ABSTRACT
Background: There are numerous etiologies relating to physeal
arrest. The clinical manifestations of physeal arrest may include limb length
discrepancy (LLD) and bone malalignment, especially in younger children with
more growth ahead of them.
Case: We performed three-dimensional gait analysis (3DGA) four times
over a 13-year period in a boy aged from 9 to 22 years who was suffering from
LLD and genu valgum. At the final follow-up, the patient’s LLD and coronal
malalignment had been ameliorated on radiographic findings after multiple
corrective surgeries, including the use of external fixation. In 3DGA, the
patient’s Gait Profile Score (GPS) at age 12.5 years was poorest at 12.4°,
improving to 8.4° at age 22.3, a change of 2.5 times the minimal clinically
important difference. Assessment of kinetics showed a mean knee coronal moment
during the stance phase of 0.17 (varus) and 0.20 (valgus) Nm/kg at the ages of
18.6 and 22.3 years, respectively. Importantly, this revealed significant
improvement from the perspective of knee coronal moment (P
<0.001).
Discussion: This is the first report of long-term follow-up 3DGA
using GPS in a patient undergoing multiple corrective surgeries for LLD and genu
valgum. Although both LLD and genu valgum improved, gait function did not
normalize. This shows that focusing on radiographic findings alone may not lead
to improved patient outcomes and indicates the value of gait function
assessment.
INTRODUCTION
The etiologies of physeal arrest include infection, tumor, and trauma such as sports
injuries.1,2) Clinical manifestations of physeal arrest may
include limb length discrepancy (LLD) and bone malalignment, especially in younger
children with more growth ahead of them. This report describes a case of early
physeal arrest of the left distal femur and proximal tibia. Long-term follow up with
instrumented three-dimensional gait analysis (3DGA) data was done concurrently with
several orthopedic surgeries on four different occasions over a 13-year period
(patient age: 9–22 years). This report was approved by the Institutional Review
Board of the institution where the surgeries and measurements were performed
(Hokkaido Medical Center for Child Health and Rehabilitation; Approval number and
date: 42-2, May/17/2021). The patient, after reaching the age of majority, provided
written consent for this article.
CASE
An 8-year-old boy presented at an orthopedic clinic complaining of right knee pain
after skiing, but without any left knee symptoms. Bilateral knee joint evaluation
revealed asymptomatic abnormal radiographic findings on the left distal femur and
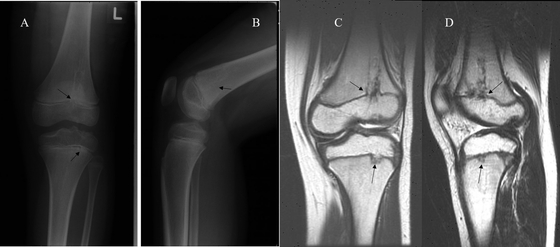
proximal tibia, but no restrictions in lower limb range of motion. The physician
made a diagnosis of premature physeal arrest and opted for observation, anticipating
future corrective surgery. (Fig. 1
A, B) One year later, the patient presented again,
complaining of abnormal gait, and was first referred to our facility. The patient
had no objective physical findings and participated in karate team activities. Long
limb alignment radiographs revealed a 0.7-cm LLD with the left lower limb being
shorter. Further radiographic and magnetic resonance imaging of the left knee showed
linear partial physeal bars at the distal lateral femur and proximal lateral tibia
(Fig. 1 C,
D).
Several orthopedic surgeries were performed to correct the left lower limb
deformities. At age 9.3 years, the patient underwent arthroscopic resection of the
femoral bar and autologous fat transfer based on the work of Saisu et al.3); we opted for
observation of the proximal tibia, considering the small lesion size and risk of
complications. Distal femoral bar resection failed to prevent subsequent deformities
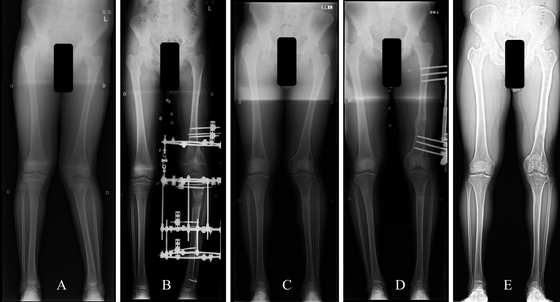
from developing. At age 11.3 years, the patient underwent an alignment osteotomy
plus lengthening using an Ilizarov External Fixator (Smith & Nephew, Memphis,
TN, USA) to correct a progressive valgus deformity of 22°, and an LLD of 2.5 cm.
