ABSTRACT
Objectives: The purpose of this study was to examine the association
between baseline dysphagia and the improvement of activities of daily living
performance and cognitive level among inpatients after stroke.
Methods: This was a retrospective cohort study of patients
undergoing convalescent rehabilitation after stroke. Dysphagia was assessed
using the Food Intake LEVEL Scale. Outcomes were the motor and cognitive scores
of the Functional Independence Measure (FIM) at discharge. Multiple regression
analysis was performed to examine the association between dysphagia at admission
and these outcomes.
Results: There were 499 participants with a median age of 74 years.
A multiple regression analysis was carried out after adjusting for potential
confounders including age and sex. Dysphagia at admission was independently and
negatively associated with motor (β=−0.157, P<0.001) and cognitive (β=−0.066,
P=0.041) FIM scores at discharge.
Conclusions: Baseline dysphagia in patients after stroke was
negatively associated with improvement in performance of activities of daily
living and cognitive level.
INTRODUCTION
Dysphagia is known to be associated with dehydration,1) poor nutrition,2) cognitive
function,3)
sarcopenia, and physical decline,4,5) making it a significant problem. Stroke is
significantly related to the occurrence of aspiration pneumonia and accounts for
approximately 60% of dysphagia cases that develop into aspiration
pneumonia.6)
Furthermore, dysphagia after stroke has been observed in 29%–67% of patients in the
acute phase7) and
28%–59% of patients in convalescent wards.8,9)
Quality of life for patients after a stroke is directly associated with dysphagia and
activities of daily living (ADL).5) Dysphagia after a stroke is also associated with
increased length of hospital stay, pneumonia, decreased physical independence, high
mortality risk,10) poor
oral hygiene,11)
nutritional disorders,12) and a low rate of discharge to home.13) Furthermore, patients
are known to have reduced motor and cognitive functions following stroke, resulting
in a poorer quality of life.14) ADL and cognitive function after a stroke are
prognostic predictors of discharge destination,15) and it has been shown that low functional
independence at discharge is associated with mortality.16) Therefore, dysphagia, inability to
perform ADL, and cognitive decline after stroke are important issues to be addressed
in convalescent wards. Patients who present with dysphagia on admission after a
cerebrovascular accident may suffer deleterious effects on their ADL and cognitive
function at the time of discharge because of a variety of factors, including
compromised nutritional status, in contrast to patients who do not present with
dysphagia. Studies on acute care patients have reported that dysphagia at admission
is associated with motor and physical function at discharge.17)
Few studies have examined whether dysphagia at hospital admission in patients with a
stroke is associated with motor, physical, and cognitive functions at discharge.
Therefore, the purpose of this study was to determine the association between the
presence of dysphagia at admission and ADL performance and cognitive function at
discharge in patients admitted to convalescent rehabilitation hospital following
stroke. Recognizing that dysphagia on admission correlates with motor and cognitive
functioning at the time of discharge can help healthcare professionals improve
patient assessment and treatment protocols.
MATERIALS AND METHODS
Patients and Settings
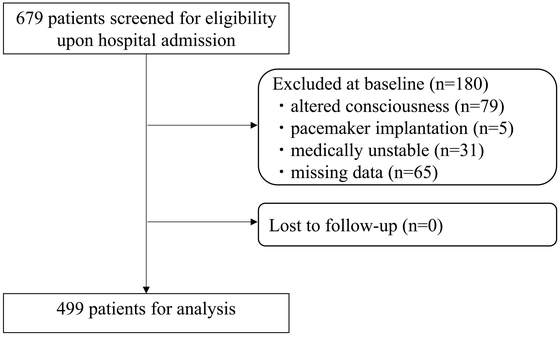
We conducted a retrospective cohort study of 679 patients consecutively admitted
to our post-stroke convalescent rehabilitation units from 2015 to 2020. Patients
with impaired consciousness as determined by a triple-digit Japan Coma Scale
score and those with medically unstable respiratory or circulatory status were
excluded because of the difficulty in providing adequate rehabilitation. In
addition, patients deemed unsuitable for bioimpedance analysis, such as those
with pacemaker implantation, were excluded because of challenges in assessing
muscle mass. Finally, a total of 499 patients were included in the analysis
(Fig. 1).
