Effect of Leg Length Discrepancy on Dynamic Gait Stability
2023 Volume 8 Article ID: 20230013
Details
2023 Volume 8 Article ID: 20230013
Objectives : It is unclear whether the increased center of mass lateral shift during gait induced by leg length difference induces lateral instability. The purpose of this study was to investigate the effect of leg length discrepancy (LLD) on dynamic gait stability and the compensatory kinematic and dynamic strategies for this effect by using the extrapolated center of mass and margin of stability.
Methods : Nineteen healthy male participants walked without insoles (no LLD condition; 0 cm) and with added insoles (LLD condition; 3 cm). Kinematic and kinetic data were analyzed using a three-dimensional motion analyzer and force plates; the values were compared between the two conditions. Correlation analysis was performed on the parameters and the margin of stability and significant changes were identified.
Results: Compared with the no-LLD condition, in the LLD condition, lateral stability was maintained on both the short leg side and the long leg side. Nonetheless, changes in joint angles and muscle activity on the frontal plane were observed on the short leg side, although the correlations were not significant. On the long leg side, a moderate negative correlation was found between the lateral flexion angle of the trunk and the margin of stability (r=–0.56, P=0.011).
Conclusions: The short leg side may compensate for lateral stability by complex changes in joint angles and muscle activity, and the long leg side may compensate for lateral stability by actively adjusting the trunk lateral flexion angle.
Leg length discrepancy (LLD) is believed to result from postoperative orthopedic conditions and joint contractures.1,2) Konyves et al. used radiography to measure the leg length difference in post-arthroplasty patients and reported that 62% of all patients had leg length difference; moreover, epidemiological studies have shown that >1 in 1000 patients had an LLD of ≥2 cm.3,4) In clinical practice, patients with LLD often experience lateral body sway during the stance phase of the shorter leg, making it difficult for them to achieve independent gait. In a follow-up study of patients with late effects of poliomyelitis, the rate of falls during level gait increased threefold if the LLD exceeded 1 cm.5) This suggested that structural changes in the human body caused by LLD may be a factor in falls.
Previous studies on LLD have shown that scoliosis, the pelvic tilt angle, and the pelvic torsion angle increase in upright posture,6,7,8,9) and that the load and muscle activity of the shorter leg increase.10,11) However, the trajectory length of the center of pressure (COP) is not significantly affected by LLD.12,13) Therefore, it can be inferred that LLD has a limited effect on stability under static conditions.
Conversely, reports on dynamic stability, such as during gait, suggested that LLD may decrease stability during gait because the lateral shift of the center of mass (COM) and the variability of the distance between the COM and the inner and outer COP increase during the entire gait cycle when the leg length difference exceeds 2.5 cm.14) However, the COM’s direction and velocity must also be considered, indicating that COM is not a good indicator of stability under dynamic conditions.15) Therefore, it is not known whether LLD alters lateral stability.
Recently, Hof et al. proposed the extrapolated center of mass (XCOM) as a measure of dynamic equilibrium based on an inverted pendulum.16) As shown in Fig. 1, XCOM is the sum of the position of the COM and its traveling velocity at that time, divided by the frequency of the inverted pendulum. Since XCOM is a position coordinate on the horizontal plane, it can be projected onto the floor surface, and the margin of stability (MOS) can be calculated from the relationship of the distance between XCOM and the base of support (BOS). Thereby, it is possible to evaluate the degree to which stability is maintained with respect to the direction of movement of the center of gravity.
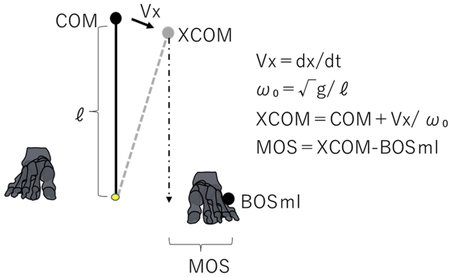
Overview of the extrapolated center of mass and margin of stability lateral distances. XCOM, extrapolated center of mass; COM, center of mass; MOS, margin of stability; Vx, center of mass velocity; g, gravitational acceleration (9.8 m/s2); l, axial length of the inverted pendulum (trochanteric height × 1.34); ωo, frequency of the inverted pendulum; BOSml, base of support in the internal and external directions.
