol on day 3 after surgery. Load-bearing training was stopped if any
femoral fracture was detected on CT performed 3 weeks after surgery, in which case,
patients were instructed not to put their weight on the affected limb until callus
formation was observed on X-ray images.
The height of the parallel bars was set according to patient’s height, i.e., located
between the superior anterior iliac spine and the greater trochanter. The distance between
the parallel bars was consistently set at 562 mm.
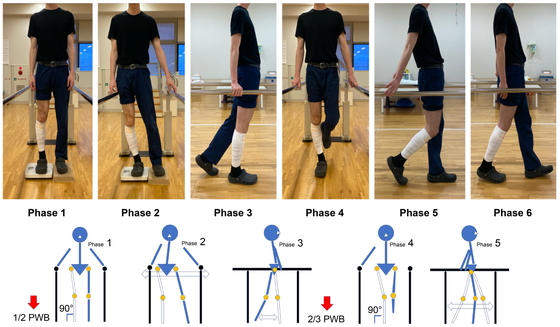
Parallel Bar Protocol
The parallel bar protocol comprised the six phases described below (Figs. 3 and 4).
Phase 1: The goal was to apply at least half partial-weight bearing (PWB) on the operated
side while standing.
Phase 2: The goal was to achieve lateral pelvic movement in a standing weight-bearing
position with, as far as possible, no twisting of the trunk, pelvis, or lower limbs and to
acquire lateral movement to the extent of the patient hitting their pelvis on the parallel
bars simply by shifting their center of gravity laterally.
Phase 3: The goal was to sense the midstance from the initial contact and to be able to
apply weight-bearing to approximately 2/3 PWB on the operated side.
Phase 4: With the aim of standing on one leg, to enable smooth transition from the
midstance to the late stance phase, the goal was to stand on one leg while holding the bar
with one hand.
Phase 5: The goal was to sense the initial swing phase from the midstance and acquire a
stable form while holding the handrail.
Phase 6: The goal was to be able to walk the length of the parallel bars without
disturbance of the gait acquired in phases 1–5.
The importance of straightening the leg in the stance phase and avoiding the stress of
femoral torsion over the entire process was emphasized to all patients. When gait
disturbance occurred, the subject was instructed to stop, and form acquisition was
reinforced.
Furthermore, when exacerbation of pain was evident, the subject was not pushed to overdo
it and was instructed not to take another step; the protocol phase was then maintained at
a level at which there was no pain exacerbation, and once the pain was relieved, the
subject proceeded to the next phase.
Clinical Evaluation
Successful completion of the parallel bar protocol was defined as the time at which the
patient accomplished phase 6, i.e., being able to walk stably the length of the parallel
bars. Independent walking was defined as the time at which the patient was able to stably
walk without any walking aid, such as a cane.
Clinical examinations comprised both subjective and objective parameters using the
Japanese Knee Osteoarthritis Measure (JKOM) and the Japanese Orthopaedic Association score
for osteoarthritic knees (JOA). Additional clinical and radiological assessments included
the range of motion and possible postsurgical correction loss. These evaluations were
conducted before surgery and 6 months postoperatively (Table 2).
Table 2.
