ABSTRACT
Objectives: Coronavirus infection 2019 (COVID-19) is an indication
for rehabilitation medicine, especially in severe cases. However, there has been
no system analysis of safe and continuous provision of medical rehabilitation
for COVID-19 patients. The aim of this study was to confirm the effectiveness of
rehabilitation for severe COVID-19 and to analyze the optimization of the
medical rehabilitation system using the Functional Resonance Analysis Method
(FRAM).
Methods: The subject of the analysis was the medical rehabilitation
system itself, which had been implemented by the Rehabilitation Center of our
hospital in response to the increased number of COVID-19 patients. In the FRAM
analysis, Functions were identified, and their relationships were examined.
Functions were established using a hierarchical cross-check by the authors.
Patient outcomes resulting from optimization of the rehabilitation system were
length of hospital stay, patient independence in daily living, and
rehabilitation-related medical costs, and these were statistically
validated.
Results: In repeated optimizations of the rehabilitation system, the
main issues were “handling of infected patients and isolation of usual clinical
practice,” “staff rotation,” and “remote consultation”. The modification of the
medical rehabilitation system was associated with shorter hospital stays,
shorter periods of time without prescription, faster improvement in independence
of daily living, and lower rehabilitation-related medical costs.
Conclusions: Optimization at each stage of medical rehabilitation
resulted in positive effects on patient outcomes. FRAM is useful for identifying
and the optimization of key functions.
INTRODUCTION
The SARS-CoV-2 virus, which causes coronavirus disease 2019 (COVID-19), has affected
more than 600 million people.1) Because of its high infectivity, healthcare
facilities are required to treat patients with COVID-19 separately from other
patients, and healthcare workers must wear personal protective equipment (PPE) to
reduce the risk of infection. Although more than 60% of COVID-19 cases are
considered mild,2) some
cases are very severe and require ventilatory management and extracorporeal membrane
oxygenation. In such severe cases, the use of sedation to prevent lung
injury3)
associated with spontaneous breathing and the effects of immobility have been found
to reduce systemic skeletal muscle function4) and cognitive function5) in approximately 80% of patients. These
functional declines have been reported previously as intensive care unit-acquired
weakness,6)
indicating the need for early physical therapy and medical rehabilitation in the
intensive care unit.7)
Our long-term acute care hospital provides emergency and acute care in a region with
a population of 1.7 million people. Beginning in March 2020,8) only patients with
COVID-19 who were critically ill or had the potential to become critically ill were
admitted and provided with medical care, and, for their reduced physical mobility,
medical rehabilitation has been provided since May 2020. Rehabilitation specialists
such as physical therapists, occupational therapists, and speech/language/hearing
therapists provide exercise training, assist in the practice of basic movements and
daily living, and, in some cases, unmasking and various oral and pharyngeal motor
assessments. Although the rehabilitation professionals wear PPE when treating
patients with COVID-19, the combination of the infectivity of the virus and the
contact density (a concept combining contact time, distance, and aerosol exposure)
between the rehabilitation specialists and the patient may increase the risk of
infection for the therapist.9) Although some reports recommend specific PPE,
protection against the high infectivity of newly emerging strains, the proximity of
therapist and patient, and the contact time between them have not been
demonstrated.10,11) In addition, there has been no verification of the
ability of medical rehabilitation practices to ensure the safety of patient
independence in daily living or its economic sustainability.
The Functional Resonance Analysis Method (FRAM)12) is a systems analysis method that has been
developed and applied in medicine to analyze the occurrence of accidents and solve
clinical problems,13)
including those that have risen during the COVID-19 pandemic.14) During the spread of
SARS-CoV-2 virus infection, we implemented optimal system modifications for several
variables (number of patients, severity of illness, SARS-CoV-2 virus infection
potential, staff health status). As a result, some patient outcomes and staff
adaptations were observed. However, there has not been sufficient analysis of the
disadvantages and advantages of the system optimization with repeated modifications.
We considered that FRAM would be useful for the analysis of our system of safe
rehabilitation medicine with a high density of patient contact.
The purpose of this study was to identify ways to optimize medical rehabilitation
during a period of increased COVID-19 cases using FRAM and to help prepare for
future expansion of the infection. The aim of this study was to confirm the
effectiveness of rehabilitation for severe COVID-19 and to analyze the optimization
of our medical rehabilitation system that led to this effectiveness.
MATERIALS AND METHODS
This retrospective observational study was approved by the Ethics Committee of Hyogo
Medical University (registration number 3866) and was described according to the
SQIURE (Standards for Quality Improvement Reporting Excellence) 2.0
checklist.15)
The Rehabilitation Department consisted of 5 rehabilitation physicians, 4 residents,
36 physical therapists, 14 occupational therapists, 7 speech therapists, and 1
support worker. During the analysis process, physicians in the Department of Medical
Safety and Quality Control provided guidance on methods of analysis and
validation.
Retrospective FRAM Model Construction
The FRAM model was constructed according to the procedure described by
Hollnagel,16) as follows: 1) identification and description
of Functions by hierarchical task analysis, 2) identification and description of
aspects of Functions, 3) creation of a coupled model between Functions, and 4)
system analysis based on FRAM. Hierarchical task analysis was performed
according to the following procedures: 1) description of tasks actually
performed during usual medical rehabilitation from referral of patients to
consultation by rehabilitation doctors, 2) description of tasks actually
performed during therapy implementation, 3) description of tasks related to
assignment to dedicated beds and modified consultation procedures for COVID-19
cases, and 4) tasks related to the established and modified dedicated therapist
system. The functions were described by the following procedures to verify
objectivity and validity: 1) author N.S. described the above Functions, 2)
co-authors A.Y., Y.M. (physical therapist), Y.U. (rehabilitation doctor) checked
the validity of the described Functions and sent them back to N.S., 3) N.S.
revised and re-created the Functions, 4) steps 2 and 3 were repeated, and 5)
co-author K.T. (a medical quality control specialist) checked the validity of
the Functions.
