ABSTRACT
Objectives: This study investigated the transition patterns of
activities of daily living (ADL) status based on the Functional Independence
Measure (FIM) motor and cognitive items in patients who experienced subacute
stroke.
Methods: In this single-site, retrospective investigation, 1592 FIM
samples were collected during the hospitalization of 373 stroke patients who
were admitted between April 2018 and March 2020. FIM item levels were
transformed from seven to three (FIM1–2, Complete Dependence; FIM3–5, Modified
Dependence; FIM6-7, Independence). FIM samples were classified by latent class
modeling into six latent ADL states based on the independence levels of FIM
motor and cognitive items. We created an ADL status transition diagram based on
the FIM sample’s probability of belonging to each status at different
hospitalization timepoints.
Results: Transition diagrams for each ADL status at admission
revealed distinct patterns. In two ADL statuses for which patients required full
assistance in FIM motor items, the patients remained motor-dependent without
achieving independence on discharge. In contrast, patients in transition from
the other four ADL statuses largely achieved independence in motor items by the
time of discharge. The time required to reach higher ADL status varied according
to the initial ADL status at admission; the slowest improvement was observed in
statuses initially classified as needing the most assistance, whereas many
patients achieved transition within 3 months from admission.
Conclusions: Based on the characteristics of patient ADL status and
timing of its changes, the classification of ADL status and visualization of ADL
transition can contribute to improved treatment.
INTRODUCTION
Stroke patients often experience long-term hospitalization for rehabilitation because
of functional impairment and reduced independence in activities of daily living
(ADL). Several studies of ADL have used multiple regression to predict the ADL
status at single timepoints, including on admission or discharge.1,2,3,4) However, to improve
clinical applications and treatment during long hospital stays, it is useful to
investigate changes in ADL status at multiple timepoints during hospitalization.
The Functional Independence Measure (FIM) has been used to measure ADL in several
stroke studies. FIM is a seven-step ordinal scale that comprises 18 items divided
into motor and cognitive categories. The total scores (FIM-total, FIM-motor, and
FIM-cognition) are often included in the analysis as a one-dimensional continuous
variable. The multidimensional ordinal categorical scale is treated as a
quantitative scale; however, the inability to observe qualitative differences
because of the combination of responses is a disadvantage. Regarding the
relationships between FIM items, a survey was conducted on the relative difficulty
of each FIM motor item using a Rasch analysis5,6) and a probability distribution of the independence
level of FIM motor items was established using ordinal logistic
regression.7)
However, to the best of our knowledge, no study has investigated the combination of
multidimensional FIM motor items and cognitive items. In stroke patients, where both
higher brain and motor dysfunction inhibit ADL,8) it is important to interpret the ADL structure
by considering the combination of motor and cognitive items.
Regarding changes in ADL over time, Koyama et al.9) and Kimura et al.10) used logarithmic modeling to predict
the recovery process of the total FIM motor scores, and Soh et al.11) reported the
trajectory of functional performance in older adults. However, to the best of our
knowledge, no study has investigated the changes in ADL status over time regarding
the combination of motor and cognitive items of the FIM in hospitalized stroke
patients undergoing rehabilitation.
In this study, we used a latent class analysis (LCA),12,13,14) which has recently attracted attention as a mixture
model for qualitative data, to characterize ADL status by considering the
combination of responses to FIM motor and cognitive items. LCA is a form of
unsupervised learning that does not require pre-specified criteria or class
characteristics for classification and classifies samples in a population into
unknown subpopulations (i.e., latent class) that are homogenous in their response
patterns to observed qualitative variables.12,13,14) Recently, LCA has been applied in several medical
studies.15,16,17) For example, Thomas et al.18) demonstrated a
subtyping pattern for juvenile patients with idiopathic arthritis via a combination
of arthritic symptoms. By classifying FIM samples based on the combination of
responses to FIM items, it is possible to identify latent ADL status by considering
both motor and cognitive items. Using LCA among stroke inpatients, we previously
demonstrated the effectiveness of extracting ADL segments based on a combination of
FIM items.19)
Latent class models have been used to analyze the transition of multidimensional
health status based on several health conditions.20,21) Lafortune et al.21) reported the transition of health
status at three timepoints based on a combination of cognitive function,
comorbidities, and disabilities. These analytical methods utilize samples surveyed
for multiple health conditions at different timepoints to reveal the temporal
transitions from health status profiles at one timepoint to those at different
timepoints.22)
The aim of this study was to clarify the transition patterns of various ADL statuses
by simultaneously considering the FIM motor and cognitive items among inpatients
with subacute stroke. We previously used LCA to classify FIM samples into six latent
ADL states (latent class).19) This classification was based on the combination of
responses to FIM motor and cognitive items (ordinal category scale). Herein, we
utilized the classified data from the previous study,19) and expanded the analysis of the
transition over time to create a transition diagram depicting the patterns of
transition among the ADL states. Furthermore, we present several suggestions to
improve interventions based on the characteristics of the ADL status and transition
patterns.
