ABSTRACT
Objectives: Poor adherence to home exercise programs (HEPs) is a significant barrier to continuity of care and eventual outcomes, thus requiring innovative mitigating approaches. This study aimed to develop and test the feasibility of a remote support application (RSA) designed to encourage adherence to HEPs.
Methods: Using standard computer programing, an RSA with administrator and user interfaces was developed for mobile phone or tablet. Consenting patients receiving physiotherapy for musculoskeletal conditions (n=19) were randomly assigned into the experimental group (n=10) or the control group (n=9). The experimental group received their customized HEP reminders via the RSA, whereas the control group used conventional paper handouts for HEPs. Adherence to HEPs was assessed over 4 weeks. The feasibility of the RSA was assessed using the Mobile Application Rating Scale and System Usability Scale (SUS) questionnaires. Data were summarized using descriptive and inferential statistics.
Results: The adherence rate of patients in experimental group was significantly higher than that of patients in the control group after 2 weeks [median diff.=−6.0, 95% confidence interval (CI): −8.0 to −5.0; U=5.00; Z=−3.304; P=0.001; r=0.75] and 4 weeks (median diff.=−7.0, 95% CI: −8.0 to −5.0; U=0; Z=−3.695; P<0.001; r=0.84) of intervention. The RSA had a mean SUS score of 82.53±9.04 (out of 100) and a mean app quality rating score of 75.95±4.98 (out of 95).
Conclusions: The use of an RSA to improve adherence to HEPs is feasible for patients with musculoskeletal conditions.
INTRODUCTION
Interventions in rehabilitation practice are traditionally structured to be delivered in-person to the patient.1) However, the benefits of interventions are largely dependent on sustained patient participation, which has seen the emergence of home exercise programs (HEPs).2) Like face-to-face rehabilitation interventions, HEPs are typically long-term interventions.3) Therefore, adherence to HEPs is important if they are to achieve effective rehabilitation outcomes.4) Meichenbaum and Turk5) defined adherence as “an active voluntary collaborative involvement of the patient in a mutually acceptable behavior to produce a desired preventive and therapeutic result.” Adherence to HEPs is a major predictor of improved rehabilitation outcomes for patients with musculoskeletal problems.6,7,8,9) Unfortunately, despite the proven benefits of HEPs, the rates of non-adherence to HEPs are high. Literature reports have indicated rates of non-adherence to HEPs as high as 70%, together with high costs of care, detrimental impacts on treatment outcomes, reduced overall effectiveness in the health system, and promotion of negative relationships between patients and clinical staff.9,10,11) Researchers have simplified the factors associated with HEP adherence to include self-efficacy, outcome expectations, and environmental and personal factors.4,9,12,13,14,15,16,17)
Recognizing the detrimental effects and drawbacks of these multifaceted problems of HEP adherence, several attempts are being made globally to abate the issue. Earlier approaches have involved health education and orientation of patients about the benefits of HEPs18) and exercise prescription notes,19) among several others. However, the use of technology in aiding adherence to HEPs has been suggested in the literature.20) Recent use of software tools and aids has shown significant improvement in HEP adherence.19,21) Remote monitoring is a recent innovation that is considered to have the potential to improve adherence while also providing feedback.19,20) In recent times, applications with a remote monitoring function were utilized to enhance adherence among patients with hemophilia20) and musculoskeletal dysfunction.19) However, there remains limited information on the feasibility and effectiveness of these remote applications in improving adherence to HEPs. According to Lambert et al.19) more studies are needed to establish the clinical importance and benefits of HEP applications with remote support among people with musculoskeletal conditions by using freely available online software or other comparable technology towards improving adherence to HEPs. This study aimed to develop and test the feasibility of a remote support application (RSA) for improving HEP adherence.