Participants and Data Collection
Eligible patients were COVID-19 patients who underwent rehabilitation between May
2020 and June 2022. To understand the characteristics of the patients, the
following medical record data were extracted: age, sex, height, Body Mass Index
(BMI), disease severity indices, period of hospitalization, unprescribed periods
of medical rehabilitation, and rehabilitation-related medical expenses.
Measurements of the Functional Independence Measure (FIM),17) which is an index
of independence in the activities of daily living (ADLs), were performed at
beginning of rehabilitation and at discharge from hospital. FIM was used as the
outcome measure of the rehabilitation intervention. Disease severity was rated
in terms of the Acute Physiology and Chronic Health Evaluation (APACHE) II
score,18)
the Sequential Organ Failure Assessment (SOFA) score,19) and the quick COVID-19 Severity
Index (qCSI).20)
Data accuracy was ensured by using the following protocols. The authors were not
involved in the measurements of BMI or severity index and did not have the
authority to determine the date of admission or discharge of the patients. The
assessors of the FIM were included as co-authors, but the first author was not
involved in the assessment and the co-authors were not involved in the
statistical analysis.
Rehabilitation Treatment
COVID-19 patients with severe disease or at risk of severe disease were admitted
to our hospital. The main rehabilitation prescriptions included respiratory
physiotherapy, training on the bed, mobilization, training in ADLs, and
screening evaluation of swallowing function. Patients who met the
criteria21)
for intubated ventilation were actively treated in the supine position along
with ventilatory management.21) In the bed-bound phase, strength training was
performed using weights, elastic bands, and manual resistance. When the patient
was able to get out of bed, mobilization was performed as much as possible with
care taken to avoid exercise-induced hypoxemia.22) Mobilization included rolling,
sitting up, sitting, standing up, standing, marching, transfer to a wheelchair,
gait with various aids, and free gait in stages.8) Muscle strength training after
reacquisition of standing was combined with training that used body weight, such
as squats and calf raising.
Statistical Analysis
Differences in patient variables for each period of time were examined for the
modified rehabilitation systems. One-way analysis of variance and Tukey’s post
hoc test were used to assess differences in age, BMI, hospitalization period,
unprescribed rehabilitation periods, rehabilitation-related medical expenses
(RME), and RME relative to rehabilitation period. The Kruskal-Wallis test was
used to assess ordinal scale parameters such as APACHE II score, SOFA score,
qCSI, and FIM. If significant difference was observed in the Kruskal-Wallis
test, a Mann-Whitney test was performed for the two identified parameters. For
FIM analysis, the Wilcoxon signed rank test was used for pre- and
post-rehabilitation comparisons. The gender and discharge outcomes were assessed
by the chi-square test. In considering discharge outcomes, because there were
three possible outcomes (home, transfer, or death), a chi-square test was
performed in a 3×3 contingency table. If a significant difference was
identified, a further chi-square test was performed in a 2×2 contingency table.
Statistical significance was set at P<0.05.
RESULTS
FRAM Model Construction
The hierarchical task analysis was modified seven times after its initial
creation. The list of set for the initial through to the seventh revision, a
total of eight patterns, is shown in Table
1 (the phases listed in Table
1 are explained below). Table
1 also shows a summary of what was considered in setting the
Functions. After the third development in Table 1, discussions were held to revise the system characteristics
that should be set as Function. As a result, Function were selected by focusing
on “actual patient treatment” and “actual rehabilitation medical systems” and
the fourth revision was proposed. Furthermore, changes in hospital beds caused
by the spread of infection and changes in the rehabilitation system because of
the increase in patients were incorporated as Functions, and final agreement on
the description of functions was reached in the eighth draft revision. In the
course of this discussion, the validity of the input, output, resource, time,
precondition, and control aspects of each function were also examined. In this
process, even if the same Function was used, if there was a change in the
description of the aspect, the Function was set as “modified.” In addition,
“viral characteristics,” which are not medical treatments, were considered the
important in establishing the COVID-19 system and were incorporated as a
function. In this pandemic, viral characteristics were agreed on as a Function
because “viral characteristics” are not “fixed and constant” but are diverse and
variable, and aspects such as susceptibility to infection and severity of
illness change irregularly, and these changes affect the entire system.
Table 1.
Transition of "Function" settings based on hierarchical
cross-checking
| Trial |
|
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
F9 |
F8m |
F10 |
F11 |
F12 |
F10m |
F12m |
| 1st |
Functions |
Acute treatment |
Rehabilitation treatment |
Physical therapist |
Potential infection risk |
ADL/QOL |
|
|
|
|
|
|
|
|
|
|
|
Configuration essentials |
The main functions of
“acute treatment” and “rehabilitation treatment” were
established as the usual treatment system in an acute care
hospital. The main functions are “acute treatment” and
“rehabilitation treatment” for medical rehabilitation. Outcomes
of rehabilitation care for patients infected with SARS-CoV-2
virus were defined as “Functions”. |
| 2nd |
Functions |
Acute treatment |
Rehabilitation treatment |
Physical therapist |
Potential infection risk |
ADL/QOL |
Establishment of a dedicated staffing
system |
|
|
|
|
|
|
|
|
|
|
Configuration essentials |
Following the 1st
functional model, the Function of “Establishment of a dedicated
staffing system” was added, which is the function of staff
exclusively engaged in care of COVID-19 patients. |
| 3rd |
Functions |
Acute treatment |
Rehabilitation treatment |
Physical therapist |
Potential infection risk |
Establishment of a dedicated staffing
system |
|
|
|
|
|
|
|
|
|
|
|
Configuration essentials |
“ADL/QOL” was positioned
not as a function but as a result of the performance of a
function and was excluded from the list of functions. |
| 4th |
Functions |
Newly admitted patients |
Treatment in the medical
department |
Nursing care in hospital wards |
Consultation by a rehabilitation
doctor |
Therapist involvement |
Improvement of disease and physical
motor function |
|
|
|
|
|
|
|
|
|
|
Configuration essentials |
A radical and universal
review was made in the setting of “Functions”. Author N.S. was
informed that “Function” should be positioned as an “activity”
or “set of activities” in which “Function is an actual action”.
