ABSTRACT
Background: Magnetic stimulation devices can be large because of the
need for cooling systems. We developed a compact and lightweight Spinning
Permanent Magnet (SPM) device that generates magnetic fields with intensities
below the motor threshold. In this report, we present the case of a post-stroke
patient in which an immediate reduction in spasticity of the ankle plantar
flexors was achieved after SPM treatment.
Case: A 37-year-old man was admitted to our hospital with a right
putamen hemorrhage. The patient underwent conservative therapy and exhibited
residual left hemiplegia and spasticity. Three months after stroke onset, he was
able to walk with supervision while using a left ankle–foot orthosis and a
T-cane. The Modified Ashworth Scale (MAS) score of the left ankle plantar
flexors was 1+. The plantar flexors were stimulated by SPM treatment. The
outcomes were the Hmax/Mmax of the tibial nerve (soleus muscle) and the MAS
score. On the first day, SPM stimulation was applied for 30 min. On the second
day, a sham stimulation of the same duration was performed. On the third day,
the SPM stimulation was repeated. Hmax/Mmax decreased from 41.5% to 37.7% on the
first day, and from 46.9% to 31.6% on the third day after SPM stimulation. The
MAS score decreased from 1+ to 1 on both days. In contrast, after sham
stimulation, Hmax/Mmax increased from 39.2% to 44.2%, whereas the MAS score
remained unchanged at 1+.
Discussion: Stimulation below the motor threshold using SPM
treatment can effectively reduce spasticity.
INTRODUCTION
Spasticity is a sensorimotor control disorder that results from an upper motor neuron
(UMN) lesion that presents as intermittent or sustained involuntary muscle
activation.1) It
is a common complication of stroke2) and it can have a disabling effect on stroke
survivors because of pain and reduced mobility, which may limit the potential
success of rehabilitation.3)
A systematic review of non-pharmacological interventions for spasticity in adults
showed moderate evidence for electro-neuromuscular stimulation and acupuncture as
adjunctive therapies to conventional routine care (pharmacological and
rehabilitation) in post-stroke patients.4) In addition, transcutaneous electrical stimulation
(TENS), which provides stimulation below the motor threshold, effectively reduces
spasticity.5)
The 2021 Japanese Guidelines for the Management of Stroke recommended TENS as a
Grade A treatment for spasticity in patients with stroke, along with botulinum toxin
A injection, phenol block, brace treatment, intrathecal baclofen, and oral muscle
relaxants as Grade B treatments.6) However, TENS requires an electrode attachment,
which can cause skin irritation.
Peripheral magnetic stimulation (PMS) can stimulate target nerves and muscles without
using electrodes or clothing. PMS of the extremities is also effective in reducing
spasticity even after a single session.7) Furthermore, PMS has the added advantage of causing
less pain than electrical stimulation, because it does not directly stimulate pain
receptors in the skin.8)
PMS devices are typically bulky; however, devices delivering stimulation intensity
below the motor threshold can be downsized. In this report, we present a case in
which we observed immediate reduction in the spasticity of the ankle plantar flexors
in a post-stroke patient after treatment with a Spinning Permanent Magnet (SPM)
device.
SPM Device
We have developed a compact and lightweight magnetic stimulation device (SPM
device), which generates magnetic fields by spinning a disc-shaped permanent
magnet with a motor (Fig.
1).9)
It can easily be attached to a limb using a Velcro strap.
CASE
This study was approved by the Fujita Health University Certified Review Board and
was registered with the Japan Registry of Clinical Trials (Registration No.
jRCTs042200013). Written informed consent was obtained from the patient for use of
the SPM device and for publication of this case report. This study conformed to the
CARE guidelines.10)
A 37-year-old man who had suffered a right frontal subcortical hemorrhage was
admitted to our hospital on the day of onset in 2021. Figure 2 shows a computed tomography scan of the head. The
patient had kidney cancer and was taking antineoplastic medications. Conservative
treatment was undertaken for subcortical hemorrhage, and rehabilitation was
initiated on the day of onset with 100–120 min of physical therapy and 40–60 min of
occupational therapy, five times a week. The patient had left hemiplegia, and a left
ankle–foot orthosis was fabricated approximately 7 weeks after onset. The orthosis
was a shoehorn brace that controlled ankle dorsiflexion and plantar flexion by
utilizing the flexibility of plastic. The initial dorsiflexion angle of the brace
was set at 5 degrees. A WalkAide® device (Innovative Neurotronics, Austin, TX, USA)
was also prescribed approximately 9 weeks after onset. The patient engaged in
walking exercises with both the orthosis and the WalkAide to enhance ankle stability
and activate ankle dorsiflexion. Three months after onset, he was able to walk with
the support of the orthosis and a T cane. He discontinued the use of the WalkAide at
this time because he did not have any significant ankle functional improvement after
3 weeks and we believed that an increase in walking could potentially yield further
functional improvements in the future. The patient gave the following Stroke
Impairment Assessment Set motor item (SIAS-M) scores: hip flexion, 2; knee
extension, 2, and foot-tap test, 1. Spasticity of the left limbs developed
gradually, and the Modified Ashworth Scale (MAS) score of the left ankle plantar
flexors was 1+. The dorsiflexion angle was 5 degrees with the knee extended, and the
ranges of motion of other joints in the lower extremity were normal. Deep tendon
reflexes of the left side increased, and left ankle clonus was sustained for more
than 30 s. The Manual Muscle Test score for the right lower extremity was 5.