Preoperative and postoperative evaluations
|
Preoperative |
Postoperative
at 6 months |
P-value |
| JKOM |
41.7 ± 19.3 (18–68) |
20.8 ± 7.8 (11–41) |
<0.001 |
| JOA |
74.8 ± 11.6 (50–95) |
86.5 ± 6.8 (75–95) |
<0.001 |
| Range of knee extension |
−3.3° ± 4.3° (−10° to 5°) |
−0.8° ± 1.9° (−5° to 3°) |
<0.001 |
| Range of knee flexion |
136.9° ± 12.5° (95°–150°) |
140.0° ± 8.7° (120°–155°) |
0.160 |
| Total arc of range of motion of knee |
134.1° ± 13.2° (95°–150°) |
139.5° ± 10.0° (100°–153°) |
0.015 |
| Medial proximal tibial angle |
83.3° ± 2.6° (79.8°–86.7°) |
91.6° ± 1.1° (90°–93.3°) |
|
| Lateral distal femoral angle |
91.1° ± 1.7° (88.2°–95.4°) |
85.7° ± 1° (84.1°–88.3°) |
|
| Hip–knee angle |
−8.8° ± 2.5° (−10.4° to −2.4°) |
1.8° ± 0.9° (0.8°–3.7°) valgus |
|
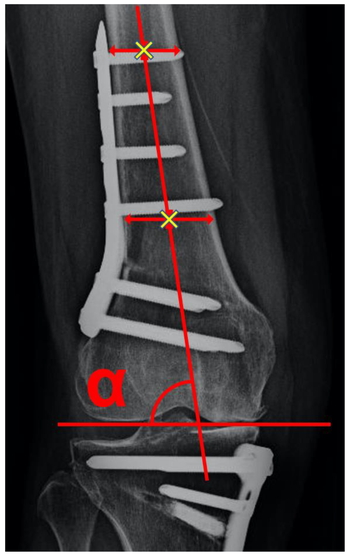
We investigated postoperative correction loss using Morland’s method.17) Two points in the middle of the
femoral medulla were marked. Then, the line connecting these two points was drawn and
extended distally to cross the articular surface line. The angle between the two lines (α
angle) was measured immediately after surgery and 6 months postoperatively. The difference
between the two α angles was defined as the correction loss (Fig. 5).
Statistical Analysis
Data are presented as the mean ± standard deviation (range). The correlation between the
time until independent gait was achieved and the body mass index (BMI) or the total
correction angle was analyzed using Spearman rank-order correlation. Comparisons of
parametric factors between groups were evaluated using paired t tests. P
<0.05 was considered significant. All statistical analyses were performed using EZR
software (http://www.jichi.ac.jp/saitama-sct/SaitamaHP.files/statmed.html).
RESULTS
No fracture or implant failure at the femoral osteotomy site was observed on radiological
evaluation using CT at 3 weeks and X-rays at 6 weeks and 6 months postoperatively in any of
the 26 patients. Furthermore, postoperative physiotherapy and weight-bearing walking
training was not delayed in any patient because of pain. To complete the parallel bar
protocol took 19.8 ± 6.2 (7–30) days after surgery. Furthermore, it took an average of 26.8
± 7.1 (16–45) days after surgery to achieve walking without any aid (Table 3). There were no significant correlations between the time
until independent gait and BMI (r=−0.114, P=0.536) or the total correction angle (r=0.324;
P=0.070). Significant improvements concerning patient-reported outcome measures and clinical
evaluations such as the JKOM (41.7 ± 19.3 vs. 20.8 ± 7.8; P <0.001), the JOA score (74.8
± 11.6 vs. 86.5 ± 6.8; P <0.001), the range of knee extension (−3.3° ± 4.3° vs. −0.8° ±
1.9°; P <0.001), and the total arc of knee range of motion (134.1° ± 13.2° vs. 139.5° ±
10.0°; P=0.015) were observed between the preoperative and 6-month postoperative
measurements. There was no significant correlation between the α angle immediately after
operation and at 6 months postoperatively (Table
4). One case of wound infection at the tibial site was diagnosed 3 months
postoperatively and was successfully treated with oral antibiotics.
Table 3.
Results of the parallel bar protocol
| All cases (n=26) |
| Number of days required for completion of the parallel
bar protocol |
19.8 ± 6.2 (7–30) days |
| Number of days required until independent gait was
achieved |
26.8 ± 7.1 (16–45) days |
| Patients with fracture observed using CT on POD 21 |
0 |
| Patients with complications on anteroposterior and
lateral X-ray images at 6 weeks and 6 months after surgery |
0 |
Values are expressed as mean ± standard deviation (range).
A mean of 35.3 days postoperatively was required before discharge; the shortest time to
discharge was post-operative day (POD) 21.
Table 4.
α angle values
|
Immediately after operation |
Postoperative
at 6 months |
P-value |
| α angle |
79.6° ± 2.7° |
79.8° ± 2.6° |
0.154 |
Values are expressed as mean ± standard deviation.