Based on the above, we hypothesized that LLD might cause lateral instability (reduced MOS) in the stance phase of the shorter leg and used the MOS obtained using the XCOM as an index to examine the effect of LLD on gait stability. This approach may indicate compensatory movement strategies caused by LLD and whether LLD is a cause of falls.
Interested students at the International University of Health and Welfare who volunteered and gave their consent were allowed to participate. The participants were 19 healthy men (mean age, 24.8±2.8 years; mean height, 170.7±5.2 cm; mean weight, 63.6±7.9 kg; and mean body mass index, 21.8±2.2 kg/m2). In women, the markers were hidden or shifted due to chest adipose tissue. For more accurate measurements, only male participants were used in this study. Participants with an LLD ≥0.5 cm, postural abnormalities such as excessive scoliosis, or limited range of motion of any joint were excluded.
The study was approved by the Ethics Committee of the International University of Health and Welfare (approval number: 20-Io-143). The study objective and procedures were explained to the participants in detail both verbally and in writing. Informed consent was obtained in writing from all participants included in the study.
Experimental ConditionsThe participants walked naturally at optimal speed (no-LLD condition) and with an LLD of 3 cm (LLD condition), making five round trips along a 10-m gait section. The no-LLD condition was measured first, followed by the LLD condition. A 5-min rest period was allowed between tasks, and a 1-min gait practice session was conducted before the measurement in the LLD condition.
The LLD condition was achieved by inserting three 1-cm-thick insoles (Morikawa Industry, Tokyo, Japan; Morito is-Fit Extra Thick Felt; Fig. 2) into the experimental shoes (Tokutake Industry, Kagawa, Japan; Sohkai Magic Open; Fig. 3). Taking into consideration the results of a previous study14) and the deformation of the insole material, the LLD was set at 3 cm. The dominant foot was determined based on the study of Kai et al.,17) and the experimental shoe was attached to the dominant foot (right: 19 participants and left: 0 participants). Velcro was applied to the rear and dorsum of the foot to improve fixation.

Image of the insoles used in the study.

Image of the experimental shoe.
Nine Vicon cameras (Vicon Motion Systems) and four force plates (Advanced Mechanical Technology) were used for the measurements, both with a sampling frequency of 100 Hz. The positions of the reflex markers were based on the Plug-in-gait model. Markers were added to the bilateral fifth metatarsal heads to identify the lateral plantar support surface boundaries, and, to correct the knee and ankle joint axis, markers were added to the bilateral medial ankle joints and medial knee joints, making a total of 45 locations. The head marker was applied over a band, the torso marker over an upper garment (tank top), the pelvis and thigh markers over a lower garment (running tights), and the dorsal foot marker over the shoe.
Data AnalysisData processing was performed using Visual 3D analytical software (C-motion). Spatial coordinates of reflective markers and grand reaction force data were processed using low-pass filters of 6 Hz and 18 Hz, respectively. The link segment model consisted of 13 segments (head, trunk, pelvis, upper arms, forearms, thighs, lower legs, and feet). Kinematic and kinetic data were calculated from the coordinate data of each segment. Distance parameters were normalized using the height of each participant, and joint moment and joint power were normalized using body weight.
The gait cycle was divided into four phases according to the vertical component of the ground reaction force: load response (LR), single stance, pre-swing, and swing phases. Next, the peak values of hip adduction angle, pelvic tilt angle, trunk lateral flexion angle, hip abduction moment, and hip abduction absorption power were calculated for each leg in the LR phase. Additionally, the COM lateral shift, step length, step width, and gait speed were calculated.