Therefore, a “Function” is defined as “a set of actions actually
performed” in the usual clinical work. Based on this method, the
modeling of the usual clinical work was set in this 4th
step. |
| 5th |
Functions |
Newly admitted patients |
Treatment in the medical
department |
Nursing care in hospital wards |
Consultation by a rehabilitation
doctor |
Therapist involvement |
Improvement of disease and physical
motor function |
Dedicated hospital beds in
operation |
Dedicated rehabilitation physician and
therapist in charge |
|
|
|
|
|
|
|
|
Configuration essentials |
In addition to “the usual
clinical work” established in the 4th step, “Function” regarding
rehabilitation to COVID-19 was established in the 5th step.
Rehabilitation professionals were selected to work exclusively
with patients because they require long hours and close
proximity to patients. |
| 6th |
Functions |
Newly admitted patients |
Treatment in the medical
department |
Nursing care in hospital wards |
Consultation by a rehabilitation
doctor |
Therapist involvement |
Improvement of disease and physical
motor function |
SARS-CoV-2 characteristics |
Dedicated hospital beds in
operation |
Dedicated rehabilitation physician and
therapist in charge |
Dedicated hospital beds in
operation |
Remote consultation by rehabilitation
doctor |
Dedicated therapist |
|
|
|
|
Configuration essentials |
Because of the increased
number of infected patients in each administrative region, our
hospital facilities were expanded to include dedicated beds for
COVID-19 patients. Medical consultation of COVID-19 patients by
rehabilitation specialists with limited staffing was performed
remotely. These elements were added to the FRAM model. The
COVID-19 virus itself was found to have changed its infectivity
and mutated into characteristics that led to severe disease, and
“SARS-CoV-2 characteristics” were introduced as a
“Function”. |
| 7th |
Functions |
Newly admitted patients |
Treatment in the medical
department |
Nursing care in hospital wards |
Consultation by a rehabilitation
doctor |
Therapist involvement |
Improvement of disease and physical
motor function |
SARS-CoV-2 characteristics |
Dedicated hospital beds in
operation |
Dedicated rehabilitation physician and
therapist in charge |
Dedicated hospital beds in
operation |
Remote consultation by rehabilitation
doctor |
Dedicated therapist |
Rotational assignment of therapists in
charge |
|
|
|
Configuration essentials |
With the expansion of
COVID-19 beds and the increase in the number of patients on
ventilatory management and ECMO because of the increasing
severity of illness, the therapists dedicated to COVID-19 became
chronically fatigued. A permanent system was introduced in which
two of the five therapists rotated among the COVID-19 patients.
Therapists were required to stay at home for 5 days after 20
days of work to determine the risk of morbidity, and PCR testing
was conducted upon reentry to the workforce. |
| 8th |
Functions |
Newly admitted patients |
Treatment in the medical
department |
Nursing care in hospital wards |
Consultation by a rehabilitation
doctor |
Therapist involvement |
Improvement of disease and physical
motor function |
SARS-CoV-2 characteristics |
Dedicated beds in operation |
Dedicated rehabilitation physician and
therapist in charge |
Dedicated beds in operation |
Remote consultation by rehabilitation
doctor |
Dedicated therapist |
Rotational assignment of therapists in
charge |
Remote consultation by rehabilitation
doctor |
Rotational assignment of therapists in
charge |
| |
Configuration essentials |
In addition to medical
rehabilitation for patients infected outside the hospital, the
number of affected patients increased rapidly because of
cross-infection within the hospital. F10 m and F12 m were set as
“Functions” corresponding to these patients and having different
“inputs” from F10 and F12. The stay-at-home and PCR testing
measures for the therapist were withdrawn because their PPE was
found to be effective. F10 m and F12 m also reflected these
changes. |
F, Function(s); m, modified; QOL, quality of life; ECMO, extracorporeal
membrane oxygenation
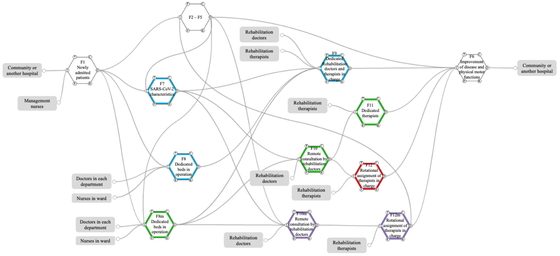
The eighth and final Functions and aspects are described in Table 2. The connections between the functions
listed in Table 2 are shown in Figs. 1 and 2. F1 to F6 show the usual medical rehabilitation
system. The acceptance of COVID-19 cases in parallel with this regular system
was set as F7, F8, and F9. This setup was established to accept a maximum of
four patients from the start of rehabilitation for the first COVID-19 case. One
rehabilitation therapist was selected to provide rehabilitation to the patients.
Next, the number of beds for COVID-19 patients was increased to six, with two
therapists in charge, because all four beds were continuously occupied, and the
conditions of patients remained severe. In Table 2 and Fig. 2, these
elements are presented as F8m, F10, and F11. Furthermore, the emergence of
mutant strains of the virus was confirmed, and the number of cases in the
medical area increased. In light of this situation, the number of beds dedicated
to COVID-19 was increased to 18. The number of rehabilitation patients also
increased, necessitating the establishment of a sustainable system. Because the
number of rehabilitation doctors on staff was limited, remote consultation was
introduced to avoid the risk of cross-infection. The risk of cross-infection was
a concern because rehabilitation therapists must spend a lot of time with
patients. Therefore, after approximately 3 weeks of responsibility for COVID-19
cases, the staff were placed on home leave for 5 days, and a system was set up
to perform polymerase chain reaction (PCR) testing. After a negative test was
confirmed, the staff member was returned to work in a general hospital ward.