MATERIALS AND METHODS
This single-center, retrospective observational investigation was part of a previous
study conducted at the Saiseikai Higashikanagawa Rehabilitation Hospital in
Japan.19)
Patients with infarction or hemorrhage were selected from a total of 613 patients
with cerebrovascular disorders who were hospitalized between April 2018 and March
2020. Patients were excluded according to the following criteria10): subarachnoid
hemorrhage, subdural hemorrhage, conditions affecting the cerebellum and brainstem,
or co-occurrence of acute locomotion-related disorders (see previous study for
patient selection details).19)
Measures
Among the various tools commonly utilized to assess ADL, FIM,23) which has a
verified reliability and validity,5,6,24,25,26) was adopted and measured by nurses once a month
from admission to discharge. To ensure the reliability of FIM, the FIM scores
were checked at monthly interprofessional conferences. FIM comprises 13 motor
and 5 cognitive items. Each item was measured on a seven-level
ordinal-categorical scale (1=total assistance; 2=maximal assistance; 3=moderate
assistance; 4=minimal assistance; 5=supervision; 6=modified independence, and
7=complete independence). These seven levels were integrated into three levels
(1–2=Complete Dependence; 3–5=Modified Dependence; and 6–7=Independence) to
adapt to the latent class model.27,28)
Statistical Analysis
The number of FIM samples per patient differed according to the length of
hospitalization required for stroke rehabilitation. Therefore, we chose a method
of capturing an individual patient’s ADL representation at each timepoint
by first classifying all FIM samples into latent ADL statuses using LCA and then
reaggregating them according to timepoints. We assumed that FIM samples were
independent and assessed under identical circumstances despite the likelihood of
some differences in clinical circumstances at different timepoints. In contrast
to cluster analysis, which categorizes the entire sample into a single class,
LCA was used to calculate the probability of membership in each specific latent
class for all samples. Upon leveraging the probabilities of belonging to each
specific latent class for FIM samples at each timepoint, temporal transitions of
latent ADL statuses were elucidated. This approach allowed detailed
understanding of changes in an individual patient's status using condition
samples at multiple timepoints.
In our previous study,19) LCA was applied to the dataset of all FIM
samples. The samples were classified into six latent classes based on the
combination of responses to the 18 FIM items that incorporated three-level
ordinal categorical variables. The classified latent classes were interpreted
and named as latent ADL statuses based on the response probabilities calculated
for each class. Details of the classification of FIM samples are provided in our
previous report.19)
In the present study, we utilized data obtained following the classification
into six latent classes19) to clarify and visualize the transitions
among the classes. By utilizing the probability of each FIM sample belonging to
each class at different evaluation timepoints (calculated using LCA and included
in the previous data),19) we probabilistically determined the
classes to which each patient's FIM samples transitioned during the
interval between timepoints. This process allowed the generation of transition
diagrams for ADL status.
The probability π^gntG|NT
that the FIM sample of patient n at time t belongs to the latent class g can be
expressed using Eq. 1 as follows:
|
π
^
g
n
t
G
|
N
T
=
P
G
n
t
=
g
X
1
n
t
,
X
2
n
t
,
…
,
X
18
n
t
)
| (1) |
based on the following notation: latent class G (g; 1 to G); patient N (n; 1 to
N); timepoint T (t; 0 to T); response to 18 items of the FIM X1–X18 (x1
to x18; Complete Dependence, Modified Dependence, and Independence). The
evaluation timepoints were as follows: t=0 (admission), t=1 (1 month after
admission), up to t=6 representing 6 months.
Using Eq. 1 for weighting, we calculated the number of each patient's FIM
samples transitioning between ADL statuses at each timepoint and constructed
transition diagrams of ADL status. Moreover, transition diagrams of ADL status
were stratified according to ADL status at admission. For example, the weighted
number of samples transitioning between latent classes (g=1 to G) at timepoints
(t=0 to T) can be expressed as follows:
|
W
e
i
g
h
t
e
d
n
u
m
b
e
r
o
f
s
a
m
p
l
e
s
t
r
a
n
s
i
t
i
o
n
i
n
g
b
e
t
w
e
e
n
l
a
t
e
n
t
c
l
a
s
s
e
s
(
g
=
1
t
o
G
)
a
t
t
i
m
e
p
o
i
n
t
s
(
t
=
0
t
o
T
)
=
∑
n
=
1
N
(
π
^
1
n
0
G
|
N
T
×
π
^
2
n
1
G
|
N
T
×
,
…
,
×
π
^
G
n
T
G
|
N
T
)
| (2) |
By aggregating the weighted numbers calculated by Eq. 2 for all transition
patterns, the number of samples transitioning between ADL statuses was
calculated, and a transition diagram of ADL status was constructed. Moreover, we
created a transition diagram of ADL status stratified according to the
corresponding class at the time of admission.