The Functional Independence Measure scores were 73 for motor function and 35 for
cognition. Thirteen weeks after onset, use of the SPM was initiated to reduce the
spasticity of the patient’s left ankle plantar flexors.
The left ankle plantar flexors were stimulated in the prone position with the SPM
device placed on the posterior portion of the lower leg at the point of maximum
circumference (see Fig. 1). On the first
day, SPM stimulation was applied for 30 min. On the second day, the device was
attached to the same location but was not turned on (sham stimulation). On the third
day, the SPM stimulation was repeated. The primary outcomes were the maximal
amplitude of the H-reflex as a percentage of the maximal M response (Hmax/Mmax) of
the tibial nerve (soleus) and the MAS score. The secondary outcome was the 10-m
walking time when walking with a T-cane and ankle–foot orthosis. Electromyography
was performed using a Neuropack X1 MEB-2300 (Nihon Kohden, Tokyo, Japan). The
recording electrode was placed on the left soleus, the reference electrode was
located 5 cm distal to it, and stimulation was performed at the popliteal fossa. We
also recorded and analyzed gait while the patient walked with the T-cane but without
the orthosis. Evaluations were conducted three times daily: before stimulation,
immediately after stimulation, and 24 h after stimulation.
On the first day after stimulation, Hmax/Mmax decreased from 41.5% to 37.7%, and the
MAS score decreased from 1+ to 1 (Fig. 3
and Table 1). On the second day, both
Hmax/Mmax and the MAS score were increased before stimulation. After sham
stimulation, Hmax/Mmax increased from 39.2% to 44.2% and the MAS score remained
unchanged at 1+. On the third day after stimulation, Hmax/Mmax decreased from 46.6%
to 30.3% and the MAS score decreased from 1+ to 1. Hmax/Mmax and MAS score increased
to 44.2% and 1+, respectively, on the fourth day. The 10-m walk time with the T-cane
and orthosis showed a trend of improvement on all days: on the first day, it was
11.6 s before stimulation, 11.34 s immediately after stimulation, and 11.22 s at
24 h after stimulation. On the second day, it was 11.07 s immediately after
stimulation and 10.95 s at 24 h after stimulation. On the third day, it was 10.03 s
immediately after stimulation and 9.74 s at 24 h after stimulation.
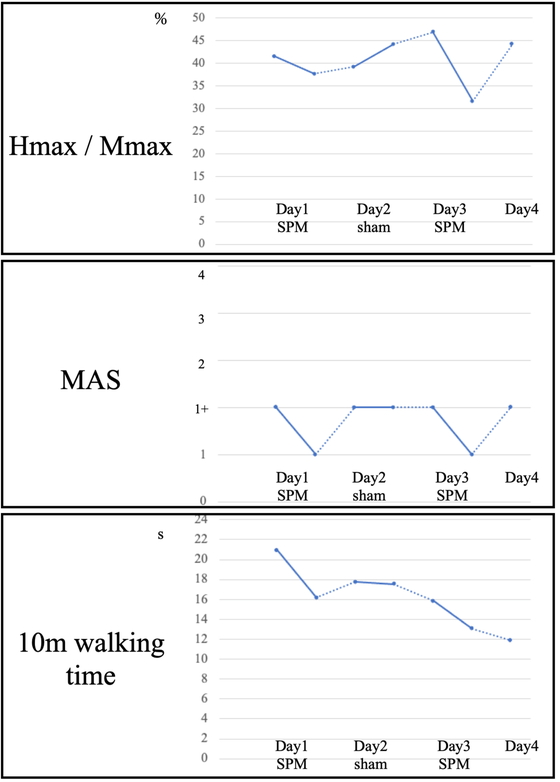
Table 1. Data for Hmax/Mmax, H-amplitude maximum, and M-amplitude maximum before
and after SPM or sham treatment over 4 days
|
Day 1 |
Day 2 |
Day 3 |
Day 4 |
| Time course (h) |
0 |
0.5 |
24 |
24.5 |
48 |
48.5 |
72 |
|
Pre-stim |
Post-stim |
Pre-stim |
Post-stim |
Pre-stim |
Post-stim |
Pre-stim |
|
SPM |
Sham |
SPM |
|
| Hmax/Mmax (%) |
41.5 |
37.7 |
39.2 |
44.2 |
46.6 |
30.3 |
44.2 |
| H-amplitude max (mV) |
9.5 |
9.2 |
9.2 |
10.9 |
9.7 |
6.4 |
8.6 |
| M-amplitude max (mV) |
22.9 |
24.5 |
23.5 |
24.6 |
20.8 |
21.0 |
19.4 |
Pre-stim, before stimulation; Post-stim, immediately after stimulation.