Data Collection
Basic patient information collected at admission included age, sex, stroke type,
Food Intake LEVEL Scale (FILS)18) at admission and discharge, the duration from
the onset of stroke, and length of hospital stay. The presence of sarcopenia was
diagnosed according to the criteria of the Asian Working Group for Sarcopenia
2019.19)
Specifically, muscle mass was assessed by bioelectrical impedance analysis,
muscle strength was assessed by grip strength, and sarcopenia was assessed if a
decline was observed. In addition, total daily convalescent units (1 unit=20
min) were calculated for therapy performed by physical therapists, occupational
therapists, and speech-language therapists (units/day). ADL performance was
assessed using the motor and cognitive domains of the Functional Independence
Measure (FIM),20)
nutritional status was assessed using the Geriatric Nutritional Risk Index
(GNRI),21)
pre-onset ADL performance was assessed using the modified Rankin Scale
(mRS),22)
and comorbidity severity was assessed using the Charlson Comorbidity Index
(CCI).23)
Dysphagia Assessment
Dysphagia was assessed on the day of admission using the FILS after a
speech-language pathologist observed the patient’s actual eating condition and
reported to a rehabilitation physician with over a decade of experience. The
FILS is an ordinal scale with ten levels of feeding status: 1–3 indicates no
oral intake, 4–6 indicates combined oral intake and alternative nutrition, 7–9
indicates oral intake only, and 10 is considered normal.18) Participants with
a FILS score of less than 7 at admission were placed in the group for oral
intake with supportive nutrition (SN group), whereas participants with a FILS
score of 7 or more were placed in the group for oral intake without supportive
nutrition (ON group).
Outcomes
The primary outcome was the motor FIM score at discharge, and the secondary
outcome was cognitive FIM score at discharge. The FIM consists of a motor domain
with 13 sub-items and a cognitive domain with 5 sub-items. Each sub-item is
rated on a seven-point ordinal scale ranging from full caregiving to full
independence. Scores range from 18 to 126 for the FIM overall, from 13 to 91 for
motor FIM, and from 5 to 35 for cognitive FIM. Lower scores indicate lower
levels of patient independence.
Convalescent Rehabilitation
The convalescent rehabilitation program was tailored to each patient’s function
and weaknesses (up to 3 h/day).24) The program was implemented in collaboration
with multiple specialists including physiatrists, physical therapists,
occupational therapists, speech-language therapists, nurses, pharmacists, dental
staff, and registered dietitians. Patients admitted to the convalescent
rehabilitation hospital were divided into three categories according to their
disease etiology: stroke, musculoskeletal disorders, and hospital-associated
deconditioning. All patients with stroke were transferred from the stroke care
unit of acute care hospitals in the local medical cooperation system.
Physical and occupational therapy included facilitation of paralyzed limbs, range
of motion training, basic movement training, gait training, resistance training
(e.g., chair-stand exercise),24,25) and ADL training.26) Therapy was administered according
to each patient’s functional abilities and weaknesses.
Nutritional management consisted of nutrition screening and assessment for
eligible patients. Active nutritional support, such as high-energy and
high-protein diets, was also implemented. Nutritional management was also
tailored to each patient’s condition and nutritional needs, including the
adjustment of energy and protein contents according to changes in rehabilitation
time and load.27)
Rehabilitation for dysphagia included oral management and indirect and direct
swallowing training with collaboration between speech-language pathologists,
dental hygienists, and ward nurses. Rehabilitation was conducted according to
each patient’s swallowing ability and function.28,29)
Medication management was handled by a multidisciplinary team that included a
pharmacist. Measures were taken to reduce or discontinue polypharmacy and
potentially inappropriate medications (PIMs), as well as to adjust or taper
medications that affect swallowing and cognitive levels.30,31)
Sample Size Calculation
The sample size was calculated using data from our previous study,32) the results of
which showed that the motor FIM score of patients admitted to the hospital was
normally distributed with a standard deviation of 26. For a true difference in
means between those with and without dysphagia of 17,33) a sample size of at least 65
participants was needed in each group to reject the null hypothesis with a power
of 0.8 and an alpha error of 0.05, which would support the validity of our
results.
Statistical Analysis
The eligible patients were classified into two groups according to the presence
or absence of supplementary nutrition, and basic information and outcomes were
compared between the groups. Statistical analysis was performed using the
unpaired t-test, the Mann–Whitney U test, and the chi-square
test according to variables and normality. To assess the association between
dysphagia on admission and outcome, clinically important confounding factors for
outcome were considered and adjustment variables were selected. Confounders
included age, sex, sarcopenia status, motor and cognitive FIM scores on
admission, daily convalescent ward attendance, GNRI, length of hospital stay,
CCI, and pre-admission mRS. The dependent variables were the motor and cognitive
FIM scores at discharge. SPSS version 21 (IBM, Armonk, NY, USA) was used for
statistical analysis, and P<0.05 was considered to indicate statistical
significance.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was
approved in advance by the Ethics Review Committee of Kumamoto Rehabilitation
Hospital (Approval No. 179–211117). In addition, the study protocol was
disclosed on the hospital website, and an opt-out method was used to present
patients with the opportunity to refuse participation.
RESULTS
The study population consisted of 499 patients with a median age of 74.0 years
[interquartile range (IQR), 63.0–82.0 years]. Of the 499 patients, 269 (53.9%) were
male. The median FILS score was 8 (IQR, 7–10), and 104 (20.8%) patients had a FILS
score less than 7. The results of univariate analysis between the two groups
according to basic patient information at admission and the presence or absence of
supplemental nutrition are summarized in Table
1. The SN group had a higher prevalence of sarcopenia, lower motor and
cognitive FIM scores at admission, lower GNRI scores, longer hospital stays, and
higher CCI scores than the ON group.