MATERIALS AND METHODS
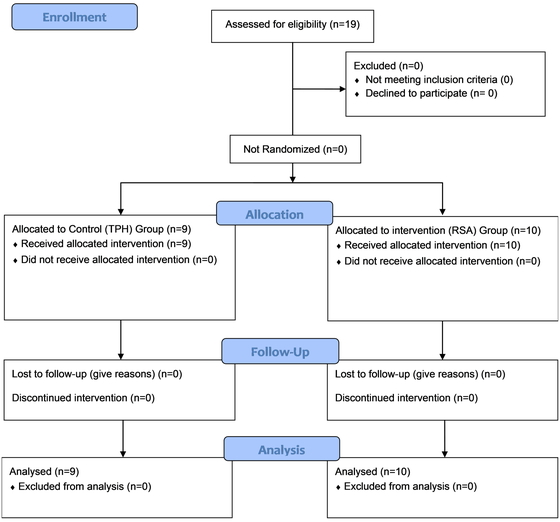
ParticipantsParticipants for this experimental study were patients receiving physiotherapy for musculoskeletal conditions at the Physiotherapy Department of Obafemi Awolowo University Teaching Hospital Complex (OAUTHC), Ile-Ife, Nigeria. The following inclusion criteria were used: a musculoskeletal dysfunction (MSD), aged 18 years or older, and use of a physiotherapist-prescribed HEP. Patients with cognitive impairment were excluded. By using the stepped rules of thumb for a pilot study, with a standardized difference d≥0.7 and expected 80% power for the main trial, ten samples were needed for each group.22) In total, 19 patients met the inclusion criteria and were recruited into either the experimental group (n=10) or the control group (n=9) based on simple consecutive assignment. As the patients became available and consented to participate in the study, they were enrolled in the study register. Patients with odd serial numbers on the register were assigned to the experimental group, whereas those with even serial numbers were assigned to the control group. The decision to assign odd (heads) or even (tails) numbers to the experimental or control group was based on a coin flip carried out by one of the research team. The assessors and therapists were not blinded to the patients who enrolled in this study. The study was carried out between 21 June and 10 September 2021. The CONSORT flow diagram of participant selection is shown in Fig. 1.
Each patient assigned to the experimental group used a mobile phone or tablet device (Android® operating system) loaded with the RSA developed for this study. The Android® operating system was selected because it was the most commonly used operating system in the study setting. Patients in the control group used a diary to record their adherence to the HEP.
The RSA was assessed using the System Usability Scale (SUS) and the Mobile App Rating Scale (MARS). The SUS questionnaire assessed each user’s experience in terms of engagement, satisfaction, level of motivation, and perceived complexity of the RSA. The interpretation of user experience was based on ISO 9241–210 (Ergonomics of human–system interaction), which defines a user’s experience as “a person’s perceptions and responses that result from the use or anticipated use of a product, system, or service.” The SUS questionnaire presents ten statements about the perceived usability of the mobile application. Participants rate on a scale of 0–4 to indicate the extent to which they agree with the statement.23) The MARS questionnaire was used to assess application quality, esthetics, engagement, functionality, and the user’s experience. This questionnaire is recognized as a reliable multidimensional scale for classifying and rating the information quality of mobile applications.24)
ProcedureBefore commencing this study, approval was obtained from the Ethics and Research Committee (ERC) of the Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria (Protocol number: ERC/2021/06/27). This study was conducted in accordance with the CONSORT statement25) and was retrospectively registered on the Pan African Clinical Trial Registry (PACTR202310710523197). Written informed consent was obtained from all participants. Using standard computer programing, an RSA for a HEP was developed for mobile phone or tablet. The application allowed for individualized exercises/activities to be created for the patient and included reminders to carry out the exercises/activities, in addition to tracking the patient’s adherence. The RSA had dual interfaces for administration and user interaction. The administrator interface allowed users to be added to the database and allowed the administrator (researcher) to register, monitor progress, and interact with users by sending them data in form of exercises, descriptive clips, texts, and notifications (Fig. 2). The user interface allowed the user to access individualized data sent by the administrator. It also allowed the user to set automatic reminders for exercise sessions (with consideration of the patient’s daily routine) and to view progress (Fig. 3).