A video recording of the gait with a T-cane and without the orthosis before
stimulation on the first day (Movie 1, Suppl. Video 1) is shown as part of Fig. 4. The video shows that initial foot
contact was with the forefoot. However, Movie 2 (Fig. 4, Suppl. Video 2), which was recorded after stimulation, shows
initial foot contact on the heel. Moreover, 24 h after stimulation on the first day,
the foot-tap test score on the SIAS-M increased from 1 to 2, and the score continued
to be 2 until the end of the study.

After the conclusion of this study, the patient was discharged to another hospital
for further evaluation of his kidney cancer and was readmitted to our hospital for
additional cancer treatment. The patient experienced recurrent cranial hemorrhage
because of brain metastasis, which worsened the left hemiplegia. Despite this,
rehabilitation with magnetic stimulation was continued, and botulinum toxin A was
injected to treat the remaining spasticity in the left tibial posterior,
gastrocnemius, and soleus muscles. The patient was discharged and was able to walk
independently with the orthosis and T-cane at 8 months after onset. No adverse
effects were detected with the long-term use of magnetic stimulation using the SPM
device.
DISCUSSION
We present a case in which immediate reduction in spasticity in the ankle plantar
flexors of a stroke patient was observed after treatment with an SPM device. This
compact device, which provides magnetic stimulation below the motor threshold, has
not been described in previous studies. The patient’s spasticity improved
immediately following SPM stimulation, as evidenced by favorable changes in
Hmax/Mmax and the MAS score and observed improvements in gait.
In clinical practice, Hmax/Mmax is often used as a reliable indicator of
spasticity.11)
Hmax represents the number of excited alpha motor neurons in the anterior horn of
the spinal cord when the input from group Ia fibers is maximized through electrical
stimulation. In contrast, the Mmax indicates the amplitude of the muscle action
potential when all the alpha motor neurons dominating the muscle are synchronously
excited. Therefore, the Hmax/Mmax reflects the fraction of excited alpha motor
neurons among all alpha motor neurons that dominate the target muscle during
electrical stimulation. According to a previous study among 24 stroke patients and
12 age-matched healthy individuals, the mean Hmax/Mmax of the tibial nerve on the
affected side, with the patient in the prone position, was higher in stroke patients
(37.95% ± 15.16%) than in healthy individuals (26.88% ± 11.88%).12) The Hmax/Mmax of our
patient’s affected spastic leg was similar to that of stroke patients in a previous
study, although it improved to some degree after SPM stimulation. We speculate that
the Hmax/Mmax observed before stimulation on Day 3 was higher than that observed
before stimulation on Day 1 because of a decrease in the M wave. Although we made
efforts to place the electrode in the same position and each examination was
conducted with supramaximal stimulation, some factors such as muscle fatigue or body
temperature also affect the height of the M wave.13) Such effects need to be carefully
considered.
The phenomenon of spasticity is attributed to the hyperexcitability of the stretch
reflex mediated by Ia afferents, which is caused by loss of inhibition in the dorsal
reticulospinal tract.14) We believe that the underlying mechanism
responsible for the effect of SPM is presynaptic inhibition of hyperactive stretch
reflexes and reduced co-contraction of spastic antagonist muscles, which is similar
to the effect of TENS.15)
The use of SPM treatment has several advantages. The SPM device does not produce a
tingling sensation because it does not stimulate the skin pain receptors, as is the
case with PMS. Another advantage of SPM treatment is its ease of use. The device is
lightweight with a rechargeable battery and can be easily attached to limbs using a
Velcro strap. This allows patients with the SPM device attached to their limbs to
perform exercises in relative comfort.
This study was limited in that it involved a single case and showed only the
immediate effects of SPM treatment. Therefore, the long-term effects of the
treatment should be evaluated in a large sample size.
CONCLUSION
We report a post-stroke case in which an immediate reduction in ankle plantar flexor
spasticity was achieved after treatment with an SPM device. Our findings suggest
that magnetic stimulation using the SPM device, which provides stimulation below the
motor threshold, may be useful for immediate reduction of spasticity.