Table 1. Comparison between patient groups by patient background and with or
without supportive nutrition on admission
|
Total
n=499 |
SN group
n=104 |
ON group
n=395 |
P value |
| FILS at admission |
8 (7–10) |
2 (2–2) |
10 (7–10) |
<0.001 |
| Age (years) |
74 (63–82) |
74.5 (63–83) |
73 (63–81) |
0.460b |
| Sex |
|
|
|
0.509c |
| Male |
269 (53.9%) |
53 (50.9%) |
216 (54.6%) |
| Female |
230 (46.1%) |
51 (49.0%) |
179 (45.3%) |
| Stroke type |
|
|
|
<0.001c |
| Cerebral infarction |
313 (62.7%) |
49 (47.1%) |
264 (66.8%) |
| Cerebral hemorrhage |
146 (29.2%) |
48 (46.1%) |
98 (24.8%) |
| Subarachnoid hemorrhage |
40 (8.0%) |
7 (6.7%) |
33 (8.3%) |
| Sarcopenia |
|
|
|
<0.001c |
| Yes |
216 (43.3%) |
71 (68.2%) |
145 (36.7%) |
| No |
283 (56.7%) |
33 (31.7%) |
250 (63.2%) |
| Motor FIM at admission |
47 (20–69) |
13 (13–15) |
57 (34–73) |
<0.001b |
| Cognitive FIM at admission |
22 (14–28) |
8 (6–15) |
24 (17–30) |
<0.001b |
| Rehabilitation units per day |
8.2 (7.7–8.5) |
8.2 (7.2–8.5) |
8.2 (7.7–8.5) |
0.443b |
| Time from onset to hospital admission
(days) |
14 (10–22) |
17 (12–25) |
13 (10–21) |
<0.005b |
| GNRI |
96.8 (88.7–105.3) |
88.8 (81.0–96.3) |
99.2 (91.1–106.0) |
<0.001 |
| CCI |
3 (1–4) |
3 (2.2–4) |
3 (1–3) |
<0.001b |
| Premorbid mRS |
0 (0–1) |
0 (0–2) |
0 (0–1) |
0.376b |
Data given as number (percentage) or median (interquartile range).
at-test; b Mann–Whitney U test;
c chi-square test.
A comparison of the motor and cognitive FIM scores at discharge between the two
groups with and without supplemental nutrition is presented in Table 2. The SN group had significantly lower motor
(P<0.001) and cognitive (P<0.001) FIM scores at discharge.
Table 2. Comparison of outcomes and patient characteristics between patient
groups with and without supportive nutrition on admission
|
Total
n=499 |
SN group
n=104 |
ON group
n=395 |
P valuea |
| FILS at discharge |
10 (9–10) |
8 (4.2–9) |
10 (9–10) |
<0.001 |
| Length of hospital stay (days) |
91 (53–142) |
142 (107–158) |
81 (47–122) |
<0.001 |
| Rehabilitation units per day |
8.2 (7.7–8.5) |
8.2 (7.2–8.5) |
8.2 (7.7–8.5) |
0.443 |
| Motor FIM at discharge |
82 (56–89) |
46 (17.2–74.5) |
85 (74–90) |
<0.001 |
| Cognitive FIM at discharge |
30 (22–34) |
18.5 (10–29.7) |
31 (25–34) |
<0.001 |
Data given as median (interquartile range).
a Mann–Whitney U test.
The results of multiple regression analysis for motor and cognitive FIM scores at
discharge are presented in Table 3.
Because the variance inflation factor of all variables was less than 3.560, we
considered all of them acceptable as independent factors in the multiple regression
analysis. Dysphagia was independently associated with motor (β=−0.157, P<0.001)
and cognitive (β=−0.066, P=0.041) FIM scores at discharge.
