ABSTRACT
Objectives: It is essential to identify the factors that reduce the risk of frailty at discharge in patients with cardiovascular disease. We sought to verify the association between pre-admission hobbies and frailty at discharge in patients hospitalized for acute cardiovascular diseases.
Methods: We retrospectively analyzed the cases of the 269 patients admitted to our hospital with cardiovascular diseases, excluding those who required assistance with activities of daily living before admission or had missing data on hobbies or frailty. The patients’ pre-admission hobbies (if any) were recorded, and the patients were then classified into the no-hobby group, inactive-hobby group, or active-hobby group. Frailty was assessed using the Cardiovascular Health Study criteria (Japanese version) on the day before discharge. We conducted a multinomial logistic regression analysis to investigate the relationship between hobbies and frailty.
Results: Compared with the no-hobby group, the inactive-hobby group did not show a significantly lower odds ratio (OR) for pre-frailty and frailty. In contrast, the active-hobby group showed a significantly lower OR for pre-frailty and frailty even after adjustment (OR: 0.41, 95% confidence interval: 0.17–0.90). Regarding the components of frailty, the active-hobby group had lower ORs for slow gait speed, exhaustion, and low physical activity relative to the no-hobby group.
Conclusions: Even if patients had hobbies before admission, if those hobbies were non-active, they did not reduce the risk of frailty, suggesting the need for reconsidering rehabilitation approaches during hospitalization.
INTRODUCTION
Frailty in the elderly is a physiological state characterized by a decreased reserve capacity, resulting in vulnerability to stress.1) Frailty has been reported to increase in prevalence with aging, and in Japan, which has a high population of aged citizens, there is concern about the growing number of individuals with frailty. Persons with cardiovascular diseases have a higher prevalence of frailty when compared with community-dwelling people, and frailty is a contributing factor to increased cardiovascular disease and mortality risk.2,3) During hospitalization for cardiovascular diseases, a significant number of patients experience a decline in physical function because of inactivity.4) Frailty is a factor that increases the risk of developing various diseases and the need for care. Therefore, it important to consider factors that can reduce the risk of frailty at the time of discharge in patients with cardiovascular disease.5,6)
In a study of community-dwelling older adults, a 10% reduction in the risk of death over a 6-year period was reported for the subjects with two or more hobbies when compared with those without any hobbies.7) Other investigations of community-dwelling older adults over a 3-year period revealed that having one or more hobbies was also associated with better physical function, whereas the individuals without hobbies had a higher risk of requiring care certification.8,9) Furthermore, in a study that covered a 4-year period, older individuals with hobbies were observed to show a reduced risk of developing frailty.10) Therefore, we speculated that having a hobby may help maintain physical function and prevent frailty even after the onset of cardiovascular disease. However, patient hobby status before hospitalization for cardiovascular disease and the specific hobbies associated with frailty have not been established. We conducted the present study to test the hypothesis that patients with active hobbies before their admission for acute cardiovascular diseases have a lower risk of frailty at the time of discharge than patients without active hobbies.
MATERIALS AND METHODS
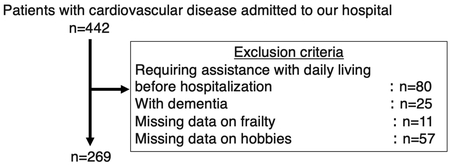
This was a retrospective observational investigation of patients at an acute-care hospital in Japan. The subjects were 442 patients with cardiovascular disease who were admitted to our hospital from 5 January 2019 to 30 June 2023 and subsequently discharged to their homes. Cardiovascular disease included heart failure, myocardial infarction, angina pectoris, coronary artery bypass grafting, aortic valve replacement, mitral valvuloplasty, and aortic graft replacement. The flowchart of the patient enrollment is shown in Fig. 1. The following patients were excluded: those requiring assistance with activities of daily living (ADL) before admission (n=80), those with dementia (n=25), and those for whom data regarding hobbies or frailty were missing (n=68). The final analysis included 269 subjects.