The mobile interface was set based on the patient’s characteristics, preferences, and clinical profile. Interfaces were based on a simple design to ensure that inexperienced or less skilled users of technology would find the application easy to use with only basic educational experience or qualifications.
The development of the RSA occurred in two stages. The first stage considered the design of the user experience/user interface (UX/UI) for the administrator and the user. The interface designs were developed by a product designer. These interfaces were then constructed on the Android® operating system by a product developer. Full disclosure of the purpose and procedure of the research was given to all consenting participants prior to the study. The RSA developed and used in this study is for research purposes only and does not have any financial or commercial interest. It is available from the authors on request.
All participants were assigned to either the experimental (RSA) group (n=10) or the control group (n=9). The experimental group received customized HEP reminders via the RSA, whereas the control group used conventional paper handouts for HEPs provided to them by the supervising physiotherapist. The participants in the control group were advised to keep a daily record of their adherence to the recommended HEPs in a dairy. They did not receive any encouragement nor were asked to provide feedback until their 2-week follow-up assessment when diaries were assessed.
All participants in the experimental group used mobile phones that ran the Android® operating system (version 8.0 or above). After individualized HEPs were configured on the RSA installed on the mobile devices, participants were instructed on how to navigate through the application. Participants were instructed to use the application for 4 weeks, and those who required further clarification on use of the application were allowed to call for assistance. Participants were advised to complete their HEPs as recommended by the supervising physiotherapist. Each time the RSA was opened or used by the patients, the researcher received notifications and could log patient activities. However, participants were assured of their privacy and safety and that none of their personal information would be remotely accessed. Adherence to HEPs through RSA use was assessed after the second and fourth weeks of the study. All participants using the RSA completed the SUS and MARS questionnaires. Because self-administration was used in this study, the participants required a basic standard of literacy.
Data AnalysisData were summarized using the descriptive statistics of mean, standard deviation, median, interquartile range (IQR), frequency, range, and percentage. The chi-square test and Mann–Whitney U test were used to investigate differences in gender and age between the groups. The inferential statistics of the Mann–Whitney U test were used to compare effects between groups. The alpha level was set at P<0.05. Data analysis was carried out using SPSS version 28 (IBM, Armonk, NY, USA).
RESULTS
In this study, 52.6% of the participants were male and 47.4% were female. Most participants (73.7%) were aged 43–65 years with the remainder (26.3%) aged 18–42 years. The mean age of the participants was 48.4±13.5 years. Each group included five men. The mean age of the participants was 47.5±13.5 years in the experimental group and 49.5±13.6 years in the control group. There was no significant difference between the groups in terms of age or gender (P>0.05). Clinical characteristics of the patients are presented in Table 1. The most commonly affected sites among the participants were the lower limbs (42.1%), whereas the neck regions (5.3%) showed the lowest involvement. The most common type of injury was post-immobilization stiffness secondary to fracture (31.6%). The prescribed home programs were varied and used 13 different exercises amongst the 19 patients. The more commonly used exercises included grip strengthening exercises (15.8%), supine heel slides (15.8%), prone press-ups on elbows (10.5%), and supine triceps extension (10.5%).