DISCUSSION
The most important findings of the present study were that load-bearing training could be
started 3 days postoperatively, and independent walking could be achieved within 1 month
using the parallel bar protocol under the condition of no fractures at the femoral osteotomy
site.
Patients who underwent this protocol were able to walk independently without any aid within
an average of 27 days after surgery. CT was performed 3 weeks after surgery, and
multi-planar reconstruction images were used to detect any fractures at the femoral
osteotomy site. We found no fractures in these sequences, and all 26 patients successfully
completed the protocol. X-ray images taken at 6 weeks and 6 months after surgery showed no
delayed union, no correction loss, and no newly developed fracture in any of the 26
patients. According to our recent literature search, this article describes one of the first
loading rehabilitation protocols for DLO.
Regarding MOWHTO, Brinkman et al. reported that TomoFix plate-fixated, open-wedge, high
tibial osteotomy allowed early full weight bearing without loss of correction. The patients
in the early weight-bearing group achieved the same clinical outcomes within a shorter time
than those following the standard rehabilitation protocol.18) To our knowledge, no report has yet described
weight-bearing gait training that commenced 3 days after DFO and DLO.1,2,3,4,5,6,7,10,11,12,13)
The benefits of shortening the unloaded period are considered to be significant in several
past reports. Early loading can reduce the risk of developing deep vein thrombosis19,20) and prevent muscle weakness. However, there is a
certain concern regarding newly developed fractures caused by loading and associated
correction loss, thereby resulting in delayed union.
Concerning the safety and efficacy of rehabilitation using parallel bars, patients with
cerebral infarction and lower limb amputation who cannot walk stably frequently undertake
rehabilitation with this equipment and are able to safely perform activities such as walking
training and unilateral leg standing; moreover, the frequency of use and the safety of
parallel bars have already been established.21)
There were no significant correlations between the time required to achieve independent
gait and BMI or total correction angle in our patient cohort. However, compared with the
preoperative stance, the postoperative stance was different after osteotomy.22) Furthermore, postoperative lower
limb alignment in most patients who underwent DFO and DLO changed significantly after
surgery. Therefore, providing a safe environment using parallel bars for these patients is
important in terms of safety. Performing gait training with simple set tasks to reacquire
smooth weight shift in each phase of standing and walking is safe and efficient for
postoperative patients. The transition distance of the parallel bar protocol is short;
consequently, it is easy for patients to perform repetitive training. Visual feedback using
a mirror and advice to the patient from the physical therapist on ideal movement patterns
are likely to improve the effectiveness of rehabilitation.23,24,25)
In our institution, parallel bar protocol rehabilitation is applied to all patients who
undergo osteotomy around the knee, regardless of the type of surgical procedure. This
protocol comprises separate training for the standing phase and the walking phase. Emphasis
is placed on straightening the leg during the entire protocol. To enable a smooth transition
to full-scale gait training, we aimed for patients to obtain a sense of the shift in their
center of gravity in an environment that reduces the fear of weight bearing and eliminates
torsion as much as possible. Biplane-cut DFOs are reportedly able to resist axial pressure
better than single-plane cut DFOs. However, biplane-cut DFOs are less resistant to torsional
forces.26) Therefore, it is
important to reduce torsional stress to prevent new fractures and postoperative correction
loss. The extent to which the lower leg is aligned vertically can be easily assessed by a
physiotherapist or other health professional, both subjectively and objectively.
There were several limitations in this study. First, it was a retrospective study at a
single institution without a control group using the same protocol. Second, it was not a
randomized trial. Randomization in postoperative rehabilitation is difficult to achieve in a
single institution. This report describes a pilot study, and the sample size was not
adequate for robust evaluation. Therefore, the results obtained in this study cannot be
applied to all osteotomy patients treated with other procedures and fixation implants.
In conclusion, gait training was performed with early weight bearing using our parallel bar
protocol, and all patients were able to acquire full-load walking without complications. In
the future, it will be necessary to increase the number of subjects and verify the safety of
this protocol.