Table 3. Multivariate analysis with motor FIM at discharge and cognitive FIM at
discharge as dependent variables
|
Multiple regression analysis:
forced entry method (n=499) |
| Motor FIM at discharge |
|
Cognitive FIM at
discharge |
| B (95% CI) |
SE |
β |
P value |
|
B (95% CI) |
SE |
β |
P value |
| Dysphagia (FILS<7) |
−9.588
(−13.603, −5.574) |
2.043 |
−0.157 |
<0.001 |
|
−1.365
(−2.676, −0.054) |
0.667 |
−0.066 |
0.041 |
| Age |
−0.052
(−0.175, 0.072) |
0.063 |
−0.027 |
0.412 |
|
−0.057
(−0.097, −0.016) |
0.021 |
−0.089 |
0.006 |
| Sex (female0, male1) |
0.976
(−1.720, 3.671) |
1.372 |
0.02 |
0.477 |
|
−0.398
(−1.279, 0.482) |
0.448 |
−0.024 |
0.375 |
| Sarcopenia (yes 1) |
−2.927
(−6.237, 0.384) |
1.685 |
−0.059 |
0.083 |
|
−0.533
(−1.615, 0.548) |
0.550 |
−0.031 |
0.333 |
Motor FIM at
admission |
0.450
(0.354, 0.546) |
0.049 |
0.463 |
<0.001 |
|
0.040
(0.008, 0.071) |
0.016 |
0.121 |
0.013 |
Cognitive FIM at
admission |
0.505
(0.289, 0.721) |
0.11 |
0.184 |
<0.001 |
|
0.592
(0.521, 0.663) |
0.036 |
0.636 |
<0.001 |
| Rehabilitation units/day |
−0.068
(−0.627, 0.491) |
0.285 |
−0.007 |
0.812 |
|
0.030
(−0.150, 0.215) |
0.093 |
0.009 |
0.726 |
| GNRI |
0.187
(0.058, 0.317) |
0.066 |
0.097 |
0.005 |
|
0.030 (−0.012, 0.072) |
0.021 |
0.045 |
0.164 |
| Hospital stay |
0.065
(0.028, 0.102) |
0.019 |
0.127 |
0.001 |
|
0.027
(0.015, 0.039) |
0.006 |
0.154 |
<0.001 |
| CCI |
−0.489
(−1.334, 0.356) |
0.43 |
−0.033 |
0.256 |
|
−0.109
(−0.385, 0.167) |
0.140 |
−0.022 |
0.437 |
| Premorbid mRS |
−3.003
(−4.185, −1.822) |
0.601 |
−0.153 |
<0.001 |
|
−0.880
(−1.266, −0.494) |
0.196 |
−0.132 |
<0.001 |
|
R2=0.65 |
|
R2=0.68 |
CI, confidence interval; SE, standard error.
DISCUSSION
We investigated whether dysphagia at the time of admission was associated with ADL
performance and cognitive level at the time of discharge in patients admitted to
convalescent rehabilitation hospital after stroke. Our results showed that dysphagia
at admission was negatively associated with ADL performance and cognitive level at
discharge.
In recovering stroke patients, dysphagia at admission was associated with lower ADL
performance and cognitive level at discharge. Other studies have shown that patients
with dysphagia at admission in the acute phase are likely to have a poorer prognosis
for motor function,17,34) and it has been indicated that patients who retain
motor and cognitive functions at admission tend to have a better prognosis for
dysphagia.35,36,37)
This study focused on patients with post-stroke dysphagia. Based on previous
research, it was hypothesized that improvements in dysphagia during rehabilitation
could contribute to improvements in ADL performance and cognitive level. Factors
associated with improvements in post-stroke motor and cognitive functions include
the severity of the stroke,38) stroke characteristics such as bilateral damage,
previous stroke, and lesion location,38,39) and the time from onset to hospital
admission.40)
Stroke severity has been shown to correlate with dysphagia,41) but there are also
reports of no association between stroke severity and dysphagia when compared with
another factor.42) The
results of this study suggest that dysphagia at admission is related to ADL and
cognitive levels at discharge. However, previous research indicates that factors
such as history of stroke, lesion type, damage site, and severity of stroke in the
SN and ON groups may also have had an impact. This is further supported by the fact
that the SN group had lower admission FIM scores than the ON group, suggesting a
possible association.
It has also been shown that decreases in muscle strength and muscle mass on the
nonparalyzed side occur in patients after stroke and contribute to their level of
physical function.43)
In addition, dysphagia caused by sarcopenia has recently received attention, and
cases of dysphagia have been reported in the absence of stroke or other central
nervous system diseases. In these cases, reduced muscle strength and mass were
contributing factors.44) The relationship between sarcopenia and dysphagia
is well recognized; cases are known in which dysphagia can lead to malnutrition and
systemic sarcopenia and vice versa where systemic sarcopenia can lead to
dysphagia.45)
In the current study, which focused on post-stroke patients with dysphagia, it was
difficult to attribute dysphagia solely to sarcopenia. However, patients with
dysphagia at admission had significantly lower motor FIM scores at admission and at
discharge, suggesting an association between dysphagia and motor function.
Regarding the prognosis of post-stroke dysphagia, factors such as the level of
consciousness,41) the severity of the stroke,46) and specific stroke
characteristics (including brainstem lesions, bilateral damage, history of stroke,
and stroke location)41,46) have been identified. Reports on the relationship
between stroke type and dysphagia are conflicting, with one study finding an
association and others not.47,48,49,50) In the present study, the SN group had
significantly lower cognitive FIM scores at both admission and discharge, in
addition to higher dysphagia severity, when compared with the ON group. These
observations suggest that variations in consciousness and specific characteristics
of cerebrovascular events may have contributed to these results. The pathophysiology
of dysphagia following a stroke is multifaceted, involving both motor output issues,
such as tongue movement and chewing strength, and sensory challenges, such as the
initiation of swallowing and cough reflexes. Research focusing on individuals with
severe post-stroke dysphagia has highlighted the importance of factors associated
with the recovery of oral intake, including motor and cognitive FIM, the presence of
aspiration, and pharyngeal residue.51) Instrumental assessments such as videofluoroscopy
(VF) and videoendoscopy (VE) provide detailed assessments of dysphagia. Given the
correlation between dysphagia at the time of hospitalization and subsequent motor
and cognitive outcomes, understanding the pathophysiology of dysphagia is considered
important.