Table 1. Clinical characteristics of participants
| Characteristic | Control group (n=9) | Experimental group (n=10) | Total (n=19) |
| Affected area | | | |
| Neck | 0 (0) | 1 (10.0) | 1 (5.3) |
| Upper limb | 4 (44.4) | 3 (30.0) | 7 (36.8) |
| Lower limb | 2 (22.2) | 6 (60.0) | 8 (42.1) |
| Lower back | 3 (33.3) | 0 (0) | 3 (15.8) |
| Injury/condition type | | | |
| Bilateral knee OA | 0 (0) | 1 (10.0) | 1 (5.3) |
| Frozen shoulder | 1 (11.1) | 0 (0) | 1 (5.3) |
| Low-back pain | 3 (33.3) | 0 (0) | 3 (15.8) |
| Neck pain | 0 (0) | 1 (10.0) | 1 (5.3) |
| PIMSF | 3 (33.3) | 3 (30.0) | 6 (31.6) |
| Piriformis syndrome | 0 (0) | 1 (10.0) | 1 (5.3) |
| Round shoulder | 1 (11.1) | 0 (0) | 1 (5.3) |
| Unilateral knee OA | 2 (22.2) | 3 (30.0) | 5 (26.3) |
| Exercise | | | |
| Ankle pump exercise | 1 (11.1) | 0 (0) | 1 (5.3) |
| Bridging exercise | 1 (11.1) | 0 (0) | 1 (5.3) |
| Doorway pectoralis stretch | 1 (11.1) | 0 (0) | 1 (5.3) |
| Grip strengthening exercise | 2 (22.2) | 1 (10.0) | 3 (15.8) |
| Lateral neck flexion stretch | 0 (0) | 1 (10.0) | 1 (5.3) |
| Piriformis stretch | 0 (0) | 1 (10.0) | 1 (5.3) |
| Prone press-ups on elbows | 2 (22.2) | 0 (0) | 2 (10.5) |
| Seated knee flexion and extension | 0 (0) | 1 (10.0) | 1 (5.3) |
| Shoulder wall-climb stretch | 1 (11.1) | 0 (0) | 1 (5.3) |
| Squatting with support | 0 (0) | 1 (10.0) | 1 (5.3) |
| Supine hamstring stretch | 1 (11.1) | 0 (0) | 1 (5.3) |
| Supine heel slides | 0 (0) | 3 (30.0) | 3 (15.8) |
| Supine triceps extension | 0 (0) | 2 (20.0) | 2 (10.5) |
Data presented as number (percentage).
OA, osteoarthritis; PIMSF, post-immobilization stiffness secondary to fracture.
The mean scores from the SUS and MARS questionnaires are presented in Table 2. The mean total usability rating score (from SUS) was 82.5±9.04 (out of 100). The mean score for the total app quality rating (from MARS) was 76.0±4.98 (out of 95). The mean score for the subjective app quality rating (from MARS) was 16.6±2.43. The scores for engagement (19.6±1.07), functionality (16.1±1.56), and information (28.1±3.12) were relatively high. The mean scores for the perceived impacts of the RSA on the knowledge, attitudes, intentions, and behavior change in relation to the importance of adherence to HEPs are presented in Table 3. The total mean score was 24.5±2.41 (out of 30). The results showed that use of the RSA primarily led to increased levels of awareness and increases in other parameters. After 2 weeks, the median (IQR) adherence to HEPs was 10.0 (4.5) sets (out of 28 sets) for the control group (paper handouts) and 15.5 (3.0) sets for the experimental group (RSA). After 4 weeks, the median (IQR) adherence to HEPs was 14.0 (3.5) sets for the control group and 20.5 (1.5) sets for the experimental group. The adherence rate after 2 weeks was significantly higher for the experimental group [median diff.=−6.0, 95% confidence interval (CI): −8.0 to −5.0; U=5.00; Z=−3.304; P= 0.001; r=0.75]. After 4 weeks, the participants in the experimental group showed a significant increase in adherence to HEPs when compared with the control group (median diff.=−7.0, 95% CI: −8.0 to −5.0; U=0; Z=−3.695; P<0.001; r=0.84).
