Age of Adolescent Female Soccer Players at First Ankle Sprain and Menarche
2023 Volume 8 Article ID: 20230042
Details
2023 Volume 8 Article ID: 20230042
Objectives : To provide targeted interventions for the prevention of first ankle sprains, this study determined the prevalence of ankle sprains in female adolescent soccer players and analyzed the correlation between the age at the first occurrence of ankle sprain and the age at menarche.
Methods : The study included 131 female participants from three club teams. The mean age was 13.37 ± 0.96 years. A survey was conducted using a questionnaire that requested information regarding the age at which the first ankle sprain occurred, age at menarche, status of ankle problems, extent to which the ankle joint problem affected playing ability, use of medical facilities or other healthcare facilities for the first or recurrent ankle sprains, and methods used to care for their ankle.
Results: Ankle sprains most commonly occurred for the first time at 12 years, followed by the ages of 13, 10, and 11 years. About 25% of participants experienced their first ankle sprain at the age of menarche, 20% at 1 year after menarche, and 16% a year before menarche. The incidence of the first ankle sprain was high in the second and fifth years after starting to play soccer. Medical treatment was rarely received for the second or subsequent injury, although 36% had some sequelae.
Conclusions: Adolescent female soccer players were not injured early in their soccer careers. Most players experienced their first ankle sprain at the age of 12 years, which was at or close to the age of menarche.
Ankle sprains are one of the most common sports injuries,1) accounting for 15% of all athletics injuries.2) Many risk factors for ankle sprains have been reported, including young age, high body mass index, weight gain, joint laxity, asymmetry in eccentric ankle plantar flexion strength,3) female gender,4) history of ankle sprains, and decreased proprioceptive sensibility.5) A study reported that the risk of re-injury to athletes with a history of an ankle sprain is approximately five times higher than athletes without a history.6) Therefore, prevention of the first ankle sprain is crucial for athletes to deliver their best performance.
When individuals engage in a particular sport during childhood, there is a high chance of experiencing sports injuries because of physical underdevelopment7) and excessive training.8) Sports injuries that occur during adolescence can be influenced by variations in physical maturation among individuals.9)
In girls, adolescence refers to the stage of physical development that starts with the appearance of secondary sexual characteristics and continues from menarche to a regular menstrual cycle. This period of adolescence typically spans from about 8 to 18 years of age. The occurrence of sports injuries in female athletes can be influenced by the disparity among physical attributes, such as joint range of motion and muscle development at the onset of menarche.10) Furthermore, female athletes at the onset of menarche may suffer from dysmenorrhea or premenstrual syndrome,11) which include psychological and physical symptoms that may also impact their susceptibility to sports injuries. Ligament laxity in the knee joint can fluctuate during the menstrual cycle.12) In addition, some studies have demonstrated a high incidence of anterior cruciate ligament (ACL) injury during the ovulatory or luteal phase and preovulatory phase13); however, a unanimous opinion regarding this perspective has not yet been established. These findings have been investigated with respect to estrogen and progesterone levels. Recently, relaxin, which is released during the luteal phase,14) has been reported to affect collagen degradation, thereby affecting ligament laxity and increasing the risk of ACL injury. From these perspectives, menarche could be implicated in sports injuries among adolescent female athletes.15) Currently, a relationship between female hormone levels and ankle ligament laxity is not evident; however, hormonal fluctuations might increase the risk of ankle sprains.
Athletes that compete with an ankle injury not only perform below their best ability and risk losing in competition but also may have negative psychological problems.4) A study reported that 40%–50% of acute ankle sprains lead to chronic ankle instability (CAI).16) Ankle sprains may also lead to long-term osteoarthritis of the ankle. Secondary prevention involves the early identification of athletes at high risk of ankle sprains and the provision of focused intervention and education to prevent the first ankle sprain. These steps can improve athlete performance and promote participation in sports for life, thereby leading to improved health outcomes. Therefore, it is important to clarify the actual situation regarding ankle sprains in adolescent girls, including the status of CAI. Many factors are responsible for sports injuries in adolescent girls. To the best of our knowledge, an analysis of ankle sprains in adolescent female soccer players has not yet been reported.