This study has shown that dysphagia affects ADL performance and cognitive levels, and
when combined with previous research, it suggests a bidirectional causal
relationship between post-stroke dysphagia and these factors. Consequently, it is
suggested that stroke patients with dysphagia at admission require not only
dysphagia rehabilitation but also a comprehensive approach to enhance ADL
performance and cognitive function.
Supporting patients with dysphagia after stroke is an important issue. Several
approaches have been shown to improve ADL performance and dysphagia, such as
indirect and direct swallowing training, chair-stand exercises,25) improvement of oral
problems,52)
personalized nutritional support,27) and appropriate pharmacotherapy.31) Improvements in
dysphagia have been shown to contribute to improvements in ADL performance. A
multidisciplinary approach to dysphagia after stroke is important and may contribute
not only to improvements in dysphagia but also to improvements in ADL performance
and cognitive level. For patients with dysphagia, such as those in this study,
detailed assessments of swallowing function should be performed using VF and VE
tests. In addition, a multidisciplinary approach that includes dysphagia
rehabilitation, oral function rehabilitation, and nutritional support is essential.
Furthermore, it is important to recognize the possibility that baseline dysphagia
may be associated with rehabilitation outcomes and this understanding should be
shared by the entire multidisciplinary team.
This study has several limitations. First, this study was conducted at a single
institution, which may limit its generalizability. Second, this was a retrospective
study; therefore, there may be unexplored confounding factors. Third, factors such
as impaired consciousness, type of cerebrovascular accident, interval from stroke
onset to hospital admission, stroke severity, stroke characteristics, comprehensive
dysphagia assessment, rehabilitation motivation, and sensory impairment may
potentially influence patients’ post-stroke dysphagia, ADL performance, and
cognitive level.
CONCLUSION
Dysphagia at admission was associated with lower ADL performance and cognitive level
at discharge in convalescent patients after stroke. We suggest that patients with
post-stroke dysphagia should receive early evaluation of swallowing function through
a comprehensive multidisciplinary approach to improve ADL performance and cognitive
level.
ACKNOWLEDGMENTS
This research did not receive any specific grant from funding agencies in the public,
commercial, or not-for-profit sectors.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Thiyagalingam S, Kulinski AE,
Thorsteinsdottir B, Shindelar KL, Takahashi PY: Dysphagia in older adults. Mayo
Clin Proc 2021;96:488–497. PMID:33549267,
DOI:10.1016/j.mayocp.2020.08.001
- 2. Burgos R, Bretón I, Cereda E, Desport JC,
Dziewas R, Genton L, Gomes F, Jésus P, Leischker A, Muscaritoli M, Poulia KA,
Preiser JC, Van der Marck M, Wirth R, Singer P, Bischoff SC: ESPEN guideline
clinical nutrition in neurology. Clin Nutr 2018;37:354–396. PMID:29274834,
DOI:10.1016/j.clnu.2017.09.003
- 3. Jo SY, Hwang JW, Pyun SB: Relationship
between cognitive function and dysphagia after stroke. Ann Rehabil Med
2017;41:564–572. PMID:28971040, DOI:10.5535/arm.2017.41.4.564
- 4. Cha S, Kim WS, Kim KW, Han JW, Jang HC,
Lim S, Paik NJ: Sarcopenia is an independent risk factor for dysphagia in
community-dwelling older adults. Dysphagia 2019;34:692–697. PMID:30612233,
DOI:10.1007/s00455-018-09973-6
- 5. Yoshimura Y, Wakabayashi H, Bise T,
Nagano F, Shimazu S, Shiraishi A, Yamaga M, Koga H: Sarcopenia is associated
with worse recovery of physical function and dysphagia and a lower rate of home
discharge in Japanese hospitalized adults undergoing convalescent
rehabilitation. Nutrition 2019;61:111–118. PMID:30710883,
DOI:10.1016/j.nut.2018.11.005
- 6. Ministry of Health, Labour and Welfare:
Response to the increasing number of diseases caused by the aging of the
population [in Japanese]. Tokyo: Ministry of Heath, Labour and Welfare. 2016.
https://www.mhlw.go.jp/file/05-Shingikai-10801000-Iseikyoku-Soumuka/0000135467.pdf.
Accessed 2 Aug 2022.