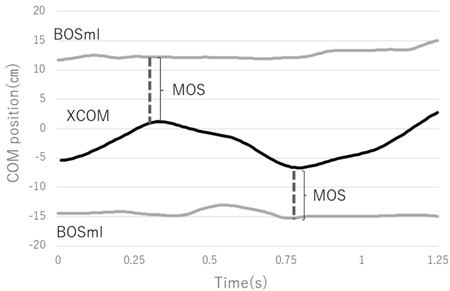
The MOS was calculated as the lateral MOS in the front–back and left–right directions with reference to a previous study18); a smaller MOS indicates greater dynamic instability. The minimum MOS distance was calculated by subtracting the fifth metatarsal head (x coordinate) position from the XCOM (x coordinate) position in the horizontal plane in the LR phase (Fig. 4). The maximum lateral XCOM movement was calculated as the distance between the XCOM (x coordinate) position at heel contact and the XCOM (x coordinate) position at maximum movement in the LR phase (Fig. 5).
Calculation of the margin of stability.
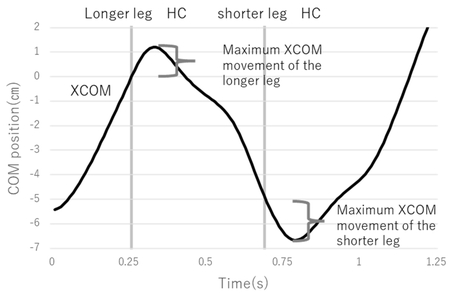
Calculation of the maximum extrapolated center of mass movement. HC, heel contact.
After confirming normality using the Shapiro-Wilk test, the COM lateral shift, MOS, maximum lateral XCOM movement, step width, step length, hip adduction angles, pelvic tilt angle, trunk lateral flexion angle, hip joint abduction moment, hip joint abduction absorption power, and gait speed were compared between the two conditions (no LLD and with LLD) using the t-test or Wilcoxon’s signed rank test, as appropriate.
Pearson’s correlation coefficient was calculated for the relationship between MOS and kinematic/kinetic parameters, and a no-correlation test was performed. SPSS Statistics Premium Pack v.28.0 (International Business Machines) was used for statistical analysis. The significance level was set at 5%.
The results are shown in Table 1. Compared with the no-LLD condition, in the LLD condition, on the shorter leg side, there were no significant differences in the MOS, maximum lateral XCOM movement, or step width. However, there was a decrease in step length (P=0.031) and hip adduction angle (P=0.003), a change in pelvic tilt to the shorter leg side in a downward direction (P<0.001), a decrease in trunk lateral flexion toward the shorter leg side (P<0.001), increased hip abduction moment (P=0.002), and increased hip abduction absorption power (P=0.009). On the longer leg side, there were no significant differences in step width or hip adduction angle, but there was an increase in MOS (P=0.006), maximum lateral XCOM movement (P<0.001), pelvic tilt to the longer leg side (P<0.001), and trunk lateral flexion toward the longer leg side (P<0.001) and a decrease in the hip abduction moment (P=0.003) and hip abduction absorption power (P=0.002). Moreover, the LLD condition showed an increase in COM lateral movement (P=0.013) and a decrease in gait speed (P=0.001).