To guide the secondary prevention of ankle sprains, this study aimed to investigate the occurrence of ankle sprains in adolescent female soccer players by examining the relationship between the age of players at the first sprain and the age at menarche, which is an important indicator of physical maturity. We hypothesized that the incidence of ankle sprains increases around the time of menarche, which is characterized by changes in physique and alterations in female hormone levels.
This retrospective cross-sectional study was approved by the Ethical Review Committee of the International University of Health and Welfare (Approval No. 19-Io-136). Three soccer teams from regional clubs in Chiba and Hyogo prefectures were invited to participate in the study by the prefectural soccer associations. A total of 131 female soccer players participated in the study. The participants played soccer twice on weekdays for approximately 2 h, with one or two additional sessions on weekends, which included practice or games.
The purpose of the study was verbally explained to the participants and through written forms, and the participants and their guarantors provided written consent. To check for missing answers, the questionnaire requested the name of the participant. Questionnaires were distributed to the players at their practice stadiums and were collected later. The period between the distribution and collection of the questionnaires was less than 3 weeks. The survey was conducted from January 2020 to July 2022.
The questionnaire form supplied to the participants is shown in Table 1. The questionnaire was developed based on questionnaires used in two previous studies,17,18) which were originally designed to investigate the actual conditions of ankle sprain injuries17) and treatment behaviors after ankle sprain injuries18) among female college soccer players. These questionnaires were considered appropriate for the junior high school and high school players in the current study. In addition, a question regarding the occurrence and time of menarche was added. A draft questionnaire form was checked by two junior high school athletes to ensure that it could be easily interpreted by the participants.
| Name: | Date of Birth: / / | |||
| Please put your answer in parentheses or check (✓) where applicable to you. | ||||
| # Age: | 7) Did you see a doctor or other healthcare specialist for the second or subsequent sprain? | |||
| [ ] years | ||||
| # Grade: | □ Every time → move to 8) | |||
| □ Junior high school [ ] grade | □ Sometimes → move to 8) | |||
| □ High school [ ] grade | □ Not at all → move to 9) | |||
| # Dominant leg (kicking leg) | 8) Where did you receive medical care? Select all answers that apply to you. | |||
| □ Right | ||||
| □ Left | □ Hospital | |||
| # Soccer career | □ Orthopedic clinic | |||
| □ Before elementary school [ ] years | □ Osteopathic care | |||
| □ Elementary school [ ] years | □ Other ( ) | |||
| □ Junior high school [ ] years | 9) Currently, do you have problems with your ankles when you are playing soccer? | |||
| □ High school [ ] years | ||||
| # Age you started playing soccer | □ Yes → move to 10) | |||
| [ ] years | □ No → move to 12) | |||
| 1) Have you ever sprained your ankle? | 10) What problems (feelings) do you have? Select all answers that apply to you. | |||
| □ Yes→ move to 2) | ||||
| □ No→ move to 14) | □ I will likely have another sprain | |||
| 2) Which ankle did you sprain? | □ I get sprains repeatedly | |||
| □ Right | □ I have pain | |||
| □ Left | □ I feel strange | |||
| □ Both | □ My ankle joint catches | |||
| 3) How old were you when you first sprained your ankle? | □ Other ( ) | |||
| 11) Are you caring for your ankle? | ||||
| □ Right [ ] years old | □ Yes → move to 12) | |||
| □ Left [ ] years old | □ No →move to 14) | |||
| 4) How many times have you had a sprained ankle? | 12) How are you taking care of your ankle? Select all answers that apply to you. | |||
| □ Right [ ] times | ||||
| □ Left [ ] times | □ Taping | |||
| 5) Did you visit a doctor or healthcare specialist for your first sprain? | □ Regularly receive medical care | |||
| □ Muscle training or rehabilitation | ||||
| □ Yes → move to 6) | □ Other ( ) | |||
| □ No → move to 7) | 13) How is your soccer performance affected by your ankle problem? | |||
| 6) Which medical care did you receive? | ||||
| □ Hospital | □ Performance considerably decreased | |||
| □ Orthopedic clinic | □ Performance slightly decreased | |||
| □ Osteopathic care | □ No effect | |||
| □ Other ( ) | 14) Have you had your first menstruation? | |||
| □ Yes → When? [ ] years old | ||||
| □ No | ||||
Ankle sprain is an acute injury resulting from sudden trauma that is typically characterized by an ankle ligamentous sprain caused by explosive inversion or eversion.19) In this study, ankle sprains were defined as those that occurred while playing soccer and included both lateral and medial ankle sprains. The severity of the injury and whether it was diagnosed by a physician were not assessed in this study.