Table 2. App quality rating and system usability scores for the RSA (n=10)
| Rating | Participant score | Range |
| Minimum | Maximum |
| App quality scrs | | | |
| Engagement | 19.6±1.07 | 18 | 23 |
| Functionality | 16.1±1.56 | 14 | 19 |
| Esthetics | 12.2±1.65 | 7 | 14 |
| Information | 28.1±3.12 | 22 | 34 |
| App quality mean score | 76.0±4.98 | 69 | 87 |
| Subjective quality rating | | | |
| App subjective quality score | 16.6±2.43 | 12 | 20 |
| App usability score of RSA | | | |
| Total app usability score | 82.5±9.04 | 66 | 92 |
Participant scores given as mean±standard deviation. App quality scores and subjective quality score from MARS questionnaire; total app usability score from SUS questionnaire.
Table 3. Mean scores for perceived impact of the RSA on user knowledge, attitude, intentions, and behavior change in relation to the importance of adherence to HEPs (n=10)
| App effect | Score | Minimum | Maximum |
| Awareness | 4.32±0.58 | 3 | 5 |
| Knowledge | 3.84±0.89 | 3 | 5 |
| Attitude | 4.00±0.75 | 3 | 5 |
| Intention to change | 4.21±0.71 | 3 | 5 |
| Help seeking | 4.16±0.90 | 3 | 5 |
| Behavior change | 3.95±0.91 | 2 | 5 |
| Total mean score | 24.5±2.41 | 21 | 29 |
Scores given as mean±standard deviation.
DISCUSSION
Despite the rapid uptake of digital applications within the health community, there has been little attempt at providing and validating an RSA to promote adherence to HEPs in the field of physiotherapy. The aim of this study was to develop and test the feasibility of an RSA for HEP adherence, as well as to assess the usability of the application among users. The results showed that adherence to recommended HEPs for patients using the RSA was higher than the adherence shown by patients using the conventional approach. There are limited studies on the use of RSAs to improve adherence to HEPs among patients with MSDs; however, their benefits have been reported in other studies.19,20) The results of the current study confirm the earlier reports. Beyond the method employed by Lambert et al.,19) where self-reported adherence was used to determine the effect of online software for HEP adherence, the RSA used in the current study calculated the patient’s adherence, which could be monitored through the administrator dashboard of the application. This new approach helps to minimize the chances of poor completion rates, inaccurate recall, and self-presentation bias, which are factors already noted by other investigators.26) Furthermore, the RSA utilized in this study was designed to allow for individualized HEPs that could be monitored remotely by triggering an alert when the patient starts and completes a HEP session. These features help the monitoring of HEPs and are valuable for providing feedback to patients.
The findings of this study showed that the RSA for adherence to HEPs had high scores for usability, quality, and ability to change health behavior. In addition, there was a significant increment in adherence to HEPs through use of the RSA. It can be inferred that the RSA is a credible and reliable tool to improve patient adherence to HEPs. In the present study, the participants gave a high rating for the quality of the RSA, especially in the areas of engagement, functionality, and information. These features have been reported to be important in the uptake and continued use of health-related apps.27) A report released by a software company claimed that only 8% of users continued to use medical and fitness apps 7 days after installation because of a lack of or poor engagement and functionality features (see https://www.braze.com/blog/app-customer-retention-spring-2016-report). Another study reported that most patients only use medical apps a few times after initial exposure.28) In the present study, no participant in the experimental group was lost to follow-up and none discontinued the intervention during the 4 weeks of the study. Furthermore, the adherence rate among this group increased from the 2-week assessment to the 4-week assessment, suggesting that the application was easy to use with good functionality. Other factors that have been mentioned in the literature as being responsible for poor continued use of medical apps include a lack of interactive, feedback, and self-monitoring features.29) The RSA in the present study had these features and may be responsible for the high ratings of patients.
This study has some limitations. First, the generalizability of the findings of this study is limited to patients with MSDs and those with basic literacy. Second, the lack of blinding to the participants in this study may be a source of performance and detection bias. This may have affected the internal validity of the findings through possible underestimation or overestimation of the intervention effect. Nonetheless, considering the pilot nature of this study, the findings will serve as preliminary data for a full-size randomized clinical trial. In this study, the RSA attributes of satisfaction, usability, acceptance, and quality were assessed using MARS and SUS questionnaires, in addition to adherence, which is an associated clinical outcome. The findings showed that use of the RSA enhanced the adherence to HEPs when compared with conventional methods using paper handouts. However, further studies should be carried out to ascertain the long-term effectiveness of RSAs.