Statistical analysis was performed using LatentGOLD🄬 5.1.0 (Statistical
Innovations, Arlington, MA, USA). Transition diagrams of ADL status were drawn
using Python 3.9.0 (Python Software Foundation, Wilmington, DE, USA).
ETHICS
The Ethics Committee of the Saiseikai Higashikanagawa Rehabilitation Hospital
approved this study. All participants included in the study provided informed
consent using the opt-out method (approval number: 21–04).19)
RESULTS
Patients
From the 373 selected patients, 34 FIM samples with missing values were excluded,
leaving 1592 samples to be included in the analysis. The details on patient
selection are described in our previous report.19)Table 1 shows the patient-to-patient characteristics
at admission, and Table 2 shows the
18 FIM items at each timepoint (t=0 to 6).
Table 1. Patient characteristics
| Patient characteristic |
Total=373 |
| Sex, male |
258 (69%) |
| Age |
|
| <65 years |
139 (37%) |
| 65–74 years |
100 (27%) |
| >74 years |
133 (36%) |
| Missing |
1 (0%) |
| Lesion type |
|
| Hemorrhage |
154 (41%) |
| Infarction |
215 (58%) |
| Infarction with hemorrhage |
4 (1%) |
| Lesion side |
|
| Left |
201 (54%) |
| Right |
155 (42%) |
| Both sides |
17 (5%) |
| Acute treatment, operative |
67 (18%) |
| History of past stroke |
70 (19%) |
| History of past locomotor
disorders |
48 (13%) |
Data given as number (percentage).
Table 2. Proportions of FIM items (%) at each timepoint
| FIM item |
Status |
T0 |
T1 |
T2 |
T3 |
T4 |
T5 |
T6 |
All |
| (n=373) |
(n=373) |
(n=296) |
(n=233) |
(n=170) |
(n=122) |
(n=59) |
(n=1626) |
| Motor |
| Eating |
I |
39 |
58 |
62 |
64 |
57 |
64 |
69 |
57 |
| MD |
46 |
29 |
27 |
26 |
29 |
25 |
17 |
31 |
| CD |
15 |
12 |
11 |
10 |
12 |
11 |
14 |
12 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Grooming |
I |
30 |
47 |
49 |
53 |
47 |
46 |
51 |
45 |
| MD |
43 |
38 |
38 |
36 |
39 |
43 |
37 |
39 |
| CD |
27 |
14 |
13 |
11 |
12 |
11 |
12 |
16 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Bathing |
I |
16 |
30 |
27 |
28 |
21 |
16 |
17 |
24 |
| MD |
45 |
45 |
51 |
52 |
59 |
66 |
68 |
50 |
| CD |
39 |
24 |
21 |
20 |
18 |
18 |
15 |
25 |
| Missing |
0 |
1 |
1 |
0 |
2 |
0 |
0 |
1 |
| Dressing the upper
body |
I |
25 |
42 |
46 |
45 |
37 |
31 |
41 |
38 |
| MD |
37 |
37 |
35 |
36 |
40 |
48 |
41 |
38 |
| CD |
38 |
20 |
19 |
19 |
21 |
21 |
18 |
24 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Dressing the lower
body |
I |
23 |
42 |
44 |
45 |
37 |
30 |
32 |
38 |
| MD |
32 |
29 |
29 |
27 |
32 |
44 |
46 |
31 |
| CD |
45 |
28 |
27 |
28 |
29 |
26 |
22 |
31 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Toileting |
I |
27 |
44 |
49 |
48 |
41 |
41 |
49 |
41 |
| MD |
29 |
29 |
27 |
28 |
33 |
37 |
32 |
30 |
| CD |
44 |
26 |
24 |
24 |
24 |
22 |
19 |
29 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Bladder control |
I |
43 |
56 |
58 |
55 |
48 |
49 |
58 |
52 |
| MD |
13 |
12 |
12 |
13 |
14 |
14 |
5 |
13 |
| CD |
44 |
31 |
30 |
32 |
36 |
37 |
37 |
35 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Bowel control |
I |
46 |
60 |
61 |
61 |
56 |
58 |
59 |
57 |
| MD |
16 |
15 |
15 |
15 |
16 |
14 |
14 |
15 |
| CD |
38 |
24 |
24 |
24 |
26 |
28 |
27 |
28 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Transfer to
bed/chair/wheelchair |
I |
23 |
43 |
49 |
47 |
43 |