Table 2 shows these system
modifications as F10m and F12.
Table 2.
Description of Functions and Components for FRAM
| Usual |
F1 |
Newly admitted patients |
|
F2 |
Treatment in the medical
department |
|
F3 |
Nursing care in hospital
wards |
|
I |
Hospitalization, Permission for
hospitalization |
|
I |
Assignment of departments,
Intention to treat |
|
I |
Assignment of ward,
Nursing care |
|
O |
Assignment of departments, Assignment
of ward |
|
O |
Treatment, Request for
rehabilitation |
|
O |
Needs for
rehabilitation |
|
P |
|
|
P |
Information from
rehabilitation doctors and therapists |
|
P |
Information from
rehabilitation physicians and therapists |
|
R |
|
|
R |
Needs for
rehabilitation |
|
R |
|
|
C |
|
|
C |
Judgement on
rehabilitation indication |
|
C |
|
|
T |
|
|
T |
Daily, Continuous |
|
T |
Daily, Continuous |
|
|
|
|
|
|
|
|
|
|
F4 |
Consultation by a rehabilitation
doctor |
|
F5 |
Therapist involvement |
|
F6 |
Improvement of disease and
physical motor function |
|
I |
Request for rehabilitation, Medical
examination |
|
I |
Rehabilitation
prescription, Readiness to respond |
|
I |
Treatment, Progress in
hospitalization, Medical rehabilitation treatment |
|
O |
Rehabilitation prescription |
|
O |
Medical rehabilitation
treatment |
|
O |
Discharge |
|
P |
|
|
P |
Information from attending
physician, nurse, and rehab physician |
|
P |
|
|
R |
Medical record entry |
|
R |
Medical record
information |
|
R |
|
|
C |
|
|
C |
|
|
C |
|
|
T |
|
|
T |
Daily, Continuous |
|
T |
|
|
|
|
|
|
|
|
|
|
| Phase I |
F7 |
SARS-CoV-2 characteristics |
|
F8 |
Dedicated beds in
operation |
|
F9 |
Dedicated rehabilitation
doctors and therapists in charge |
|
I |
Contracting the virus, COVID-19
infection during hospitalization |
|
I |
Inpatients, Risk of
spreading infection, Nursing care, Intention to treat |
|
I |
Risk of spreading
infection, Need for rehabilitation, Rehabilitation examination,
Readiness to respond |
|
O |
Risk of spreading infection |
|
O |
Need for
rehabilitation |
|
O |
Conduct of therapy |
|
P |
|
|
P |
|
|
P |
Avoidance of close
contact |
|
R |
|
|
R |
|
|
R |
Human restriction |
|
C |
Infection transmission capability,
Organ damage capability, Unknown characteristics |
|
C |
Small number of
patients |
|
C |
Separation of lines of
flow |
|
T |
|
|
T |
Daily, Continuous |
|
T |
Daily, Continuous |
|
|
|
|
|
|
|
|
|
| Phase II |
F8m |
Dedicated beds in operation |
|
F10 |
Remote consultation by
rehabilitation doctor |
|
F11 |
Dedicated therapist |
|
I |
Inpatients, Intention to treat |
|
I |
Request for
rehabilitation, Medical examination |
|
I |
Risk of spreading
infection, Need for rehabilitation, Readiness to respond |
|
O |
Request for rehabilitation,
Nursing |
|
O |
Rehabilitation
prescription |
|
O |
Conduct of therapy |
|
P |
Information from rehabilitation
doctors and therapists |
|
P |
No infection risk |
|
P |
Inevitability of close
contact |
|
R |
|
|
R |
Deployment of remote
terminals |
|
R |
Two-person system |
|
C |
Getting larger number of patients |
|
C |
Continuous operation |
|
C |
Separation of flow lines,
Continuous operation |
|
T |
Daily, Continuous |
|
T |
Daily, Continuous |
|
T |
Daily, Continuous |
|
|
|
|
|
|
|
|
|
| Phase III |
F12 |
Rotational assignment of
therapists in charge |
|
|
|
|
I |
Rehabilitation
prescription, Readiness to respond |
|
|
|
|
O |
Implementation of therapy,
Participation in regular clinical practice, Continuous
operation |
|
|
|
|
P |
Periodic rotation, Two of
the five staff members work full-time in shifts |
|
|
|
|
R |
Availability of personnel,
Five self-directed therapists |
|
|
|
|
C |
Separation of flow lines,
Routine PCR testing, Five days home stay to avoid false negative
before PCR test |
|
|
|
|
T |
Daily, Continuous |
|
|
|
|
|
|
|
|
|
|
| Phase IV |
F10m |
Remote consultation with a
rehab doctor |
|
F12m |
Rotational assignment of
therapists in charge |
|
I |
Request for rehabilitation
medical treatment, Request for medical examination for cases
occurring in the hospital, Medical examination |
|
I |
Rehabilitation
prescription, Response to hospital outbreaks, Readiness to
respond |
|
O |
Rehabilitation
prescription, Continued operation |
|
O |
Implementation of therapy,
Participation in regular clinical activities, Ongoing
operations |
|
P |
No infection risk |
|
P |
Negative PCR test results
for 500 consecutive persons/day, Clarification that PPE is
sufficiently effective |
|
R |
Deployment of remote
terminals |
|
R |
Staffing |
|
C |
|
|
C |
Continuation of periodic
rotation, Removal of line of flow separation, Release PCR test,
Removal of home confinement |
|
T |
Daily, Continuous |
|
T |
Daily, Continuous |
|
|
|
|
|
|
|
| Each profession |
F |
Doctors in each
department |
Rehabilitation
doctors |
Management nurses |
Nurses in ward |
Rehabilitation therapists |
|
I |
|
|
|
|
|
|
O |
Intention to
treatment |
Medical examination |
Permission to
hospitalization |
Nursing care |
Readiness to respond |
|
P |
|
|
|
|
|
|
R |
|
|
|
|
|
|
C |
|
|
|
|
|
|
T |
|
|
|
|
|
F, function; I, input; O, output; P, preconditions; R, resources; C,
control; T, time; m, modified; Modifiers are indicated by
underlines.