CONCLUSION
This study examined the feasibility of using an RSA to encourage adherence to HEPs by comparison with the conventional method of using paper handouts. The use of RSAs is feasible for the improvement of patient engagement and to improve adherence to HEPs among patients with musculoskeletal dysfunctions.
ACKNOWLEDGMENTS
The authors thank the study participants for their assistance.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Spetch LA, Kolt GS: Adherence to sport injury rehabilitation: implications for sports medicine providers and researchers. Phys Ther Sport 2001;2:80–90. DOI:10.1054/ptsp.2001.0062
- 2. Picorelli AM, Pereira LS, Pereira DS, Felício D, Sherrington C: Adherence to exercise programs for older people is influenced by program characteristics and personal factors: a systematic review. J Physiother 2014;60:151–156. PMID:25092418, DOI:10.1016/j.jphys.2014.06.012
- 3. Kisner C, Colby LA, Borstad J: Therapeutic exercise: foundations and techniques. F.A. Davis, Philadelphia, 2017.
- 4. Okezue OC, Nwafor GC, Ezeukwu OA, John JN, Uchenwoke CI: Adherence to home exercise programmes and its associated factors among patients receiving physiotherapy. Clin Health Promot 2019;9:7–14. DOI:10.29102/clinhp.19003
- 5. Meichenbaum D, Turk DC: Facilitating treatment adherence: a practitioner’s guidebook. Plenum Press, New York, 1987.
- 6. Bassett SF: The assessment of patient adherence to physiotherapy rehabilitation. NZ J Physiother 2003;31:60–66.
- 7. Holden MA, Haywood KL, Potia TA, Gee M, McLean S: Recommendations for exercise adherence measures in musculoskeletal settings: a systematic review and consensus meeting (protocol). Syst Rev 2014;3:10. PMID:24512976, DOI:10.1186/2046-4053-3-10
- 8. Pisters MF, Veenhof C, Schellevis FG, Twisk JW, Dekker J, De Bakker DH: Exercise adherence improving long‐term patient outcome in patients with osteoarthritis of the hip and/or knee. Arthritis Care Res (Hoboken) 2010;62:1087–1094. PMID:20235201, DOI:10.1002/acr.20182
- 9. Sluijs EM, Kok GJ, van der Zee J: Correlates of exercise compliance in physical therapy. Phys Ther 1993;73:771–786. PMID:8234458, DOI:10.1093/ptj/73.11.771
- 10. O’Carroll R, Dennis M, Johnston M, Sudlow C: Improving adherence to medication in stroke survivors (IAMSS): a randomised controlled trial: study protocol. BMC Neurol 2010;10:15. PMID:20181255, DOI:10.1186/1471-2377-10-15
- 11. Paterson BL, Charlton P, Richard S: Non‐attendance in chronic disease clinics: a matter of non‐compliance? J Nurs Healthc Chronic Illn 2010;2:63–74. DOI:10.1111/j.1752-9824.2010.01048.x
- 12. Forkan R, Pumper B, Smyth N, Wirkkala H, Ciol MA, Shumway-Cook A: Exercise adherence following physical therapy intervention in older adults with impaired balance. Phys Ther 2006;86:401–410. PMID:16506876, DOI:10.1093/ptj/86.3.401
- 13. Burton LC, Shapiro S, German PS: Determinants of physical activity initiation and maintenance among community-dwelling older persons. Prev Med 1999;29:422–430. PMID:10564634, DOI:10.1006/pmed.1999.0561
- 14. Conn VS: Older adults and exercise: path analysis of self-efficacy related constructs. Nurs Res 1998;47:180–189. PMID:9610652, DOI:10.1097/00006199-199805000-00009
- 15. Resnick B: Testing a model of exercise behavior in older adults. Res Nurs Health 2001;24:83–92. PMID:11353456, DOI:10.1002/nur.1011