42 |
47 |
40 |
| MD |
48 |
43 |
41 |
42 |
43 |
49 |
47 |
45 |
| CD |
29 |
13 |
10 |
11 |
12 |
9 |
6 |
15 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Transfer to toilet |
I |
25 |
43 |
46 |
47 |
40 |
44 |
49 |
40 |
| MD |
40 |
40 |
40 |
39 |
44 |
42 |
39 |
41 |
| CD |
35 |
16 |
14 |
14 |
14 |
14 |
12 |
19 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Transfer to
tub/shower |
I |
7 |
25 |
22 |
21 |
16 |
16 |
22 |
18 |
| MD |
34 |
36 |
44 |
46 |
45 |
46 |
37 |
40 |
| CD |
59 |
38 |
34 |
33 |
37 |
38 |
41 |
42 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Walking or wheelchair
use |
I |
17 |
42 |
48 |
48 |
48 |
51 |
56 |
40 |
| MD |
23 |
31 |
29 |
34 |
34 |
34 |
32 |
30 |
| CD |
60 |
26 |
22 |
18 |
17 |
15 |
12 |
30 |
| Missing |
0 |
1 |
1 |
0 |
1 |
0 |
0 |
0 |
| Stairs |
I |
8 |
25 |
21 |
18 |
14 |
16 |
14 |
17 |
| MD |
30 |
29 |
36 |
38 |
42 |
41 |
47 |
35 |
| CD |
62 |
44 |
40 |
42 |
42 |
43 |
37 |
46 |
| Missing |
0 |
2 |
3 |
2 |
2 |
0 |
2 |
2 |
| Cognitive |
| Comprehension |
I |
36 |
50 |
50 |
51 |
51 |
55 |
64 |
48 |
| MD |
46 |
37 |
41 |
39 |
38 |
38 |
29 |
40 |
| CD |
18 |
12 |
9 |
10 |
9 |
7 |
7 |
12 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Expression |
I |
36 |
53 |
57 |
56 |
55 |
62 |
63 |
52 |
| MD |
42 |
34 |
34 |
32 |
34 |
30 |
29 |
35 |
| CD |
22 |
12 |
9 |
12 |
9 |
8 |
8 |
13 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Social interaction |
I |
51 |
64 |
65 |
66 |
63 |
66 |
69 |
62 |
| MD |
32 |
26 |
28 |
27 |
28 |
28 |
24 |
28 |
| CD |
17 |
9 |
7 |
7 |
7 |
6 |
7 |
10 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Problem-solving |
I |
25 |
37 |
36 |
38 |
34 |
39 |
42 |
34 |
| MD |
43 |
40 |
43 |
43 |
43 |
39 |
41 |
43 |
| CD |
32 |
22 |
21 |
19 |
21 |
22 |
17 |
23 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
| Memory |
I |
32 |
47 |
46 |
48 |
45 |
49 |
61 |
44 |
| MD |
40 |
34 |
38 |
36 |
37 |
34 |
27 |
37 |
| CD |
28 |
18 |
16 |
16 |
16 |
17 |
12 |
19 |
| Missing |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
I, independence; MD, modified dependence; CD, complete dependence.
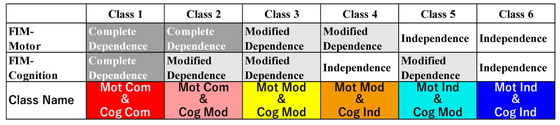
The six latent classes were interpreted as ADL statuses and the names and
characteristics of these classes are shown in Fig. 1. Classes 1–6 were arranged in order of improvement in the
degree of independence in motor items. Class 1 was named “Motor-Complete
Dependence and Cognition-Complete Dependence” because most motor and cognitive
items were assigned to Complete Dependence. Following the same reasoning, the
remaining classes were named as follows: Class 2 was named “Motor-Complete
Dependence and Cognition-Modified Dependence”; Class 3 was named “Motor-Modified
Dependence and Cognition-Modified Dependence”; Class 4 was named “Motor-Modified
Dependence and Cognition-Independence”; Class 5 was named “Motor-Independence
and Cognition-Modified Dependence”; and Class 6 was named “Motor-Independence
and Cognition-Independence”. Further details are provided in our previous
report.19)
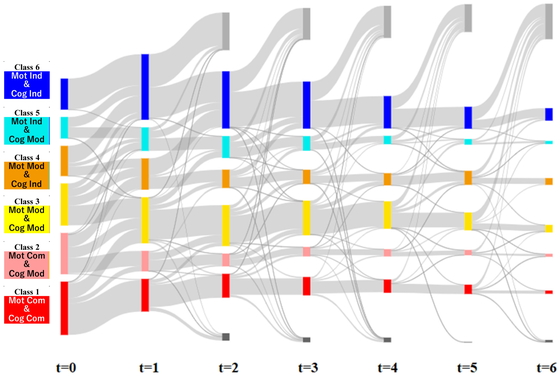
ADL Status Transition
Using the probability that each FIM sample belonged to each class (Class 1–6) at
each timepoint (t=0 to 6) as a weighting, we calculated the number of samples
that transitioned between classes. Fig.