| Parameter | Leg | No LLD | LLD | P |
| COM lateral shift (cm/Ht) | 3.0±2.0 | 4.0±2.0 | 0.013* | |
| MOS (cm/Ht) | Short | 4.3±0.9 | 4.4±0.9 | n.s |
| Long | 6.7±0.6 | 7.1±0.6 | 0.01** | |
| Maximum XCOM movement (cm/Ht) | Short | 0.9±0.2 | 1.0±0.3 | n.s |
| Long | 0.6±0.2 | 0.8±0.3 | <0.001*** | |
| Step width (cm/Ht) | Short | 8.2±1.5 | 8.5±2.0 | n.s |
| Long | 5.8±1.5 | 6.4±1.6 | n.s | |
| Step length (cm/Ht) | Short | 39.0±2.4† | 38.0±2.4† | 0.03* |
| Long | 38.6±5.3† | 41.5±8.3† | 0.01* | |
| Peak hip joint adduction angle (°: abduction+) |
Short | –2.7±1.5 | –2.0±1.7 | 0.003** |
| Long | –0.7±1.5 | –0.5±2.1 | 0.10 | |
| Peak pelvic tilt angle (°: longer leg side +) | Short | 0.6±2.3 | –1.0±2.8 | <0.001*** |
| Long | –1.5±2.5† | –3.4 ±2.7† | <0.001*** | |
| Peak trunk lateral flexion angle (°: longer leg side +) | Short | –6.0±2.2 | –4.6±2.4 | <0.001*** |
| Long | 4.0±2.4 | 5.7±2.1 | <0.001*** | |
| Peak hip joint abduction moment (Nm/kg) | Short | 0.95±1.0 | 1.03±1.0 | 0.002** |
| Long | 0.67±2.0 | 0.59±1.0 | 0.003** | |
| Peak hip joint abduction absorption power (W/kg) | Short | –0.56±2.0 | –0.64±2.0 | 0.009** |
| Long | –0.39±2.0 | –0.29±1.0 | 0.002** | |
| Gait speed (m/s) | 1.33±0.2 | 1.27±0.1 | 0.001** |
COM, center of mass; XCOM, extrapolated center of mass; MOS, margin of stability; LLD, leg length discrepancy condition; no LLD, no leg length discrepancy condition; Ht, body height; n.s, not significant.
†Wilcoxon's signed rank test.
*P<0.05; **P<0.01; ***P<0.001.
Furthermore, as shown in Table 2, correlation analysis between MOS and kinematic parameters and maximum hip abduction moment identified a significant negative correlation (r=–0.56, P=0.011) between the long leg MOS and the trunk lateral bending angle to the long leg side.
| Parameter | Condition | r | P |
| Step length (shorter leg side) |
No LLD | –0.2 | n.s |
| LLD | –0.04 | n.s | |
| Peak hip joint adduction angle
(shorter leg side) |
No LLD | 0.28 | n.s |
| LLD | 0.31 | n.s | |
| Peak pelvic tilt angle (shorter leg side) |
No LLD | 0.08 | n.s |
| LLD | 0.16 | n.s | |
| Peak trunk lateral flexion angle
(shorter leg side) |
No LLD | –0.10 | n.s |
| LLD | –0.21 | n.s | |
| Peak hip joint abduction moment
(shorter leg side) |
No LLD | –0.2 | n.s |
| LLD | –0.3 | n.s | |
| Step length (longer leg side) |
No LLD | 0.1 | n.s |
| LLD | 0.08 | n.s | |
| Peak hip joint adduction angle
(longer leg side) |
No LLD | 0.002 | n.s |
| LLD | 0.34 | n.s | |
| Peak pelvic tilt angle (longer leg side) |
No LLD | –0.2 | n.s |
| LLD | –0.02 | n.s | |
| Peak trunk lateral flexion angle
(longer leg side) |
No LLD | –0.34 | n.s |
| LLD | –0.56 | 0.011* | |
| Peak hip joint abduction moment
(longer leg side) |
No LLD | –0.1 | n.s |
| LLD | –0.35 | n.s |
*P<0.05
This study analyzed the effect of leg length difference on dynamic stability during gait using XCOM and MOS, as proposed by Hof et al.16) Furthermore, by analyzing the relationship between MOS and kinematic/kinetic parameters, strategies to compensate for stability were investigated. The hypothesis was that leg length difference may cause lateral instability (reduced MOS) in the LR phase of the short leg.
Effect of Leg Length Difference on Dynamic Stability of the Short Leg SideFirst, the lateral shift of the COM increased when there was a leg length difference compared to no leg length difference. This is consistent with the results of a previous study,14) but the MOS on the short leg side showed no significant difference compared to the no LLD condition, suggesting that lateral stability may be maintained during the short leg side LR phase, despite the increase in COM lateral shift during the entire gait cycle. Bruijn et al. reported that instability could be avoided by adjusting the placement of the feet during gait.19) Therefore, our study participants might have avoided instability by compensatory increases of the step width; however, no significant change in step width was observed in either condition. It is also possible to avoid instability by adjusting the velocity of the shorter leg movement in the lateral direction during the LR phase; however, we found no significant changes in the maximum lateral XCOM movement in either condition.