- 7. Martino R, Foley N, Bhogal S, Diamant N,
Speechley M, Teasell R: Dysphagia after stroke: incidence, diagnosis, and
pulmonary complications. Stroke 2005;36:2756–2763. PMID:16269630,
DOI:10.1161/01.STR.0000190056.76543.eb
- 8. Gottlieb D, Kipnis M, Sister E, Vardi Y,
Brill S: Validation of the 50 ml3 drinking test for evaluation of post-stroke
dysphagia. Disabil Rehabil 1996;18:529–532. PMID:8902426,
DOI:10.3109/09638289609166040
- 9. DePippo KL, Holas MA, Reding MJ, Mandel
FS, Lesser ML: Dysphagia therapy following stroke: a controlled trial. Neurology
1994;44:1655–1660. PMID:7936292, DOI:10.1212/WNL.44.9.1655
- 10. Bath PM, Lee HS, Everton LF: Swallowing
therapy for dysphagia in acute and subacute stroke. Cochrane Libr
2018;10:CD000323. PMID:30376602,
DOI:10.1002/14651858.CD000323.pub3
- 11. Matsuo K, Sekimoto Y, Okamoto M, Shibata
S, Otaka Y: Association between oral health status and oral food intake level in
subacute stroke patients admitted to a convalescent rehabilitation unit.
Gerodontology 2022;39:67–73. PMID:34448242,
DOI:10.1111/ger.12586
- 12. Foley NC, Martin RE, Salter KL, Teasell
RW: A review of the relationship between dysphagia and malnutrition following
stroke. J Rehabil Med 2009;41:707–713. PMID:19774302,
DOI:10.2340/16501977-0415
- 13. Sunahara T, Yoshimura Y, Bise T, Shimazu
S: Swallowing function and nutritional status affect discharge home after
convalescent rehabilitation [in Japanese]. JSPEN
2020;2:262–269.
- 14. Gunaydin R, Karatepe AG, Kaya T, Ulutas
O: Determinants of quality of life (QoL) in elderly stroke patients: a
short-term follow-up study. Arch Gerontol Geriatr 2011;53:19–23. PMID:20598382,
DOI:10.1016/j.archger.2010.06.004
- 15. Meijer R, Ihnenfeldt DS, van Limbeek J,
Vermeulen M, de Haan RJ: Prognostic factors in the subacute phase after stroke
for the future residence after six months to one year. A systematic review of
the literature. Clin Rehabil 2003;17:512–520. PMID:12952157,
DOI:10.1191/0269215503cr644oa
- 16. Springer MV, Skolarus LE, Feng C, Burke
JF: Functional impairment and postacute care discharge setting may be useful for
stroke survival prognostication. J Am Heart Assoc 2022;11:e024327.
DOI:10.1161/JAHA.121.024327
- 17. Matsuo H, Yoshimura Y, Fujita S, Maeno Y:
Dysphagia is associated with poor physical function in patients with acute heart
failure: a prospective cohort study. Aging Clin Exp Res 2020;32:1093–1099.
PMID:31368089, DOI:10.1007/s40520-019-01287-3
- 18. Kunieda K, Ohno T, Fujishima I, Hojo K,
Morita T: Reliability and validity of a tool to measure the severity of
dysphagia: the Food Intake LEVEL Scale. J Pain Symptom Manage 2013;46:201–206.
PMID:23159683, DOI:10.1016/j.jpainsymman.2012.07.020
- 19. Chen LK, Woo J, Assantachai P, Auyeung
TW, Chou MY, Iijima K, Jang HC, Kang L, Kim M, Kim S, Kojima T, Kuzuya M, Lee
JS, Lee SY, Lee WJ, Lee Y, Liang CK, Lim JY, Lim WS, Peng LN, Sugimoto K, Tanaka
T, Won CW, Yamada M, Zhang T, Akishita M, Arai H: Asian Working Group for
Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am
Med Dir Assoc 2020;21:300–307. PMID:32033882,
DOI:10.1016/j.jamda.2019.12.012
- 20. Ottenbacher KJ, Hsu Y, Granger CV,
Fiedler RC: The reliability of the functional independence measure: a
quantitative review. Arch Phys Med Rehabil 1996;77:1226–1232. PMID:8976303,
DOI:10.1016/S0003-9993(96)90184-7
- 21. Bouillanne O, Morineau G, Dupont C,
Coulombel I, Vincent JP, Nicolis I, Benazeth S, Cynober L, Aussel C: Geriatric
Nutritional Risk Index: a new index for evaluating at-risk elderly medical
patients. Am J Clin Nutr 2005;82:777–783. PMID:16210706,
DOI:10.1093/ajcn/82.4.777
- 22. Banks JL, Marotta CA: Outcomes validity
and reliability of the modified Rankin scale: implications for stroke clinical
trials: a literature review and synthesis. Stroke 2007;38:1091–1096.