2 shows a transition diagram of the ADL status. Transition diagrams
stratified according to the ADL status at the time of admission are shown in
Fig. 3.
As shown in Fig. 3a, patients within
Class 1 at admission, characterized as Motor-Complete Dependence and
Cognition-Complete Dependence, showed minimal transition towards achieving
independence in ADL status. Most patients in this class transitioned to Class 3
(Motor-Modified Dependence and Cognition-Modified Dependence) where motor items
generally improved to a state of Modified Dependence before discharge. This
transition decreased after t=3. Furthermore, this class showed a home discharge
rate of only 27%, a statistic consistent with findings from previous
studies.19)
As shown in Fig. 3b, some patients
within Class 2 at admission (Motor-Complete Dependence and Cognition-Modified
Dependence) experienced improvements, particularly transitioning to Class 5
(Motor-Independence and Cognition-Modified Dependence) before discharge.
However, a substantial number of patients did not attain motor independence and
left without achieving this goal. It is noteworthy that this transition became
less frequent after t=4. Interestingly, previous studies reported a higher home
discharge rate of 62%.19)
Most patients within Class 3 (Motor-Modified Dependence and Cognition-Modified
Dependence; Fig. 3c) at admission
transitioned to a status superior to Class 5 (Motor-Independence and
Cognition-Modified Dependence) before discharge. However, this transition
declined after t=3. Previous research documented a home discharge rate of
81%.19)
A considerable majority of patients within Class 4 (Motor-Modified Dependence and
Cognition-Independence; Fig. 3d) at
admission transitioned to a status superior to Class 5 (Motor-Independence and
Cognition-Modified Dependence) before discharge. Many of these transitions
occurred within the first timepoint (t=1). Previous studies have reported a high
home discharge rate of 92% for this specific group.19)
Most patients initially categorized as Class 5 (Motor-Independence and
Cognition-Modified Dependence; Fig.
3e) at admission made a transition to the optimal state (Class 6;
Motor-Independence and Cognition-Independence) before discharge. Many of these
transitions occurred within the first timepoint (t=1). Previous studies have
reported an impressive home discharge rate of 95% for this group.19)
For patients initially categorized as Class 6 (Motor-Independence and
Cognition-Independence; Fig. 3f), a
considerable number of patients achieved discharge within the first timepoint
(t=1). Previous studies have consistently reported an impressive home discharge
rate of 98% for this group.19)
DISCUSSION
We categorized six latent ADL statuses by applying LCA to the FIM samples measured
among inpatients with stroke and classifying them into homogeneous classes based on
their combination of responses to the 18 FIM items in a previous study.19) Using these
classification data, we constructed the transition diagrams of ADL status stratified
according to ADL status at admission (Fig.
3). Accordingly, we considered recommendations for interventions based on
the characteristics of ADL status at admission and characteristics of the recovery
process. In the future, the ability to input daily clinical measurements and update
the model with new data will contribute to building a data-driven personalized
medical system directly linked to the management of the facility.
Classification
A qualitative classification of latent ADL status based on the combination of FIM
motor and cognitive items was confirmed. Detailed characteristics of the 18 FIM
items are described in our previous report.19) In the mixed classes, cognitive items are
better in Class 4 (Motor-Modified Dependence and Cognition-Independence) whereas
motor items are better in Class 5 (Motor-Independence and Cognition-Modified
Dependence). According to the transition diagrams of these two ADL statuses at
the time of admission (Fig. 3d,e),
more patients with ADL status showing strong cognitive items at t=1 (Fig. 3d) transitioned to the optimal
state of Class 6 (Motor-Independence and Cognition-Independence) than those with
strong motor items at t=1 (Fig. 3e).
This finding is consistent with previous studies on the effects of cognition on
functional performance.29) The ability to identify differences in how ADL
status improves will be necessary in efforts to structure FIM as a
multidimensional concept, as mentioned in a previous study.30)
ADL Status Transition
In the transition of ADL status, we constructed the transition diagram of ADL
status based on the probability that the FIM sample at each timepoint belonged
to each latent ADL status (Fig. 2).
The transition diagrams were stratified according to the status at the time of
admission (Fig. 3). Previous studies
on the transition through the application of LCA have discussed transition
probabilities over all classes at the time of admission.31,32,33) In this study, by
stratifying the transition diagram based on the class (latent ADL status) at the
time of admission, it was possible to analyze the transitions in ADL status in
terms of the status at admission. The clinical recommendations for each latent
ADL status on admission are described below.
In our analysis, we observed distinct patterns of transition among different ADL
status classes, shedding light on the rehabilitation journey of elderly
patients. For Class 1 patients (Fig.