ACKNOWLEDGMENTS
We thank Tsuneari Takahashi MD, PhD, and Crimson Interactive Pvt. Ltd. (Ulatus,
www.ulatus.jp) for their assistance in manuscript translation and editing.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Saragaglia D, Mercier N, Colle PE:
Computer-assisted osteotomies for genu varum deformity: which osteotomy for which varus?
Int Orthop 2010;34:185–190. PMID:19305996, DOI:10.1007/s00264-009-0757-6
- 2. Nakayama H, Schroter S, Yamamoto C, Iseki T,
Kanto R, Kurosaka K, Kambara S, Yoshiya S, Higa M: Large correction in opening wedge high
tibial osteotomy with resultant joint-line obliquity induces excessive shear stress on the
articular cartilage. Knee Surg Sports Traumatol Arthrosc 2018;26:1873–1878. PMID:28831525,
DOI:10.1007/s00167-017-4680-x
- 3. Nakayama H, Iseki T, Kanto R, Kambara S, Kanto M,
Yoshiya S, Schröter S: Physiologic knee joint alignment and orientation can be restored by
the minimally invasive double level osteotomy for osteoarthritic knees with severe varus
deformity. Knee Surg Sports Traumatol Arthrosc 2018. PMID:30196434,
DOI:10.1007/s00167-018-5103-5103
- 4. Schröter S, Nakayama H, Yoshiya S, Stöckle U,
Ateschrang A, Gruhn J: Development of the double level osteotomy in severe varus
osteoarthritis showed good outcome by preventing oblique joint line. Arch Orthop Trauma
Surg 2019;139:519–527. PMID:30413943, DOI:10.1007/s00402-018-3068-9
- 5. Babis GC, An KN, Chao EY, Rand JA, Sim FH,
Clinical Results: Double level osteotomy of the knee: a method to retain joint-line
obliquity. Clinical results. J Bone Joint Surg Am 2002;84:1380–1388. PMID:12177268,
DOI:10.2106/00004623-200208000-00014
- 6. Schröter S, Ateschrang A, Löwe W, Nakayama H,
Stöckle U, Ihle C: Early full weight-bearing versus 6-week partial weight-bearing after
open wedge high tibial osteotomy leads to earlier improvement of the clinical results: a
prospective, randomised evaluation. Knee Surg Sports Traumatol Arthrosc 2017;25:325–332.
PMID:25854499, DOI:10.1007/s00167-015-3592-x
- 7. Lee OS, Ahn S, Lee YS: Effect and safety of early
weight-bearing on the outcome after open-wedge high tibial osteotomy: a systematic review
and meta-analysis. Arch Orthop Trauma Surg 2017;137:903–911. PMID:28444438,
DOI:10.1007/s00402-017-2703-1
- 8. Hernigou P, Queinnec S, Picard L, Guissou I,
Naanaa T, Duffiet P, Julian D, Archer V: Safety of a novel high tibial osteotomy locked
plate fixation for immediate full weight-bearing: a case-control study. Int Orthop
2013;37:2377–2384. PMID:23974839, DOI:10.1007/s00264-013-2066-3
- 9. Takeuchi R, Ishikawa H, Aratake M, Bito H, Saito
I, Kumagai K, Akamatsu Y, Saito T: Medial opening wedge high tibial osteotomy with early
full weight bearing. Arthroscopy 2009;25:46–53. PMID:19111218,
DOI:10.1016/j.arthro.2008.08.015
- 10. Van Heerwaarden RJ, Wymenga AB, Freiling D, Staubli
AE: Supracondylar varization osteotomy of the femur with plate fixation. In: Osteotomies
around the Knee. AO and Thieme 2008;147–166.