PMID:17272767, DOI:10.1161/01.STR.0000258355.23810.c6
- 23. Charlson ME, Pompei P, Ales KL, MacKenzie
CR: A new method of classifying prognostic comorbidity in longitudinal studies:
development and validation. J Chronic Dis 1987;40:373–383. PMID:3558716,
DOI:10.1016/0021-9681(87)90171-8
- 24. Nagano F, Yoshimura Y, Bise T, Shimazu S,
Shiraishi A: Muscle mass gain is positively associated with functional recovery
in patients with sarcopenia after stroke. J Stroke Cerebrovasc Dis
2020;29:105017. PMID:32807432,
DOI:10.1016/j.jstrokecerebrovasdis.2020.105017
- 25. Yoshimura Y, Wakabayashi H, Nagano F,
Bise T, Shimazu S, Shiraishi A: Chair‐stand exercise improves post‐stroke
dysphagia. Geriatr Gerontol Int 2020;20:885–891. PMID:32772455,
DOI:10.1111/ggi.13998
- 26. Kido Y, Yoshimura Y, Wakabayashi H,
Momosaki R, Nagano F, Bise T, Shimazu S, Shiraishi A: Sarcopenia is associated
with incontinence and recovery of independence in urination and defecation in
post-acute rehabilitation patients. Nutrition 2021;91-92:111397. PMID:34364264,
DOI:10.1016/j.nut.2021.111397
- 27. Shimazu S, Yoshimura Y, Kudo M, Nagano F,
Bise T, Shiraishi A, Sunahara T: Frequent and personalized nutritional support
leads to improved nutritional status, activities of daily living, and dysphagia
after stroke. Nutrition 2021;83:111091. PMID:33388653,
DOI:10.1016/j.nut.2020.111091
- 28. Shiraishi A, Wakabayashi H, Yoshimura Y:
Oral management in rehabilitation medicine: oral frailty, oral sarcopenia, and
hospital-associated oral problems. J Nutr Health Aging 2020;24:1094–1099.
PMID:33244566, DOI:10.1007/s12603-020-1439-8
- 29. Yoshimura Y, Shiraishi A, Tsuji Y,
Momosaki R: Oral management and the role of dental hygienists in convalescent
rehabilitation. Prog Rehabil Med 2022;7:20220019. PMID:35495548,
DOI:10.2490/prm.20220019
- 30. Matsumoto A, Yoshimura Y, Nagano F, Bise
T, Kido Y, Shimazu S, Shiraishi A: Polypharmacy and potentially inappropriate
medications in stroke rehabilitation: prevalence and association with outcomes.
Int J Clin Pharm 2022;44:749–761. PMID:35578145,
DOI:10.1007/s11096-022-01416-5
- 31. Yoshimura Y, Matsumoto A, Momosaki R:
Pharmacotherapy and the role of pharmacists in rehabilitation medicine. Prog
Rehabil Med 2022;7:20220025. PMID:35633757,
DOI:10.2490/prm.20220025
- 32. Yoshimura Y, Wakabayashi H, Nagano F,
Matsumoto A, Shimazu S, Shiraishi A, Kido Y, Bise T: The applicability of the
ESPEN and EASO-defined diagnostic criteria for sarcopenic obesity in Japanese
patients after stroke: prevalence and association with outcomes. Nutrients
2022;14:4205. PMID:36235857, DOI:10.3390/nu14194205
- 33. Beninato M, Gill-Body KM, Salles S, Stark
PC, Black-Schaffer RM, Stein J: Determination of the minimal clinically
important difference in the FIM instrument in patients with stroke. Arch Phys
Med Rehabil 2006;87:32–39. PMID:16401435,
DOI:10.1016/j.apmr.2005.08.130
- 34. Matsuo H, Yoshimura Y, Ishizaki N, Ueno
T: Dysphagia is associated with functional decline during acute‐care
hospitalization of older patients. Geriatr Gerontol Int 2017;17:1610–1616.
PMID:27910255, DOI:10.1111/ggi.12941
- 35. Ito Y, Goto T, Huh JY, Yamamura O, Hamano
T, Kikuta KI, Hayashi H: Development of a scoring system to predict prolonged
post-stroke dysphagia remaining at discharge from a subacute care hospital to
the home. J Stroke Cerebrovasc Dis 2021;30:105804. PMID:33906072,
DOI:10.1016/j.jstrokecerebrovasdis.2021.105804
- 36. Maeshima S, Osawa A, Hayashi T, Tanahashi
N: Factors associated with prognosis of eating and swallowing disability after
stroke: a study from a community-based stroke care system. J Stroke Cerebrovasc
Dis 2013;22:926–930. PMID:23680686,
DOI:10.1016/j.jstrokecerebrovasdis.2013.04.003
- 37. Kojima A, Imoto Y, Osawa Y, Fujieda S:
Predictor of rehabilitation outcome for dysphagia. Auris Nasus Larynx
2014;41:294–298. PMID:24560094, DOI:10.1016/j.anl.2013.12.009
- 38. Meyer MJ, Pereira S, McClure A, Teasell
R, Thind A, Koval J, Richardson M, Speechley M: A systematic review of studies
reporting multivariable models to predict functional outcomes after post-stroke