(Fig. 2A,
B). When the patient was 12.5 years old, we operated to correct
recurrent genu valgum via medial hemi-epiphysiodesis with staples (Smith &
Nephew) in the left distal femur. Follow up revealed failure of this procedure,
possibly resulting from insufficient remaining growth. Lastly, at age 18.6 years
(skeletal maturity), the patient underwent femoral lengthening (LLD 2.9 cm) and genu
valgum (13° valgus) correction osteotomy using the Limb Reconstruction System
(Orthofix Srl, Verona, Italy) (Fig.
2C, D). At final follow-up (age 22.3 years), genu valgum
(3°) and LLD (0.2 cm) had improved compared with the worst values as measured at
18.6 years (Fig.
2E). Despite the improvement in lower limb alignment, left
knee flexion was restricted to 118°, without extension lag. Although the patient was
unable to sit on his knees, he did not manifest any other restriction of range of
motion at the hip or ankle joint; there were no significant differences in lower
limb ranges of motion between the affected and unaffected sides. There was no
significant decline in muscle strength on the involved side, and the patient did not
report any knee pain during participation in high stress activities such as
recreational football. The circumference of the left thigh was 2 cm less than the
uninvolved side.
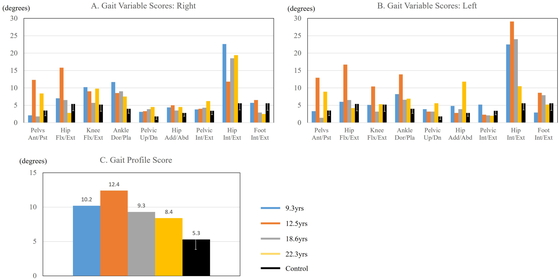
Multiple instrumented 3DGA data were used to assess gait function prior to the
first, third and fourth operations, via quantitative scoring systems, i.e.,
Movement Analysis Profiles (MAPs), including the Gait Variable Scores (GVS) and
Gait Profile Score (GPS).4,5) 3DGA data were collected using an MX-F20 camera
(Vicon, Oxford, UK) with two force plates (AMTI, Watertown, MA, USA). In the
zero position, we manually maintained the neutral position prior to the
examination because the patient suffered from lateral laxity of the left knee.
Kinematic data and kinetic data were calculated using Plug-in Gait (Vicon). MAP
visually represents kinematic data with simple bar charts, providing improved
readability over conventional graphs. The constituents of MAP are GVS and GPS,
which were described by Baker et al.6) Both GVS and GPS are measured in degrees. On a
GVS chart, taller bars indicate greater deviation from the control for each
joint motion, whereas higher bars on GPS show reduced function in overall gait
pattern. GVS is the root-mean-square difference of an individual’s kinematic
data, consisting of nine kinematic parameters: pelvic tilt, pelvic obliquity,
pelvic rotation, hip flexion, hip abduction, hip rotation, knee flexion, ankle
dorsiflexion, and foot rotation, which are compared with a control dataset (38
normative children, aged less than 18 years, collected from 2005 to 2007 in
Melbourne7)). GPS is calculated as the root-mean-square average
of GVS variables. Furthermore, to confirm the effectiveness of coronal
realignment, we investigated the valgus/varus moment of the left knee during the
stance phase using kinematic analysis. Statistical analysis employed a paired
t-test, performed using SPSS ver. 24 for Windows (SPSS Inc, Armonk, NY, USA). P
< 0.05 was considered statistically significant.
The patient’s GPSs were 10.2° and 12.4° at ages 9.3 and 12.5 years, respectively.
On GVS for hip rotation at the age of 12.5, the left side demonstrated greater
compensatory motions than the right side. The same finding was revealed at the
age of 18.6, with a GPS of 9.3°. At the final follow-up, GPS had improved to
8.4° (Fig.
3–5). Kinetic assessment showed mean knee coronal moment
during the stance phase of 0.12 (valgus), 0.04 (valgus), 0.17 (varus), and 0.20
(valgus) Nm/kg at the ages of 9.3, 12.5, 18.6, and 22.3 years, respectively.