3a), characterized by severe dependence in both FIM-motor and
FIM-cognitive items at admission, we noted transitions to ADL statuses where
motor items remained non-independent until discharge. Therefore, we consider
that obtaining early informed consent for ADL at discharge and effectively
utilizing social resources are of paramount importance, especially considering
the low home discharge rate (27%).
Class 2 (Fig. 3b), comprising patients
with severe motor and moderate cognitive dependence at admission, exhibited
transitions to ADL statuses with motor independence (Class 5) or further
improvement. Achieving these transitions within t=3 is critical, aligning with
the goal of home discharge (62%) and FIM improvement.
Class 3 (Fig. 3c), representing
patients requiring moderate assistance in motor and cognitive items at
admission, showed transitions to ADL statuses with motor independence (Class 5)
or further improvement. Here, achieving these transitions within t=2 is crucial,
given the substantial home discharge rate (81%).
For Class 4 patients (Fig. 3d),
characterized by moderate motor and independent cognitive assistance at
admission, most transitioned to ADL statuses with motor independence (Class 5)
or better, often within t=1. The high home discharge rate (92%) underscores the
importance of early improvement of ADL status.
Class 5 (Fig. 3e), comprising patients
with independent motor items and requiring modified cognitive assistance at
admission, demonstrated transitions to the best status (Class 6) primarily
within t=1. Prioritizing early ADL improvement and home discharge was evident,
as reflected in the high home discharge rate (95%).
Class 6 patients (Fig. 3f), admitted
with both motor and cognitive independence, achieved discharge within t=1, with
an impressive home discharge rate of 98%. In these patients, emphasizing home
discharge and early discharge is highly recommended. These findings reveal the
diverse trajectories of elderly patients during rehabilitation, emphasizing the
significance of tailored strategies for different ADL status classes, with the
ultimate goal of achieving better outcomes and home discharge.
Study Limitations
In FIM analysis, it is common to use the seven levels of FIM.5,6) However, in this
study, three levels of integrated FIM were used, as was the case in a previous
study.19)
Therefore, there remains scope for future verification of integrated FIM levels
as an abbreviated form of the seven-level FIM.
In this and previous studies, FIM samples from hospitalized patients at several
assessment timepoints were used for classification as a single combined dataset.
When classifying ADL status that appears in FIM response patterns, we analyzed
as many FIM samples as possible to capture a snapshot of all situations between
patients and within patient measurement timepoints, including differences in the
number of timepoints between patients. FIM samples were assumed to be
independent and identically distributed, given the variations in FIM severity
among patients and the fundamental nature of FIM as an assessment tool for ADL.
As shown in previous research, we confirmed that this classification does not
significantly contradict that of the preliminary analysis conducted at each
timepoint. In the future, it will be crucial to consider applying a method of
analysis that aligns better with the structure of the data.
This study did not consider the duration from stroke onset to admission for each
patient. We chose to analyze this setting to focus on improving treatment
regimens in convalescence hospitals. According to the procedures outlined by the
Japanese Health Insurance System, admission to convalescence hospitals is
restricted to a maximum of 60 days from onset, but the duration from onset to
admission varied within this range. This variability may potentially impact the
results and serve as a limitation of this study. Similar studies considering the
effects of duration from onset to admission are needed in the future.
Given that this study was conducted at a single institution, the findings of this
Japanese study may not be fully transferable to populations in other parts of
the world. Although many medical studies strive for enhanced generalizability,
researchers and clinicians must recognize the potential for wide variation in
processes and outcomes of long-term hospitalization for elderly patients with
complex health conditions based on the region and medical facilities.
CONCLUSION
The results of this study suggest that the classification of ADL status and its
transition, based on the characteristics of ADL status and the timing of status
changes, can contribute to improved treatment. To advance data-driven precision
medicine, it is imperative to construct models that are tailored to the unique
attributes of individual regions and facilities. This will involve the utilization
of real-world medical data from these specific settings and continuously refining
the models.
ACKNOWLEDGMENTS
This investigation was supported by the Japan Agency for Medical Research and
Development (Grant no. JP18he0402255h0005). We thank hospital staff for their
collaboration in this study. We thank Editage (www.editage.com) for English language
editing.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Dam M, Tonin P, Casson S, Ermani M,
Pizzolato G, Iaia V, Battistin L: The effects of long-term rehabilitation
therapy on poststroke hemiplegic patients. Stroke 1993;24:1186–1191.