inpatient rehabilitation. Disabil Rehabil 2015;37:1316–1323. PMID:25250807,
DOI:10.3109/09638288.2014.963706
- 39. Senda J, Ito K, Kotake T, Mizuno M,
Kishimoto H, Yasui K, Nakagawa-Senda H, Katsuno M, Nishida Y, Sobue G:
Association between National Institutes of Health Stroke Scale and Functional
Independence Measure scores in patients with ischemic stroke from convalescent
rehabilitation outcomes. Nagoya J Med Sci 2023;85:428–443. PMID:37829489,
DOI:10.18999/nagjms.85.3.428
- 40. Miyazaki Y, Kawakami M, Kondo K,
Tsujikawa M, Honaga K, Suzuki K, Tsuji T: Comparing the contribution of each
clinical indicator in predictive models trained on 980 subacute stroke patients:
a retrospective study. Sci Rep 2023;13:12324. PMID:37516806,
DOI:10.1038/s41598-023-39475-x
- 41. Liu CH, Huo M, Qin HH, Zhao BL: Critical
prognostic factors for poststroke dysphagia: a meta-analysis. Eur Rev Med
Pharmacol Sci 2022;26:610–622. PMID:35113437,
DOI:10.26355/eurrev_202201_27888
- 42. Ikenaga Y, Nakayama S, Taniguchi H, Ohori
I, Komatsu N, Nishimura H, Katsuki Y: Factors predicting recovery of oral intake
in stroke survivors with dysphagia in a convalescent rehabilitation ward. J
Stroke Cerebrovasc Dis 2017;26:1013–1019. PMID:28108097,
DOI:10.1016/j.jstrokecerebrovasdis.2016.12.005
- 43. Scherbakov N, von Haehling S, Anker SD,
Dirnagl U, Doehner W: Stroke induced sarcopenia: muscle wasting and disability
after stroke. Int J Cardiol 2013;170:89–94. PMID:24231058,
DOI:10.1016/j.ijcard.2013.10.031
- 44. Kuroda Y, Kuroda R: Relationship between
thinness and swallowing function in Japanese older adults: implications for
sarcopenic dysphagia. J Am Geriatr Soc 2012;60:1785–1786. PMID:22985156,
DOI:10.1111/j.1532-5415.2012.04123.x
- 45. Fujishima I, Fujiu-Kurachi M, Arai H,
Hyodo M, Kagaya H, Maeda K, Mori T, Nishioka S, Oshima F, Ogawa S, Ueda K,
Umezaki T, Wakabayashi H, Yamawaki M, Yoshimura Y: Sarcopenia and dysphagia:
position paper by four professional organizations. Geriatr Gerontol Int
2019;19:91–97. PMID:30628181, DOI:10.1111/ggi.13591
- 46. Li Y, Xu Z, Zhang X, Ma D, Meng X, Zhang
M, Sun J: Predictors of complete oral feeding resumption after feeding tube
placement in patients with stroke and dysphagia: a systematic review. J Clin
Nurs 2023;32:2533–2546. PMID:35676778, DOI:10.1111/jocn.16404
- 47. Fernández-Pombo A, Seijo-Raposo IM,
López-Osorio N, Cantón-Blanco A, González-Rodríguez M, Arias-Rivas S,
Rodríguez-Yáñez M, Santamaría-Nieto A, Díaz-Ortega C, Gómez-Vázquez E,
Martínez-Olmos MÁ: Lesion location and other predictive factors of dysphagia and
its complications in acute stroke. Clin Nutr ESPEN 2019;33:178–182.
PMID:31451257, DOI:10.1016/j.clnesp.2019.05.019
- 48. Jørgensen HS, Nakayama H, Raaschou HO,
Olsen TS: Intracerebral hemorrhage versus infarction: stroke severity, risk
factors, and prognosis. Ann Neurol 1995;38:45–50. PMID:7611724,
DOI:10.1002/ana.410380110
- 49. Crisan D, Shaban A, Boehme A, Dubin P,
Juengling J, Schluter LA, Albright KC, Beasley TM, Martin-Schild S: Predictors
of recovery of functional swallow after gastrostomy tube placement for dysphagia
in stroke patients after inpatient rehabilitation: a pilot study. Ann Rehabil
Med 2014;38:467–475. PMID:25229025,
DOI:10.5535/arm.2014.38.4.467
- 50. Jang S, Yang HE, Yang HS, Kim DH: Lesion
characteristics of chronic dysphagia in patients with supratentorial stroke. Ann
Rehabil Med 2017;41:225–230. PMID:28503455,
DOI:10.5535/arm.2017.41.2.225
- 51. Calvo I, Pizzorni N, Gilardone G, Mayer
F, Vanacore N, Buraschi V, Gilardone M, Corbo M: Predictors of oral feeding
resumption after stroke in a rehabilitation hospital: a retrospective study. J
Stroke Cerebrovasc Dis 2019;28:1958–1970. PMID:30981584,
DOI:10.1016/j.jstrokecerebrovasdis.2019.03.040
- 52. Shiraisi A, Yoshimura Y, Wakabayashi H,
Nagano F, Bise T, Shimazu S: Improvement in oral health enhances the recovery of
activities of daily living and dysphagia after stroke. J Stroke Cerebrovasc Dis
2021;30:105961. PMID:34247054,
DOI:10.1016/j.jstrokecerebrovasdis.2021.105961