Nonetheless, a significant decrease in step length was observed compared to the no LLD condition, as in the previous study.20) Hak et al.21) reported that step frequency increased with increased instability during gait, suggesting that step length reduction may avoid instability during short leg side stance because the leg length difference because the leg length difference increases COM movement in the lateral directions. However, there was no significant correlation between MOS and step length. Consequently, it was suggested that step length reduction may not be a strategy to compensate for lateral stability.
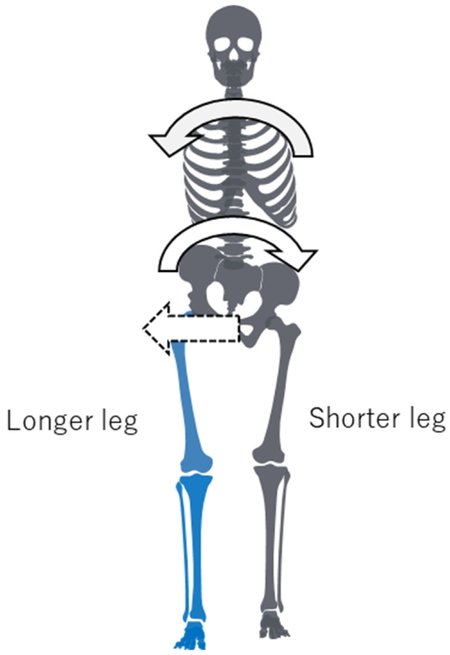
On the shorter leg side, compared with the no-LLD condition, we found a significant decrease in the hip adduction angle during the LR phase, a change in pelvic tilt to the shorter leg side in a downward direction, and a significant decrease in trunk lateral flexion to the shorter leg side in the LLD condition. In general, during the LR phase, the pelvis is elevated approximately 5° to the stance side, and the trunk is laterally flexed also to the stance side,22,23) suggesting that our study participants were using an unusual postural balance strategy (Fig. 6). In addition to these changes in joint angles, there was an increase in hip abduction moment and hip abduction absorption power during the short leg LR phase, but correlation analysis with MOS of the short leg showed no significant correlation.
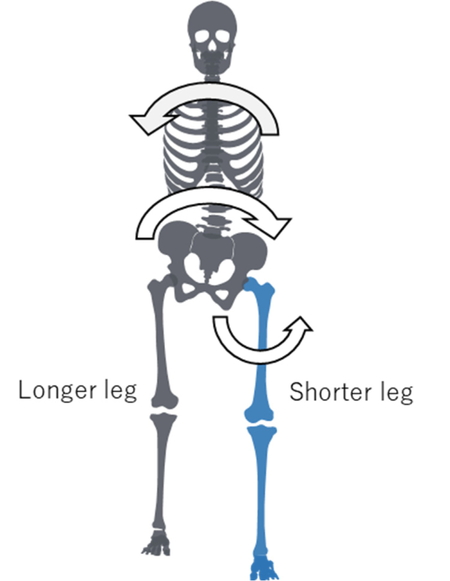
Compensatory strategies for the shorter leg.
These findings suggest that stability may be guaranteed during the LR phase of the short leg side. However, previous studies have shown that the strategy to maintain balance is to rotate the body segment in the direction opposite to the external force24) and to increase the muscle activity of the hip peroneal muscles.25) Therefore, it is possible that lateral stability is compensated for by a combination of these strategies of changing joint angles and increasing muscle activity around the hip joint.
Effect of Leg Length Difference on Dynamic Stability of the Long Leg SideThe MOS of the long leg and XCOM movement significantly increased compared to the no LLD condition, suggesting that the long leg may have increased angular momentum of the COM while being more stable in the lateral direction than in normal gait.