PMID:8342195, DOI:10.1161/01.STR.24.8.1186
- 2. Meyer MJ, Pereira S, McClure A, Teasell
R, Thind A, Koval J, Richardson M, Speechley M: A systematic review of studies
reporting multivariable models to predict functional outcomes after post-stroke
inpatient rehabilitation. Disabil Rehabil 2015;37:1316–1323. PMID:25250807,
DOI:10.3109/09638288.2014.963706
- 3. Brown AW, Lee M, Lennon RJ, Niewczyk PM:
Functional performance and discharge setting predict outcomes 3 months after
rehabilitation hospitalization for stroke. J Stroke Cerebrovasc Dis
2020;29:104746. PMID:32151479,
DOI:10.1016/j.jstrokecerebrovasdis.2020.104746
- 4. Yang DG, Gu R, Sato S, Zheng F, Sano M,
Yashima C, Eguchi J, Ishida T, Kawaguchi M, Kubo J, Kakuda W: The ability for
basic movement scale II can predict functional outcome and discharge destination
in stroke patients. J Stroke Cerebrovasc Dis 2020;29:104484. PMID:31753717,
DOI:10.1016/j.jstrokecerebrovasdis.2019.104484
- 5. Tsuji T, Sonoda S, Domen K, Saitoh E, Liu
M, Chino N: ADL structure for stroke patients in Japan based on the Functional
Independence Measure. Am J Phys Med Rehabil 1995;74:432–438. PMID:8534387,
DOI:10.1097/00002060-199511000-00007
- 6. Linacre JM, Heinemann AW, Wright BD,
Granger CV, Hamilton BB: The structure and stability of the Functional
Independence Measure. Arch Phys Med Rehabil 1994;75:127–132. PMID:8311667,
DOI:10.1016/0003-9993(94)90384-0
- 7. Koyama T, Matsumoto K, Okuno T, Domen K:
Relationships between independence level of single motor-FIM items and FIM-motor
scores in patients with hemiplegia after stroke: an ordinal logistic modelling
study. J Rehabil Med 2006;38:280–286. PMID:16931457,
DOI:10.1080/16501970600731420
- 8. Tokunaga M, Tori K, Eguchi H, Kado Y,
Ikejima Y, Ushijima M, Miyabe S, Tsujimoto S, Fukuda E: The stratification of
motor FIM and cognitive FIM and the creation of four prediction formulas to
enable higher prediction accuracy of multiple linear regression analysis with
motor FIM gain as the objective variable—an analysis of the Japan Rehabilitation
Database. Jpn J Compr Rehabil Sci 2017;8:21–29.
DOI:10.11336/jjcrs.8.21
- 9. Koyama T, Matsumoto K, Okuno T, Domen K:
A new method for predicting functional recovery of stroke patients with
hemiplegia: logarithmic modelling. Clin Rehabil 2005;19:779–789. PMID:16250198,
DOI:10.1191/0269215505cr876oa
- 10. Kimura Y, Yamada M, Hamanaka K, Tanaka N,
Muroh Y: Usefulness of the prediction method based on a logarithmic model for
functional recovery in stroke patients: in case of using the motor-Functional
Independence Measure score. Int J Rehabil Res 2017;40:134–137. PMID:28177943,
DOI:10.1097/MRR.0000000000000219
- 11. Soh CH, Reijnierse EM, Tuttle C, Marston
C, Goonan R, Lim WK, Maier AB: Trajectories of functional performance recovery
after inpatient geriatric rehabilitation: an observational study. Med J Aust
2021;215:173–179. PMID:34137032, DOI:10.5694/mja2.51138
- 12. McCutcheon AL: Latent class analysis. In:
Niemi RG, editor. Quantitative applications in the social sciences. Newbury
Park, CA: Sage; 1987. pp. 4–37.
- 13. Wraith D, Wolfe R: Classifying patients
by their characteristics and clinical presentations; the use of latent class
analysis. Respirology 2014;19:1138–1148. PMID:25302757,
DOI:10.1111/resp.12408
- 14. Kongsted A, Nielsen AM: Latent class
analysis in health research. J Physiother 2017;63:55–58. PMID:27914733,
DOI:10.1016/j.jphys.2016.05.018
- 15. Gariepy G, Malla A, Wang J, Messier L,
Strychar I, Lesage A, Schmitz N: Types of smokers in a community sample of
individuals with Type 2 diabetes: a latent class analysis. Diabet Med
2012;29:586–592. PMID:22004370,
DOI:10.1111/j.1464-5491.2011.03493.x
- 16. Greig F, Hyman S, Wallach E, Hildebrandt
T, Rapaport R: Which obese youth are at increased risk for type 2 diabetes?