The COVID-19 clinic system has become permanent. The use of periodic home stays
and PCR testing were terminated after repeated negative PCR tests continued to
show negative results and the routine use of PPE by rehabilitation professionals
was found to be effective. As the number of infected patients increased, the
rate of cross-infection of patients in the hospital increased rapidly, leading
to the establishment of a new ward as a COVID-19 receiving ward to accommodate
the patients. Examination by rehabilitation doctors and rehabilitation by a
specialist were also modified and set as F10m and F12m. As described above, the
functional settings were modified in accordance with the viral characteristics
of COVID-19, the increase in the number of patients in the region, and hospital
readiness. These changes were linked to the number of infected patients in Japan
and were made in accordance with the time of year.
The period when each function was established was divided into phases (Table 1): Phase I: F7, F8, F9 setup
period (May 6–July 31, 2020); Phase II: F8m, F10, F11 setup period (August
1–December 10, 2020); Phase III: F12 setup period (December 11, 2020–September
30, 2021); Phase IV: F10m, F12m setup period (October 1, 2021–June 30, 2022).
Figure 3 shows the number of
patients infected during each period, the number of infected patients in Japan,
and the cumulative number of COVID-19 rehabilitated patients at our
institution.
Patient Characteristics, Rehabilitation-related Healthcare Costs, and
Functional Independence in Each Phase
Between May 2020 and June 2022, 140 patients prescribed with COVID-19 medical
rehabilitation were admitted, and 139 patients underwent medical rehabilitation
at the Rehabilitation Center of Hyogo Medical University Hospital. One patient
was transferred to another hospital before our intervention. Of these 139 cases,
the cases of 2 patients aged under 18 years and that of a continuously
hospitalized patient were excluded. Of the remaining 136 patients to be
analyzed, the number of patients in each of Phases I to IV was 1, 16, 97, and
22, respectively. Outcomes in Tables
3 and 4 show comparisons
between the three groups: Phase I and II patients (n=17) combined, Phase III
patients (n=97), and Phase IV patients (n=22).
Table 3.
Patient characteristics and socio-economic outcome
| Characteristic |
Phase I, II |
Phase III |
Phase IV |
| Age (years) |
69.9 ± 11.9 |
|
62.1 ± 12.4 |
|
68.5 ± 18.7 |
|
| Male/female (n) |
14 /3 |
|
67 /30 |
|
17 /5 |
|
| BMI (kg/m2) |
23.3 ± 4.1 |
|
25.6 ± 5.3 |
|
21.9 ± 5.9 |
†† |
| APACHE II score |
16 (13–20) |
|
13 (10–17) |
** |
16.5 (14–25.5) |
† |
| SOFA score |
3 (2–5) |
|
3 (2–5) |
|
3 (2–7.5) |
|
| qCSI |
6 (5–8) |
|
6 (5–7) |
|
7 (5–7) |
|
| Hospitalization period (days) |
59.5 ± 67.7 |
|
19.8 ± 24.6 |
** |
25.6 ± 13.5 |
** |
| Unprescribed periods (days) |
13.1 ± 9.0 |
|
1.3 ± 1.3 |
** |
3.2 ± 3.2 |
** |
| RME (JPY) |
236,235.3 ± 311,826.5 |
|
61,773.2 ± 56,406.0 |
** |
55,693.2 ± 42,774.9 |
** |
| RME/rehabilitation periods
(JPY/day) |
4594.2 ± 2107.0 |
|
4151.4 ± 1723.1 |
|
2821.3 ± 1187.8 |
**, †† |
| Home/transfer/death (n) |
7/7/3 |
|
12/67/18 |
** |
8/9/5 |
†† |
| Home/transfer/death (%) |
(41.2/41.2/17.6) |
|
(12.4/69.1/18.6) |
** |
(34.8/39.1/21.7) |
†† |
Data given as mean ± standard deviation, number, or median score
(interquartile range).
* P<0.05 vs. Phase I, II; ** P<0.01 vs. Phase I, II; † P<0.05
vs. Phase III; †† P<0.01 vs. Phase IV
Table 4.
Rehabilitation outcomes represented by FIM
|
Number of patients |
Motor FIM |
Cognitive FIM |
FIM (total score) |
| Pre / post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
| Phase I, II |
17 / 14 |
13.0 |
(13.0–48.0) |
79.0 |
(51.0–89.0) |
b |
13.0 |
(5.0–35.0) |
35.0 |
(34.0–35.0) |
a |
26.0 |
(18.0–83.0) |
114.0 |
(86.0–124.0) |
b |
| Phase III |
97 / 79 |
13.0 |
(13.0–15.0) |
42.5 |
(13.0–57.0) |
b |
35.0 |
(5.0–35.0) |
35.0 |
(12.0–35.0) |
* |
48.0 |
(18.0–48.0) |
77.5 |
(32.8–92.0) |
b |
| Phase IV |
22 / 17 |
13.5 |
(13.0–35.5) |
42.5 |
(13.0–64.0) |
b |
32.0 |
(19.3–35.0) |
33.0 |
(6.5–35.0) |
* |
48.0 |
(32.5–70.5) |
75.5 |
(19.5–99.0) |
a |
Data given as median (interquartile range). Differences in patient number
between pre and post were caused by patient deaths.
a, P<0.05 vs. Pre; b, P<0.01 vs. Pre; * P<0.05 vs. Phase I,
II.