Data were analyzed using SPSS statistics version 20.0 (IBM, Tokyo, Japan). The analyses included descriptive statistics. Wilcoxon’s signed rank test, uncorrelated t-test, χ2 test, and one-way analysis of variance were used, and a risk rate of 5% was used as the significance level.
The questionnaire collection rate was 95%. After excluding two respondents with missing values that could not be confirmed, the valid response rate was 94%. The mean age of the participants was 13.37 ± 0.96 years (Tables 2 and 3). The mean age at which participants started to play soccer was 7.33 ± 1.77 years, and the mean number of years of playing soccer was 6.26 ± 2.00 years.
| Age (years) | Number of participants (n = 131) |
| 12 | 27 (21%) |
| 13 | 46 (35%) |
| 14 | 42 (32%) |
| 15 | 15 (12%) |
| 16 | 1 (1%) |
| School grade | Number of participants (n = 131) | Number with ankle sprain (n = 61) | |
| Junior high school | First grade | 52 (40%) | 20 |
| Second grade | 41 (31%) | 21 | |
| Third grade | 34 (26%) | 18 | |
| High school | First grade | 4 (3%) | 2 |
Sixty-one (47%) participants experienced 138 ankle sprains. The mean age at which the first ankle sprain was experienced was 11.69 ± 1.61 years. Twenty-one (34%) participants were 12 years old, which was the most common age of experiencing the first ankle sprain (Fig. 1). Participants who had not experienced ankle sprain at the time of the survey might experience them in the future; therefore, we calculated the age at which they had their first injury by school grade. Eight (40%) first-grade junior high school players and eight (38%) second-grade junior high school players had the first ankle sprain at 12 years old. Among the participants in the third grade and high school groups, five (25%) players aged 12 years and five (25%) players aged 13 years had experienced ankle sprain. These were the most common ages to experience first ankle sprains.
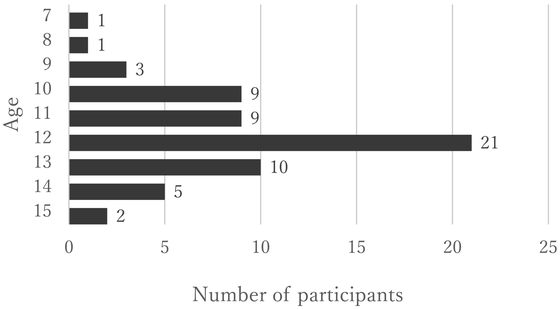
Age distribution of participants who experienced their first ankle sprain (n = 61).
The mean length of time between the first ankle sprain and starting to play soccer was 4.37 ± 2.41 years. The incidence of first ankle sprain was high in the second (second-year group) and fifth (fifth-year group) years of playing soccer (Fig. 2). The first ankle sprains did not occur early in the players’ soccer careers. Comparison of the second-year and fifth-year groups revealed that the respective ages at which they started playing soccer were 8.08 ± 1.62 and 7.0 ± 1.13 years and the respective ages at which they experienced the first ankle sprain were 10.08 ± 1.62 and 12.0 ± 1.13 years; there was no significant difference between these ages. At the time of data collection, the respective ages of participants in the second-year and fifth-year groups were 13.5 ± 0.91 and 13.5 ± 1.17 years (no significant difference). However, six (50%) participants in the second-year group had not experienced menarche at the time of the survey, whereas all the participants in the fifth-year group had experienced menarche.

Frequency distribution for the number of years after which soccer players experienced their first ankle sprain (n = 61).