- 11. Sherman SL, Thompson SF, Clohisy JC: Distal
femoral varus osteotomy for the management of valgus deformity of the knee. J Am Acad
Orthop Surg 2018;26:313–324. PMID:29629916, DOI:10.5435/JAAOS-D-16-00179
- 12. Brinkman JM, Freiling D, Lobenhoffer P, Staubli
AE, van Heerwaarden RJ: Supracondylar femur osteotomies around the knee. Orthopade
2014;43(Suppl 1):1–10. PMID:25331499, DOI:10.1007/s00132-014-3007-6
- 13. Willey M, Wolf BR, Kocaglu B, Amendola A:
Complications associated with realignment osteotomy of the knee performed simultaneously
with additional reconstructive procedures. Iowa Orthop J 2010;30:55–60.
- 14. Ahlbäck S: Osteoarthritis of the knee. A
radiographic investigation. Acta Radiol 1968;277:1–72. (suppl)
- 15. Lobenhoffer P, Agneskirchner JD: Improvements in
surgical technique of valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc
2003;11:132–138. PMID:12774149, DOI:10.1007/s00167-002-0334-7
- 16. Staubli AE, Simoni CD, Babst R, Lobenhoffer P:
TomoFix: a new LCP-concept for open wedge osteotomy of the medial proximal tibia – early
results in 92 cases. Injury 2003;34(Suppl 2):55–62. PMID:14580986,
DOI:10.1016/j.injury.2003.09.025
- 17. Moreland JR, Bassett LW, Hanker GJ: Radiographic
analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am
1987;69:745–749. PMID:3597474, DOI:10.2106/00004623-198769050-00016
- 18. Brinkman JM, Luites JW, Wymenga AB, van
Heerwaarden RJ: Early full weight bearing is safe in open-wedge high tibial osteotomy.
Acta Orthop 2010;81:193–198. PMID:20175658, DOI:10.3109/17453671003619003
- 19. Jacobs JJ, Mont MA, Bozic KJ, Della Valle CJ,
Goodman SB, Lewis CG, Yates AC, Jr, Boggio LN, Watters WC, III, Turkelson CM, Wies JL,
Sluka P, Hitchcock K: American Academy of Orthopaedic Surgeons clinical practice guideline
on: preventing venous thromboembolic disease in patients undergoing elective hip and knee
arthroplasty. J Bone Joint Surg Am 2012;94:746–747. PMID:22517391,
DOI:10.2106/JBJS.9408.EBO746
- 20. Sochart DH, Hardinge K: The relationship of foot
and ankle movements to venous return in the lower limb. J Bone Joint Surg Br
1999;81-B:700–704. PMID:10463749, DOI:10.1302/0301-620X.81B4.0810700
- 21. Visintin M, Barbeau H: The effects of parallel
bars, body weight support and speed on the modulation of the locomotor pattern of spastic
paretic gait. A preliminary communication. Paraplegia 1994;32:540–553.
- 22. Wang JH, Shin JM, Kim HH, Kang SH, Lee BH:
Discrepancy of alignment in different weight bearing conditions before and after high
tibial osteotomy. Int Orthop 2017;41:85–92. PMID:27535554,
DOI:10.1007/s00264-016-3279-z
- 23. Kilner JM, Paulignan Y, Blakemore SJ: An
interference effect of observed biological movement on action. Curr Biol 2003;13:522–525.
PMID:12646137, DOI:10.1016/S0960-9822(03)00165-9
- 24. Hirose S, Oouchida Y, Matsumura M, Naito E:
Viewing hand grip enhances observerʼs grip force in a body-part-specific manner.
Neuroreport 2009;20:1477–1480. PMID:19786923,
DOI:10.1097/WNR.0b013e3283322aef
- 25. Maslovat D, Hodges NJ, Krigolson OE, Handy TC:
Observational practice benefits are limited to perceptual improvements in the acquisition
of a novel coordination skill. Exp Brain Res 2010;204:119–130. PMID:20496059,
DOI:10.1007/s00221-010-2302-7
- 26. Brinkman JM, Hurschler C, Staubli AE, van
Heerwaarden RJ: Axial and torsional stability of an improved single-plane and a new
bi-plane osteotomy technique for supracondylar femur osteotomies. Knee Surg Sports
Traumatol Arthrosc 2011;19:1090–1098. PMID:21161172,
DOI:10.1007/s00167-010-1349-0