Latent class analysis and comparison with diabetic youth. Pediatr Diabetes
2012;13:181–188. PMID:22050535,
DOI:10.1111/j.1399-5448.2011.00792.x
- 17. Butler JC, Bosshardt SC, Phelan M,
Moroney SM, Tondella ML, Farley MM, Schuchat A, Fields BS: Classical and latent
class analysis evaluation of sputum polymerase chain reaction and urine antigen
testing for diagnosis of pneumococcal pneumonia in adults. J Infect Dis
2003;187:1416–1423. PMID:12717623, DOI:10.1086/374623
- 18. Thomas E, Barrett JH, Donn RP, Thomson W,
Southwood TR, British Paediatric Rheumatology Group: Subtyping of juvenile
idiopathic arthritis using latent class analysis. Arthritis Rheum
2000;43:1496–1503. PMID:10902751,
DOI:10.1002/1529-0131(200007)43:7%3c1496::AID-ANR12%3e3.0.CO;2-C
- 19. Furuta H, Mizuno K, Unai K, Ebata H,
Yamauchi K, Watanabe M: Functional Independence Measure subtypes among
inpatients with subacute stroke: classification via latent class analysis. Prog
Rehabil Med 2022;7:20220021. PMID:35528116,
DOI:10.2490/prm.20220021
- 20. Chang WC, Lu FP, Lan TY, Wu SC:
Multidimensional health‐transition patterns among a middle‐aged and older
population. Geriatr Gerontol Int 2013;13:571–579. PMID:22985100,
DOI:10.1111/j.1447-0594.2012.00937.x
- 21. Lafortune L, Béland F, Bergman H, Ankri
J: Health status transitions in community-living elderly with complex care
needs: a latent class approach. BMC Geriatr 2009;9:6. PMID:19192295,
DOI:10.1186/1471-2318-9-6
- 22. Collins LM, Lanza ST: Latent class and
latent transition analysis: with applications in the social, behavioral, and
health sciences. Newark, NJ: Wiley; 2009. pp. 181–224.
- 23. Center for Functional Assessment Research
and the Uniform Data System for Medical Rehabilitation: Guide for use of the
uniform data set for medical rehabilitation including the Functional
Independence Measure (FIM), Version 3.0. Buffalo, NY: State University of New
York; 1990.
- 24. Thorpe ER, Garrett KB, Smith AM, Reneker
JC, Phillips RS: Outcome measure scores predict discharge destination in
patients with acute and subacute stroke: a systematic review and series of
meta-analyses. J Neurol Phys Ther 2018;42:2–11. PMID:29232307,
DOI:10.1097/NPT.0000000000000211
- 25. Chumney D, Nollinger K, Shesko K, Skop K,
Spencer M, Newton RA: Ability of Functional Independence Measure to accurately
predict functional outcome of stroke-specific population: systematic review. J
Rehabil Res Dev 2010;47:17–29. PMID:20437324,
DOI:10.1682/JRRD.2009.08.0140
- 26. Dodds TA, Martin DP, Stolov WC, Deyo RA:
A validation of the Functional Independence Measurement and its performance
among rehabilitation inpatients. Arch Phys Med Rehabil 1993;74:531–536.
PMID:8489365, DOI:10.1016/0003-9993(93)90119-U
- 27. Hachisuka K, Okazaki T, Ogata H:
Self-rating Barthel index compatible with the original Barthel index and the
Functional Independence Measure motor score. J UOEH 1997;19:107–121.
PMID:9194213, DOI:10.7888/juoeh.19.107
- 28. Weller BE, Bowen NK, Faubert SJ: Latent
class analysis: a guide to best practice. J Black Psychol 2020;46:287–311.
DOI:10.1177/0095798420930932
- 29. Zakharova-Luneva E, Cooke DM, Okano S,
Hurst C, Geffen S, Eagles R: The relationship between cognition and functional
outcomes in rehabilitation: FIMCog vs. MoCA. Geriatr Gerontol Int
2020;20:336–342. PMID:32043811, DOI:10.1111/ggi.13884
- 30. Dickson HG, Köhler F: The
multi-dimensionality of the FIM motor items precludes an interval scaling using
Rasch analysis. J Rehabil Med 2019;28:159–162. PMID:8885038,
DOI:10.2340/165019771996283159162
- 31.Furuta H, Bito S, Yamauchi K, Watanabe
M: Exploration for long-term hospitalization factors in elderly patients with
pneumonia focused on the transition of patient conditions [in Japanese]. J Jpn
Soc Health Admin 2019;56:119–131. .DOI:10.11303/jsha.56.119
- 32. Landau S, Harris V, Burn DJ, Hindle JV,
Hurt CS, Samuel M, Wilson KC, Brown RG: Anxiety and anxious-depression in
Parkinson’s disease over a 4-year period: a latent transition analysis. Psychol
Med 2016;46:657–667. PMID:26492977,
DOI:10.1017/S0033291715002196
- 33. Soto-Ramírez N, Ziyab AH, Karmaus W,
Zhang H, Kurukulaaratchy RJ, Ewart S, Arshad SH: Epidemiologic methods of
assessing asthma and wheezing episodes in longitudinal studies: measures of
change and stability. J Epidemiol 2013;23:399–410. PMID:23994864,
DOI:10.2188/jea.JE20120201