Importantly, the latest instrumented 3DGA assessments revealed significant
improvement from 0.17 (varus) to 0.20 (valgus) Nm/kg (P
<0.001). However, despite the improvement in lower limb alignment, the gait
pattern continued to deviate from typical gait, especially for right Hip Int/Ext
and left Hip Add/Abd.
DISCUSSION
This report presents a patient with premature partial physeal arrest of the left
distal femur and proximal tibia, leading to LLD and genu valgum and consequent gait
abnormalities. Ecklund et al.8) reported that posttraumatic physeal bars accounted
for 70% of all cases of early physeal arrest, and of 111 cases, 37 lesions were
located at either the distal femur or proximal tibia. Although the specific etiology
was not identified in the current case, the mirror lesions on both sides of the left
knee joint and the vulnerable location suggest association with minor trauma.
Gordon et al.9) suggested
that a LLD > 2 cm could lead to hip, knee, and low back pain. Although there are
several reports of 3DGA in LLD cases, diverse conclusions regarding compensatory
mechanisms have been reported.10,11,12,13) Aiona et al.12) demonstrated that the site of the lesion
causing LLD influenced the type of compensation; patients with femoral shortening
tended to have increased stresses/loading on their ankles, whereas those with tibial
shortening tended to compensate with pelvic obliquity. 3DGA before final correction
revealed compensations at the hip joint rather than at the ankle. Furthermore,
compensation was predominantly on the involved side.
Although healthy knees demonstrate internal valgus moments in the stance phase,
suggesting that the third finding of this study was abnormal, few previous reports
have used 3DGA for the assessment of genu valgum, unlike LLD.14,15,16) Stevens et
al.15)
demonstrated significant clinical improvement among genu valgum patients who
underwent hemi-epiphysiodesis, finding that hip coronal kinematics improved, whereas
sagittal plane kinematics and kinetics were not affected. Similarly, Farr et
al.14)
described children with genu valgum who manifested decreased knee valgus moment and
increased external hip rotation. Comparison between our single case and those of
Farr et al.14) is
difficult, because the latter excluded patients with LLD > 1 cm. In this case,
increased left hip external rotation at 18.6 years was primarily influenced by genu
valgum rather than by LLD. Böhm et al.16) concluded that changes in dynamic load can be
predicted from changes in static alignment. This complicated case combined LLD and
genu valgum, and the patient did not demonstrate normal gait parameters despite
improvement of static lower limb alignment. The patient’s previous operations may
have caused some lasting adverse effects; in particular, the two external fixator
corrections. These repeated surgical procedures may have affected body composition
asymmetry, flexibility of the iliotibial band, and gait function.
Baker et al.6)
established GVS and GPS as quantitative scoring systems, supplementing traditional
kinematic curves. These tools are useful in evaluating neuromuscular patients with
gait disturbance.4,5) We are not aware of any reports assessing LLD
patients using 3DGA with GVS and GPS. In our patient, the observed GPS change
corresponded to 2.5 times the minimal clinically important difference of
1.6°,6) compared
to the poorest value of 12.4° at the age of 12.5 years. MAP does not include knee
valgus/varus kinematics or kinetics data, nor does it differentiate between the
stance phase and swing phase. However, because MAP was designed to summarize much of
the information contained within kinematic data, it facilitates quick assessment of
compensation strategies without requiring interpretation of multiple kinematic
plots. This may allow a wider range of clinicians to apply 3DGA, thereby avoiding
the barriers posed by traditional kinematic graphs.
In conclusion, improvement of both LLD and genu valgum did not lead to normalized
gait function. There are several reports relating to gait disturbance with either
LLD or genu valgum; however, we believe that this is the first long-term case report
and follow-up with 3DGA that included MAP for a patient diagnosed with unilateral
premature partial physeal arrest who underwent multiple surgical corrections.
Although MAP has limited use when planning surgical procedures, interpretation of
kinematics and kinetics plots together with MAP may facilitate understanding of
compensatory motions. This case illustrates the fact that improved radiographic
findings may not correlate with improved gait function, thereby indicating the
importance of 3DGA.
ACKNOWLEDGEMENTS
The authors thank Kyouji Kakimoto, Jun Hasegawa, and Daiki Shimotori, clinical
examiners in our gait lab, for assistance with motion analyses, and Allen Paul
Heffel for English language editing.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Herring JA: Tachdjian’s Pediatric
Orthopaedics. 5th ed. Philadelphia: Elsevier Saunders; 2013. pp.