The duration of hospitalization and the periods of unprescribed rehabilitation
were significantly shorter in Phases III and IV than in Phases I and II. Patient
severity was similar or slightly worse in each period. The transfer discharge
outcome was significantly higher in Phase III than in Phases I, II, and IV.
Mortality showed no difference between phases (Table 3).
The FIM score was used to represent the rehabilitation outcome (Table 4). Because the FIM score data
for 13 patients were missing, 126 patients were analyzed after exclusion of
these patients. Higher scores were observed in the post-rehabilitation motor FIM
and total FIM in each phase compared with pre-rehabilitation scores. The
cognitive FIM scores in Phases III and IV were significantly higher than those
in Phases I and II. The accumulation of these factors resulted in a decrease in
rehabilitation-related medical expenses (Table 3).
DISCUSSION
This study analyzed the use of FRAM to optimize medical rehabilitation in an
environment of increased numbers of COVID-19 patients and examined the effectiveness
of rehabilitation optimization for severe COVID-19. The results confirmed that the
optimization of the system in response to the spread of infection resulted in
shorter hospital stays, earlier initiation of rehabilitation, maintenance of ADLs,
and reduction of rehabilitation-related medical costs. In relation to rehabilitation
treatment in medical settings under the circumstances of the COVID-19 pandemic, to
our knowledge, this is the first report of a FRAM analysis of a treatment
system.
Medical systems are complex, diverse, multi-scale systems that encompass hierarchical
and non-hierarchical structures.12) In such healthcare systems, rehabilitation medicine
encompasses multiple diseases and disabilities, involves multiple departments and
professions, and is established by the assembly of individuals, professional fields,
medical teams, and related departments in a hierarchical or parallel
manner.12)
Furthermore, the system of rehabilitation medicine is also a component of a larger
organization or structure.12) The COVID-19 pandemic required adaptation in these
nested, distributed, parallel, and hierarchical structures, whether large or small.
FRAM13) was
developed to analyze systems that exhibit complex structure and behavior, and its
principles include the equivalence of failures and successes, the approximate
adjustments, emergence, and resonance.12) The various measures we have implemented in
expansion of the COVID-19 rehabilitation system have had uncertain success or
failure from time to time. Outcomes obtained in this way are considered emergent
outcomes rather than planned events. For these reasons, we considered FRAM
appropriate for analyzing the system optimization of rehabilitation medicine
implemented under the COVID-19 expansion.
The practice of FRAM revealed several characteristics in the optimization of the
COVID-19 rehabilitation system. The first measure was the respective separation of
general care, treatment of infected patients, and staff. The main task required to
avoid droplet infection is to minimize exposure,23) and it can be inferred that the basic policy of
this countermeasure was appropriate. The second identified measure was staff
rotation and remote consultation of rehabilitation physicians. A previous
study24)
reported that clear strategies for appropriately managing healthcare workers include
risk stratification, appropriate clinical monitoring, access to low-threshold
diagnostic procedures, and decision making about removal from and return to work.
Another report25) has
described the effectiveness of organizational coordination, staff classification,
and personalized services for rehabilitation services in COVID-19. The Functions
such as staff rotation and remote consultation that were presented in this study as
a result of FRAM correspond to these elements. Therefore, the measures we have taken
from time to time can be considered to have been appropriate.
The analysis clearly indicated that rehabilitation therapists need a high level of
infection protection because of the inevitability of direct and prolonged contact
with patients. In addition, they also need training in how to deal with
aerosol-generating situations such as coughing and huffing.
Within FRAM, a Function is defined “the means necessary to achieve a goal.”26) According to this
definition, the viral characteristics of SARS-CoV-2 (F7) are ineligible and may have
to be indicated as preconditions for F1. However, at any time, the characteristics
of the SARS-CoV-2 virus itself are changing, and the susceptibility to infection and
the organ damage associated with infection are mixed. Therefore, in this report,
viral characteristics were defined as a Function to indicate two variables
(infectivity and organ damage) as a control. However, there are cases where these
characteristics themselves, such as infectivity, organ damage potential, and other
unknown characteristics, are variable and may need to be shown as individual
Functions.
The system incorporates medical doctors, nurses, and therapists as Functions.
However, it may be more appropriate to treat these human factors as Resources in the
system, because many professions are involved in healthcare.27) The duties of each
profession are strictly defined according to the respective laws and regulations.
This definition is the expertise allowed to each profession, and the preceding
placement of the profession is essential in the medical treatment performed.
Therefore, each profession is positioned as a Function that generates output for
subsequent medical treatment. Therefore, in this study, each profession was analyzed
as a Function.
The F12m system was established as a more permanent system, and periodic PCR testing
of full-time therapists was suspended because no full-time therapists were infected
with SARS-CoV-2 during the 540 person-days of intervention in the COVID-19 beds.
Therefore, the PCR-negative results of 540 person-days and the test results of 27
full-time therapists were used as the basis for the suspension of routine PCR
testing. However, it is difficult to interpret whether the suspension of routine
testing was justified. Prior studies have reported a risk aversion rate of over 95%
(26 negative results out of 27 PCR tests) for COVID-19 infection by PPE,28) whereas the test
results in this study were negative (100%) on 27 occasions. These results suggest
that the routine wearing of PPE by each therapist was adequate and our response was
appropriate.