Since MOS is the difference between XCOM and BOS, it was considered possible that the position of BOS was adjusted to be more lateral. However, in this study, there was no significant change in step width in the presence of LLD. Although step length was significantly increased compared to the no-LLD condition, no significant correlation with MOS was observed, suggesting that there was little relationship with lateral stability.
In contrast, the changes in joint angles during the long leg LR phase showed a significant increase in pelvis elevation to the long leg side and trunk lateral flexion to the long leg side (Fig. 7) compared to the no-LLD condition, and a moderate negative correlation was observed between the trunk lateral flexion angle and MOS. It is known that the distribution of body weight on the short leg increases during the bilateral leg support phase in the case of LLD14); therefore, it is possible that the lateral flexion angle of the trunk was adjusted to counter the rotational moment toward the short leg caused by the shift in COM toward the inside of the body during heel contact when the long leg becomes the forward limb, thereby stabilizing postural balance.
Compensatory strategies for the longer leg.
Furthermore, the hip abduction moment and hip abduction absorption power were significantly reduced in the LLD condition, but no significant correlation was found between hip moment and MOS. A study26) comparing hip abductor muscle tension under normal gait and trunk lateral flexion conditions using a musculoskeletal computer model reported a significant decrease in hip abductor muscle tension under trunk lateral flexion conditions, suggesting that compensation of lateral balance by trunk lateral flexion results in decreases in hip abduction moment and hip abduction absorption power.
These results suggest that during the LR phase of the long leg side, the patient does not use a balancing strategy by adjusting muscle activity, but actively adjusts the trunk lateral flexion angle and rotates the body segment in opposition to external forces to compensate for lateral stability while reducing the burden on the hip muscles that are needed to stabilize the pelvis.
Effect of Leg Length Difference on Gait SpeedThe gait speed in the LLD condition was significantly lower than that in the no-LLD condition, which was consistent with the findings of McDonald et al.27) In general, it is believed that during gait, the positional energy that is maximized during the monopedal support phase is converted to kinetic energy during the bipedal support phase, resulting in efficient and repeated forward motion.28) However, it is known that in gait with LLD, the knee joint extension moment decreases from the early to mid-stance of the shorter leg side,22) resulting in asymmetry of lower limb joint moments and power20); consequently, there is a possibility of a left–right difference in the potential energy produced between the two lower limbs.29) Therefore, it is possible that the LLD in this study inhibited efficient forward propulsion, resulting in an increase in the COM lateral shift and a decrease in gait speed.
This study had some limitations. Because the study was conducted on healthy young men, the effects of age and sex were not examined. Moreover, this study was conducted using healthy participants to allow comparisons with previous studies; consequently, it is possible that the results may differ in actual patients with LLD. Furthermore, because there are various factors that cause LLD, in the future, examining such factors may be necessary, focusing on the characteristics of the mechanisms by which they occur.
The results of this study suggest that structural changes resulting from LLD reduce gait speed and increase the COM lateral shift but retain lateral stability in both the short and long lower extremities. However, it was suggested that the short leg side may compensate for lateral instability by generating a combination of strategies that alter hip, pelvis, and trunk angulation and increase periprosthetic hip muscle activity. There was also a significant negative correlation between MOS and trunk lateral flexion on the long leg side. Therefore, the stability toward the short leg side may be compensated by adjusting the trunk lateral flexion angle during the LR phase, when the long leg side becomes the forward limb. In summary, we found that it is important to maintain the joint range of motion and muscle strength in the trunk in patients with LLD to stabilize lateral balance. In addition, instability may occur in patients with functional limitations to their compensation strategy.
We would like to thank all study participants for their cooperation in conducting this study. We are also grateful to Dr. Akira Kubo and Dr. Makoto Tamari for their guidance and Dr. Sumiko Yamamoto, Dr. Yusuke Maeda, and Dr. Mizuho Ota for their advice on measurement and analysis using the three-dimensional motion analysis device.
The authors declare that they have no conflicts of interest.