Of the 51 participants who had experienced menarche and their first ankle sprain, 13 (25%) had their first ankle sprain at the age of menarche, 10 (20%) had their first ankle sprain a year after menarche, and 8 (16%) had their first ankle sprain a year before menarche (Fig. 3). In terms of school grade level, 5 (33%) players in first-grade junior high school had their first ankle sprain a year before menarche and 4 (25%) players in second-grade junior high school experienced their first ankle sprain a year after menarche. A total of 5 (25%) players in third-grade junior high school and high school experienced their first ankle sprain at the age of menarche.

Frequency distribution for the number of years between menarche and the first ankle sprain (n = 51).
Forty-six (75%) participants received medical treatment or other attention for their first ankle sprain, whereas 15 (25%) participants did not receive any treatment for the same. Of the participants who experienced an ankle sprain more than once, 16 (53%) received medical treatment or other attention for all the injuries, 7 (23%) did not receive treatment in some instances, and 6 (20%) did not receive any treatment.
At the time of data collection, 21 (34%) participants indicated that they had some problems with their ankle condition, whereas 38 (62%) participants reported that they had no problem. Of those with ankle problems, 8 (38%) participants indicated that they were likely have a sprain again, 3 (14%) indicated that they get sprains repeatedly, 7 (33%) reported having pain, 7 (33%) mentioned that their ankle felt strange, 1 (5%) indicated that her ankle joint catches, and 2 (10%) mentioned other problems.
Of the participants with ankle problems, 3 (14%) participants regarded their playing performance as obviously decreased, 9 (43%) participants considered their performance to be slightly decreased, and 7 (33%) participants reported no effect on their soccer performance. Among these, 12 (57%) were coping in some way: 6 (29%) participants were using tape, 4 (19%) received regular medical care or other care, and 4 (19%) were undertaking muscle training or rehabilitation.
In a review of the incidence and prevalence of ankle sprain injuries, Doherty et al.4) revealed that the risk of ankle sprains was high among early adolescents, although their report was not limited to those who experienced their first ankle sprain. Female residents diagnosed with an ankle sprain at emergency hospitals in the United Kingdom were often aged 10–14 years.20) Ankle sprain injuries most commonly occurred at the age of 12 years in the current study, thus similar results were observed to previous reports. Therefore, preventive education and intervention for the treatment of ankle sprains is probably required before the age of 10 years. Factors that increased the incidence of the first ankle sprain during this period were identified. Regarding the development of coordinated movements, it is considered that underdeveloped movement patterns may increase the risk of sports injuries in children and adolescents.21) The development of movement patterns is a major factor in the occurrence of sports injuries. Therefore, underdeveloped movement patterns can be viewed as a contributing factor to the increased risk of ankle sprain in early adolescents when compared with that in adults. In addition, peak height velocity age (PHVA) for girls ranges between 11 and 13 years.22) Power, balance, and sprinting ability tend to improve significantly during this period.23) However, an imbalance between bone and muscle growth increases the risk of sports injuries.24) Although not investigated in this study, the high incidence of first ankle sprains at the ages of 10 and 13 years may be related to the physical growth imbalance at the PHVA.
Given that soccer is associated with a high risk of ankle sprain,9) the activity itself should be recognized as a contributing factor to sprain injuries. However, given that the mean duration between the time of starting to play soccer and the first ankle sprain was 4.37 ± 2.41 years, it is difficult to suggest that participants experienced their first ankle sprain soon after starting to play soccer. Furthermore, comparisons between the second-year and fifth-year groups revealed no significant differences for age of the first ankle sprain, age of starting to play soccer, or age at the time of the survey. However, participants in the second-year group had not experienced menarche at the time of the survey. It has been reported that because physical growth is delayed, late-maturing athletes are more prone to injury than early maturing athletes.9) Participants in the second-year group may have been late-maturing athletes.
In girls, menarche is associated with a somatic fat level above a specific threshold.25) Evidence suggests that in mature women, maintaining a certain level of somatic fat is necessary for a regular ovulatory cycle.26) In this study, most participants experienced their first ankle sprain at the age of menarche or 1 year before or after menarche. This result suggests that menarche was associated with the occurrence of the first ankle sprain. During the ovulation phase, postural sway and muscle elasticity tend to increase. Estrogen increases the laxity of ligaments and muscles during the menstrual cycle, which may influence postural stability.27) Because this study did not investigate the relationship between ankle sprain and the menstrual cycle, it is unclear whether female hormones secreted at menarche increased ligament laxity or postural sway, which could have contributed to ankle strain in the participants.