No difference was observed between phases for the comorbidity score or COVID-19
severity scores, but the APACHE-II score was significantly lower in Phase III. This
period was the longest of all periods, and the large number of patients included in
the study suggests that many of the patients may have had mild symptoms. It is
possible that the hospitalization period was associated with mild symptoms. In
particular, there was a significant reduction in the length of hospitalization and
the time to start rehabilitation. The rotation of rehabilitation professions
indicated in F12 has enabled a sustainable rehabilitation system to be established,
and rehabilitation treatment can be started promptly after admission.
In Phases I and II, the facility could not cope with the increase in the number of
patients, and interventions were made only after progression in the decline of
physical motor function. However, from Phase III onward, rapid interventions were
possible. This may have led to better outcomes in a shorter period by reducing the
decline in ADL, especially in cognitive function, at the time of intervention, while
patient severity remained unchanged. The reduction in length of hospital stay and
the suppression and improvement of ADL decline in the hospital may have resulted in
a decrease in rehabilitation-related medical costs.
This study has several limitations. In this study, we set each Function of FRAM based
on actual actions by hierarchical cross-checking. However, the model may lack
reproducibility and universality because of the high degree of freedom in setting
and describing each Function. In addition, the range of each Function acting on the
entire system is infinitely wide and can be infinitely subdivided, making it
essential to verify the validity of the breadth and narrowness of the descriptions
in this report.
In creating the FRAM model, Functions were set based on actual procedures. However,
there are “imagined actions” and “assumed troubles” behind some actions and
countermeasure practices. Although these actions are not actually performed, they
are one of the elements of system variation and are described as “work-as-imagined”
(WAI).29) The
analysis of this WAI is an issue for future studies.
Although we have attempted to formulate the Functions in a prospective manner, the
analysis of disturbances that occur suddenly and without warning must be performed
retrospectively. In the present study, we performed a retrospective analysis,
whereas a previous study30) with FRAM was conducted as a prospective study. In
the future, it will be important to verify the usefulness of FRAM from a predictive
perspective in our study.
CONCLUSION
A retrospective analysis with FRAM confirmed that optimization of the system in
response to the spread of infection, as implemented from time to time, resulted in
shorter hospital stays, earlier initiation of rehabilitation, maintenance of ADLs,
and reduction of medical costs. The results suggest that FRAM is useful for
retrospective analysis of changes in the rehabilitation healthcare system, which may
change over time.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Johns Hopkins University of Medicine.
Coronavirus Resource Center. 2023. https://coronavirus.jhu.edu/map.html.
Accessed 24 January 2023.
- 2. Khan M, Adil SF, Alkhathlan HZ, Tahir MN,
Saif S, Khan M, Khan ST: COVID-19: a global challenge with old history,
epidemiology and progress so far. Molecules 2020;26:39–63. PMID:33374759,
DOI:10.3390/molecules26010039
- 3. Gattinoni L, Chiumello D, Caironi P,
Busana M, Romitti F, Brazzi L, Camporota L: COVID-19 pneumonia: different
respiratory treatments for different phenotypes? Intensive Care Med
2020;46:1099–1102. PMID:32291463,
DOI:10.1007/s00134-020-06033-2
- 4. Paneroni M, Simonelli C, Saleri M,
Bertacchini L, Venturelli M, Troosters T, Ambrosino N, Vitacca M: Muscle
strength and physical performance in patients without previous disabilities
recovering from COVID-19 pneumonia. Am J Phys Med Rehabil 2021;100:105–109.
PMID:33181531, DOI:10.1097/PHM.0000000000001641
- 5. Ceban F, Ling S, Lui LM, Lee Y, Gill H,
Teopiz KM, Rodrigues NB, Subramaniapillai M, Di Vincenzo JD, Cao B, Lin K,
Mansur RB, Ho RC, Rosenblat JD, Miskowiak KW, Vinberg M, Maletic V, McIntyre RS:
Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review
and meta-analysis. Brain Behav Immun 2022;101:93–135. PMID:34973396,
DOI:10.1016/j.bbi.2021.12.020
- 6. van Wagenberg L, Witteveen E, Wieske L,
Horn J: Causes of mortality in ICU-acquired weakness. J Intensive Care Med
2020;35:293–296. PMID:29241382, DOI:10.1177/0885066617745818
- 7. Schweickert WD, Pohlman MC, Pohlman AS,
Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D,
Schmidt GA, Bowman A, Barr R, McCallister KE, Hall JB, Kress JP: Early physical
and occupational therapy in mechanically ventilated, critically ill patients: a
randomised controlled trial. Lancet 2009;373:1874–1882. PMID:19446324,
DOI:10.1016/S0140-6736(09)60658-9
- 8. Uchiyama Y, Sasanuma N, Nanto T, Fujita
K, Takahashi M, Iwasa S, Koyama T, Kodama N, Domen K: COVID-19 patient returned
to work after long hospitalization and follow-up: a case report. Prog Rehabil
Med 2021;6:20210025. PMID:34164586, DOI:10.2490/prm.20210025
- 9. Harrod M, Petersen L, Weston LE, Gregory
L, Mayer J, Samore MH, Drews FA, Krein SL: Understanding workflow and personal
protective equipment challenges across different healthcare personnel roles.
Clin Infect Dis 2019;69:S185–S191. PMID:31517971,
DOI:10.1093/cid/ciz527
- 10. Thomas P, Baldwin C, Bissett B, Boden I,
Gosselink R, Granger CL, Hodgson C, Jones AY, Kho ME, Moses R, Ntoumenopoulos G,
Parry SM, Patman S, van der Lee L: Physiotherapy management for COVID-19 in the
acute hospital setting: clinical practice recommendations. J Physiother
2020;66:73–82. PMID:32312646, DOI:10.1016/j.jphys.2020.03.011
- 11. Kamalakannan S, Chakraborty S:
Occupational therapy: the key to unlocking locked-up occupations during the
COVID-19 pandemic. Wellcome Open Res 2020;5:153–163. PMID:32766458,
DOI:10.12688/wellcomeopenres.16089.1
- 12. Hollnagel E. The Principles. In: FRAM: the
Functional Resonance Analysis Method modelling complex socio-technical systems.