806-869.
- 2. Weinstein SL, Flynn JM, Crawford H: Lovell
and Winter’s Pediatric Orthopaedics. 8th ed. Philadelphia: Wolters Kluwer; 2020.
pp. 1296-1341.
- 3. Saisu T, Kamegaya M, Watanabe A, Ochiai
N, Takahashi K: Endoscopic surgery for chronic osteomyelitis extending across
the physis. A report of two cases. J Bone Joint Surg Am 2008;90:1744–1750.
PMID:18676907, DOI:10.2106/JBJS.G.01114
- 4. Fujita H, Fusagawa H, Nishibu H, Nosaka
T, Matsuyama T, Iba K, Yamashita T: Motion analysis and surgical results of
anterior transfer of flexor hallucis longus for equinovarus gait in children
with hemiplegia. J Orthop Sci 2021;26:441–447. PMID:32600904,
DOI:10.1016/j.jos.2020.05.001
- 5. Fusagawa H, Fujita H, Matsuyama T, Himuro
N, Teramoto A, Yamashita T, Selber P: Gait profile score and gait variable
scores in spina bifida. J Pediatr Orthop B 2022;31:e251–e257. PMID:34028379,
DOI:10.1097/BPB.0000000000000877
- 6. Baker R, McGinley JL, Schwartz M,
Thomason P, Rodda J, Graham HK: The minimal clinically important difference for
the Gait Profile Score. Gait Posture 2012;35:612–615. PMID:22225850,
DOI:10.1016/j.gaitpost.2011.12.008
- 7. Baker R, McGinley JL, Schwartz MH, Beynon
S, Rozumalski A, Graham HK, Tirosh O: The gait profile score and movement
analysis profile. Gait Posture 2009;30:265–269. PMID:19632117,
DOI:10.1016/j.gaitpost.2009.05.020
- 8. Ecklund K, Jaramillo D: Patterns of
premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol
2002;178:967–972. PMID:11906884, DOI:10.2214/ajr.178.4.1780967
- 9. Gordon JE, Davis LE: Leg length
discrepancy: the natural history (and what do we really know). J Pediatr Orthop
2019;39(Supplement 1):S10–S13. PMID:31169640,
DOI:10.1097/BPO.0000000000001396
- 10. Kaufman KR, Miller LS, Sutherland DH:
Gait asymmetry in patients with limb-length inequality. J Pediatr Orthop
1996;16:144–150. PMID:8742274,
DOI:10.1097/01241398-199603000-00002
- 11. Walsh M, Connolly P, Jenkinson A, O’Brien
T: Leg length discrepancy — an experimental study of compensatory changes in
three dimensions using gait analysis. Gait Posture 2000;12:156–161.
PMID:10998613, DOI:10.1016/S0966-6362(00)00067-9
- 12. Aiona M, Do KP, Emara K, Dorociak R,
Pierce R: Gait patterns in children with limb length discrepancy. J Pediatr
Orthop 2015;35:280–284. PMID:25075889,
DOI:10.1097/BPO.0000000000000262
- 13. Khamis S, Carmeli E: Relationship and
significance of gait deviations associated with limb length discrepancy: a
systematic review. Gait Posture 2017;57:115–123. PMID:28600975,
DOI:10.1016/j.gaitpost.2017.05.028
- 14. Farr S, Kranzl A, Pablik E, Kaipel M,
Ganger R: Functional and radiographic consideration of lower limb malalignment
in children and adolescents with idiopathic genu valgum. J Orthop Res
2014;32:1362–1370. PMID:25042523, DOI:10.1002/jor.22684
- 15. Stevens PM, MacWilliams B, Mohr RA: Gait
analysis of stapling for genu valgum. J Pediatr Orthop 2004;24:70–74.
PMID:14676537, DOI:10.1097/01241398-200401000-00013
- 16. Böhm H, Stief F, Sander K, Hösl M,
Döderlein L: Correction of static axial alignment in children with knee varus or
valgus deformities through guided growth: does it also correct dynamic frontal
plane moments during walking? Gait Posture 2015;42:394–397. PMID:26159802,
DOI:10.1016/j.gaitpost.2015.06.186