- 16. Jack K, McLean SM, Moffett JK, Gardiner E: Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man Ther 2010;15:220–228. PMID:20163979, DOI:10.1016/j.math.2009.12.004
- 17. Palazzo C, Klinger E, Dorner V, Kadri A, Thierry O, Boumenir Y, Martin W, Poiraudeau S, Ville I: Barriers to home-based exercise program adherence with chronic low back pain: patient expectations regarding new technologies. Ann Phys Rehabil Med 2016;59:107–113. PMID:27050664, DOI:10.1016/j.rehab.2016.01.009
- 18. Argent R, Daly A, Caulfield B: Patient involvement with home-based exercise programs: can connected health interventions influence adherence? JMIR Mhealth Uhealth 2018;6:e47. PMID:29496655, DOI:10.2196/mhealth.8518
- 19. Lambert TE, Harvey LA, Avdalis C, Chen LW, Jeyalingam S, Pratt CA, Tatum HJ, Bowden JL, Lucas BR: An app with remote support achieves better adherence to home exercise programs than paper handouts in people with musculoskeletal conditions: a randomised trial. J Physiother 2017;63:161–167. PMID:28662834, DOI:10.1016/j.jphys.2017.05.015
- 20. Goto M, Takedani H, Haga N, Kubota M, Ishiyama M, Ito S, Nitta O: Self‐monitoring has potential for home exercise programmes in patients with haemophilia. Haemophilia 2014;20:e121–e127. PMID:24418413, DOI:10.1111/hae.12355
- 21. Mbada CE, Lateef MA, Ademoyegun AB, Oyewole AI, Maikudi L, Fatoye C, Fatoye F: Effect of WhatsApp-based reminders on adherence to home exercise program. Int J Telemed Clin Pract 2022;3:341–350.
- 22. Bell ML, Whitehead AL, Julious SA: Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin Epidemiol 2018;10:153–157. PMID:29403314, DOI:10.2147/CLEP.S146397
- 23. Brooke J: SUS—a quick and dirty usability scale. In: Jordan PW, Thomas B, Weerdmeester BA, McClelland IL, editors. Usability evaluation in industry. CRC Press, London; 1996. pp. 189–194.
- 24. Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M: Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 2015;3:e27. PMID:25760773, DOI:10.2196/mhealth.3422
- 25. Schulz KF, Altman DG, Moher D, CONSORT Group: CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med 2010;7:e1000251. PMID:20352064, DOI:10.1371/journal.pmed.1000251
- 26. Beinart NA, Goodchild CE, Weinman JA, Ayis S, Godfrey EL: Individual and intervention-related factors associated with adherence to home exercise in chronic low back pain: a systematic review. Spine J 2013;13:1940–1950. PMID:24169445, DOI:10.1016/j.spinee.2013.08.027
- 27. Van Baelen F, De Regge M, Larivière B, Verleye K, Schelfout S, Eeckloo K: Role of social and app-related factors in behavioral engagement with mHealth for improved well-being among chronically ill patients: scenario-based survey study. JMIR Mhealth Uhealth 2022;10:e33772. PMID:36018618, DOI:10.2196/33772
- 28. Vaghefi I, Tulu B: The continued use of mobile health apps: insights from a longitudinal study. JMIR Mhealth Uhealth 2019;7:e12983. PMID:31469081, DOI:10.2196/12983
- 29. Perski O, Blandford A, West R, Michie S: Conceptualising engagement with digital behaviour change interventions: a systematic review using principles from critical interpretive synthesis. Transl Behav Med 2017;7:254–267. PMID:27966189, DOI:10.1007/s13142-016-0453-1