Boca Raton: CRC Press; 2012.pp. 21–32.
- 13. Damen NL, de Vos MS, Moesker MJ,
Braithwaite J, de Lind van Wijngaarden RA, Kaplan J, Hamming JF, Clay-Williams
R: Preoperative anticoagulation management in everyday clinical practice: an
international comparative analysis of work-as-done using the functional
resonance analysis method. J Patient Saf 2021;17:157–165. PMID:29994818,
DOI:10.1097/PTS.0000000000000515
- 14. Clay-Williams R, Hounsgaard J, Hollnagel
E: Where the rubber meets the road: using FRAM to align work-as-imagined with
work-as-done when implementing clinical guidelines. Implement Sci
2015;10:125–132. PMID:26319404, DOI:10.1186/s13012-015-0317-y
- 15. Ogrinc G, Davies L, Goodman D, Batalden
P, Davidoff F, Stevens D: SQUIRE 2.0 (Standards for QUality Improvement
Reporting Excellence): revised publication guidelines from a detailed consensus
process: Table 1. BMJ Qual Saf 2016;25:986–992. PMID:26369893,
DOI:10.1136/bmjqs-2015-004411
- 16. Hollnagel E: The Method: The Identification
of Variability (Step 2). In: FRAM: the Functional Resonance Analysis Method
modelling complex socio-technical systems. Boca Raton: CRC Press; 2012. pp.
63–75.
- 17. Granger CV, Hamilton BB, Linacre JM,
Heinemann AW, Wright BD: Performance profiles of the functional independence
measure. Am J Phys Med Rehabil 1993;72:84–89. PMID:8476548,
DOI:10.1097/00002060-199304000-00005
- 18. Knaus WA, Draper EA, Wagner DP, Zimmerman
JE: APACHE II: a severity of disease classification system. Crit Care Med
1985;13:818–829. PMID:3928249,
DOI:10.1097/00003246-198510000-00009
- 19. Lambden S, Laterre PF, Levy MM, Francois
B: The SOFA score—development, utility and challenges of accurate assessment in
clinical trials. Crit Care 2019;23:374–382. PMID:31775846,
DOI:10.1186/s13054-019-2663-7
- 20. Haimovich AD, Ravindra NG, Stoytchev S,
Young HP, Wilson FP, van Dijk D, Schulz WL, Taylor RA: Development and
validation of the quick COVID-19 severity index: a prognostic tool for early
clinical decompensation. Ann Emerg Med 2020;76:442–453. PMID:33012378,
DOI:10.1016/j.annemergmed.2020.07.022
- 21.Yanagida Y, Sasanuma N, Miyagi Y,
Yamakawa S, Seo T, Shirai K, Kodama N, Uchiyama Y, Domen K: Pulmonary
oxygenation capacity during repositioning and survival outcome in patients with
coronavirus disease 2019 (COVID-19): an analysis of the relationship [in
Japanese]. Phys Ther Jpn 2023;50:1–7. DOI:10.15063/rigaku.12287
- 22.Seo T, Sota K, Miyagi Y, Tsuda K,
Yanagida A, Sasanuma N, Uchiyama Y, Domen K: The effect of pulmonary physical
therapy and exercise therapy for a severe COVID-19 patient: focused on intensive
care unit-acquired weakness and exercise induced hypoxemia [in Japanese]. Phys
Ther Jpn 2022;49:415–420. DOI:10.15063/rigaku.12291
- 23. Harte J, Hamzah L: COVID-19: management
and infection control. Medicine (Abingdon) 2021;49:794–796. PMID:34584489,
DOI:10.1016/j.mpmed.2021.09.014
- 24. Bielicki JA, Duval X, Gobat N, Goossens
H, Koopmans M, Tacconelli E, van der Werf S: Monitoring approaches for
health-care workers during the COVID-19 pandemic. Lancet Infect Dis
2020;20:e261–e267. PMID:32711692,
DOI:10.1016/S1473-3099(20)30458-8
- 25. Hu S, Chen C, Yang B, Liu Q, Hu H:
Experience of rehabilitation management in public hospital after it was
identified as designated rehabilitation hospital for COVID-19 patients: a
qualitative study. Front Public Health 2022;10:919730. PMID:35958844,
DOI:10.3389/fpubh.2022.919730
- 26. Hollnagel E: The Method: Identify and
Describe the Functions (Step 1). In: FRAM: the Functional Resonance Analysis
Method modelling complex socio-technical systems. Boca Raton: CRC Press; 2012.
pp. 39–61.
- 27. Sinclair LB, Lingard LA, Mohabeer RN:
What’s so great about rehabilitation teams? An ethnographic study of
interprofessional collaboration in a rehabilitation unit. Arch Phys Med Rehabil
2009;90:1196–1201. PMID:19577033,
DOI:10.1016/j.apmr.2009.01.021
- 28. Ha JF: The COVID‐19 pandemic, personal
protective equipment and respirator: a narrative review. Int J Clin Pract
2020;74:e13578. PMID:32511834, DOI:10.1111/ijcp.13578
- 29. Hollnagel E: The Principles. In: FRAM: the
Functional Resonance Analysis Method modelling complex socio-technical systems.
Boca Raton: CRC Press; 2012. pp. 33–38.
- 30. Arcuri R, Bellas HC, Ferreira DS, Bulhões
B, Vidal MC, Carvalho PV, Jatobá A, Hollnagel E: On the brink of disruption:
applying resilience engineering to anticipate system performance under crisis.
Appl Ergon 2022;99:103632. PMID:34740073,
DOI:10.1016/j.apergo.2021.103632