ACKNOWLEDGMENTS
This work was supported by a Grant-in-Aid for Scientific Research from the Japan
Society for the Promotion of Science (Grant No. JP21K17520). This case report was
presented at the 6th autumn meeting of the Japanese Association of Rehabilitation
Medicine in Okayama, Japan, on November 4, 2022. We thank Editage (www.editage.com)
for English language editing of a draft version of this report.
CONFLICTS OF INTEREST
Hitoshi Kagaya is listed as an inventor on a patent pending for the SPM device. The
remaining authors declare no conflict of interest.
REFERENCES
- 1. Pandyan AD, Gregoric M, Barnes MP, Wood
D, Wijck FV, Burridge J, Hermens H, Johnson GR: Spasticity: clinical
perceptions, neurological realities and meaningful measurement. Disabil Rehabil
2005;27:2–6. PMID:15799140, DOI:10.1080/09638280400014576
- 2. Li S, Francisco GE: New insights into the
pathophysiology of post-stroke spasticity. Front Hum Neurosci 2015;9:192.
PMID:25914638, DOI:10.3389/fnhum.2015.00192
- 3. Ward AB: A literature review of the
pathophysiology and onset of post-stroke spasticity. Eur J Neurol 2012;19:21–27.
PMID:21707868, DOI:10.1111/j.1468-1331.2011.03448.x
- 4. Khan F, Amatya B, Bensmail D, Yelnik A:
Non-pharmacological interventions for spasticity in adults: an overview of
systematic reviews. Ann Phys Rehabil Med 2019;62:265–273. PMID:29042299,
DOI:10.1016/j.rehab.2017.10.001
- 5. Mahmood A, Veluswamy SK, Hombali A,
Mullick A, N M, Solomon JM: Effect of transcutaneous electrical nerve
stimulation on spasticity in adults with stroke: a systematic review and
meta-analysis. Arch Phys Med Rehabil 2019;100:751–768. PMID:30452892,
DOI:10.1016/j.apmr.2018.10.016
- 6. Japan Stroke Society: Japanese guidelines
for the management of stroke: 2021 [in Japanese]. Kyowa Kikaku, Tokyo,
2021.
- 7. Struppler A, Havel P, Müller-Barna P:
Facilitation of skilled finger movements by repetitive peripheral magnetic
stimulation (RPMS)—a new approach in central paresis. NeuroRehabilitation
2003;18:69–82. PMID:12719622, DOI:10.3233/NRE-2003-18108
- 8.Abe G, Oyama H, Liao Z, Honda K,
Yashima K, Asao A, Izumi S: Difference in pain and discomfort of comparable
wrist movements induced by magnetic or electrical stimulation for peripheral
nerves in the dorsal forearm. Med Devices (Auckl) 2020;13:439–447.
PMID:33376417, DOI:10.2147/MDER.S271258
- 9. Kagaya H: Peripheral magnetic stimulation
(PMS) [in Japaanese]. Jpn J Rehabil Med 2022;59:461–466.
DOI:10.2490/jjrmc.59.461
- 10. Gagnier JJ, Kienle G, Altman DG, Moher D,
Sox H, Riley D, CARE Group: The CARE guidelines: consensus-based clinical case
reporting guideline development. Glob Adv Health Med 2013;2:38–43.
PMID:24416692, DOI:10.7453/gahmj.2013.008
- 11. Kai S, Nakabayashi K: Evoked EMG makes
measurement of muscle tone possible by analysis of the H/M ratio.
Electrodiagnosis N Front Clin Res 2013;2013:195–212.
DOI:10.5772/55783
- 12.Qin W, Zhang A, Yang M, Chen C, Zhen
L, Yang H, Jin L, Li F. Soleus H-reflex change in poststroke spasticity:
modulation due to body position. Neural Plast 2021;2021:9955153. PMID:34917144,
DOI:10.1155/2021/9955153
- 13. Rodriguez-Falces J, Place N:
Determinants, analysis and interpretation of the muscle compound action
potential (M wave) in humans: implications for the study of muscle fatigue. Eur
J Appl Physiol 2018;118:501–521. PMID:29282530,
DOI:10.1007/s00421-017-3788-5
- 14. Sheean G, McGuire JR: Spastic hypertonia
and movement disorders: pathophysiology, clinical presentation, and
quantification. PM R 2009;1:827–833. PMID:19769916,
DOI:10.1016/j.pmrj.2009.08.002
- 15.Levin MF, Hui-Chan CW. Relief of
hemiparetic spasticity by TENS is associated with improvement in reflex and
voluntary motor functions. Electroencephalogr Clin Neurophysiol.
1992;85:131–142. PMID:1373366, DOI:10.1016/0168-5597(92)90079-q