In soccer, the change in playing conditions when a player shifts from an elementary school to a junior high school can increase the incidence of first ankle sprain. The size and weight of the ball and the size of the field increase as the players transit from elementary school to junior high school. Furthermore, there is no under-12 soccer league for girls in Japan so that most female players of this age participate in mixed teams in recreational weekend sport. However, when these players move to junior high school, they have the opportunity to play in highly competitive female-only teams; therefore, they extend their practice time and increase the number of games played. To compensate for the small number of competitive athletes, sixth graders in elementary school occasionally play with junior high school athletes. In this study, most participants started playing soccer during or before joining elementary school and experienced the aforementioned change. Therefore, any inability of players to adapt to this environmental change in terms of their physical capabilities may affect their susceptibility to ankle sprain injuries.
Overall, 47% of the participants in the present study had a history of ankle sprain. A previous study reported that 72.2% of players in the Japan women’s soccer team had a history of ankle sprains.28) It is expected that the number of ankle sprains will increase as the participants continue to play soccer. In the present study, 36% of the study participants with a history of ankle sprain reported ankle problems, which is much lower than the 81.3% reported for female soccer players in college.17) This difference is not surprising because the young participants in the present study can be expected to have fewer sequelae of ankle sprain than college players given the differences in age and playing experience. In addressing Question 10 on specific ankle problems, 14% of participants in the current study experienced repeated sprains compared with approximately 23% of college players.17) This suggests that the participants will repeatedly sprain their ankles and develop CAI.
For participants with ankle problems, 14% of participants in this study rated their soccer performance as obviously impaired, which is a similar rating to that of college players (18.7%).17) The frequency and number of participants who received medical care for the second and subsequent ankle sprains were lower than those for the first ankle sprain. Participants that repeatedly injured their ankles tended to disregard ankle sprains and did not seek appropriate treatment and care. Although taping was the most common form of care used by participants (50%) with ankle problems, it was used less commonly than the use of taping by college players (73.9%).17) Many participants did not receive any care for their sprained ankle, which may suggest that younger players have little knowledge of self-care related to ankle sprains.
The current findings support the previous notions29) that many soccer players injure their ankles more than once and ankle sprain is often disregarded as just a sprain. This study also indicates the necessity of educating players to promote preventive intervention for ankle sprains among younger players and to increase their awareness of methods to properly treat and care for ankle sprains.
There are some limitations to this study. First, although the study analyzed the number of first ankle sprains by school grade level, it is important to note that the age distribution of the participants in the study may have been biased. Therefore, participants who had not experienced an ankle sprain at the time of the survey could still sustain ankle sprains beyond the age of 13 years. Second, although this is a cross-sectional study, the questions on ankle injury and menarche were retrospective. Therefore, this study is less reliable than prospective studies. Third, this study did not consider amenorrhea or abnormal menstrual cycles after menarche. Hypothalamic amenorrhea in the female athlete triad is commonly perceived as a concern, primarily among elite athletes. Łuszczki et al.30) investigated the risk of the female athlete triad in female soccer players aged 13–18 years at a sports school and estimated that 64.3% were at risk of developing this condition. Nose-Ogura et al.31) suggested that menstrual cycle abnormalities, including amenorrhea, should be considered at all levels of athletic competition. In addition, the female athlete triad can affect physical and mental development and increase the susceptibility of the athletes to sports injuries. Future studies must consider not only physical development but also secondary sexual characteristics specific to female athletes.
This study investigated the factors influencing ankle sprain injuries experienced by adolescent female soccer players. Most of the study participants (female junior players) experienced their first ankle sprain at the age of 10, 11, 12, or 13 years, which typically was the age of menarche or 1 year before or after menarche. Our findings suggest that preventive education and intervention for ankle sprains is required for junior female soccer players before the age of 10 years. Secondary prevention of ankle sprains should be initiated in this age group by providing proper knowledge, treatment, and care for the treatment of ankle sprains.
The authors thank all participants and all assistants in this study.
The authors declare no conflict of interest.