Hobby CategorizationAfter the stabilization of each patient’s condition following their admission for cardiovascular disease, we obtained information on any hobbies that the patient may have pursued. Because the evaluation of frailty is primarily based on physical aspects, we classified the patients’ hobbies from the perspective of whether the hobbies involved physical activities. We categorized the patients into three groups based on previous research7): the active-hobby group of patients whose hobbies involved physical activities, the non-active hobby group of patients whose hobbies did not require physical activity, and the no-hobby group of patients who did not have any hobbies. We classified the patients who had both active and inactive hobbies as members of the active-hobby group.
Measurement of FrailtyFrailty was assessed according to the Japanese version of the Cardiovascular Health Study (J-CHS) criteria on the day before the patient’s discharge.11) J-CHS is widely employed both clinically and academically as a valid method for the assessment of frailty.12) Its use is recommended in the cardiac rehabilitation guidelines.12) The J-CHS criteria for frailty include five items: low grip strength, slow gait speed, exhaustion, weight loss, and low physical activity. Grip strength was measured with the subject in an upright position, using a Smedley-style handgrip dynamometer (Takei Kiki Kogyo, Tokyo, Japan) for both the left and right hands. A maximum grip strength less than 28 kg for men and less than 18 kg for females was considered low grip strength. Gait speed was measured by having the patient walk 6 m at his or her usual speed. Slow gait speed was defined as 1 m/s or slower. Exhaustion was defined as a “yes” response to the question: “Do you feel tired for no apparent reason?” Weight loss was defined as a current weight that was at least 2 kg less than the weight recorded 6 months earlier. If the patient had shown edema because of a condition such as heart failure 6 months before this assessment, the weight at the stage before the edema was considered. The patient’s weight on the day before discharge was considered the “dry weight,” even for heart failure patients, and it was recorded in a state without edema. Low physical activity was defined as a “no” response to the question: “Did you engage in regular physical activities, sports, or farming before your admission?” We classified the patients who met any three of the above-described criteria as frail; those meeting one or two criteria were classified as pre-frail, and those meeting zero criteria were classified as robust.
In investigating the association between pre-admission hobbies and frailty at discharge, it was anticipated that the frailty status before admission may influence the results. The Clinical Frailty Scale (CFS) was utilized for the assessment of pre-admission frailty in this study. The CFS is a clinical judgement-based frailty tool developed for the Canadian Study of Health and Aging13) and has been also evaluated in cardiovascular disease patients.14) The CFS evaluates the specific domains of comorbidity, function, and cognition to generate a frailty score ranging from 1 (very fit) to 9 (terminally ill).
Ethics ApprovalIn this study, we did not seek written informed consent from the patients themselves, because this was a minimal-risk, retrospective study and the data were anonymized according to the Declaration of Helsinki. Furthermore, there were no invasive procedures or interventions. Information was provided to the patients via the hospital website and informed consent was obtained as an alternative response to the opt-out method based on the guidelines of the Ministry of Health, Labour, and Welfare of Japan. The study was approved by the Aso Iizuka Hospital Ethics Committee (approval number: 22131).
Statistical AnalysesThe characteristics of the patients in the three hobby groups were compared by one-way analysis of variance (ANOVA) and post-hoc tests (Bonferroni). A multinomial logistic regression analysis was performed to examine the associations between each of the three hobby groups and frailty as well as the components of frailty. We calculated the odds ratios (ORs) and 95% confidence intervals (CIs) for presenting pre-frailty and frailty, with the no-hobby group acting as the reference group. The adjusted factors included age, sex, body mass index (BMI), disease classification (myocardial infarction, heart failure, others), length of hospital stay, employment status, left ventricular ejection fraction at admission, and CFS score before admission. All statistical analyses were performed using STATA ver. 17 software, with the significance level set at <5%.
RESULTS
The division of hobbies between the active- and non-active-hobby groups is presented in Table 1. Differences in characteristics among the three hobby groups are shown in Table 2. Significant differences were observed in age, gender, disease classification, left ventricular ejection fraction, CFS score before admission, the prevalence of frailty at discharge, the prevalence of slow gait speed, the prevalence of exhaustion (components of frailty), isometric knee extension strength, and body fat percentage.
Table 1. Division of hobbies into non-active and active groups
| Hobby group | List of hobbies |
| Non-active | Chorus, dinner with friends, karaoke, go, shogi, drinking, physiognomy, mahjong, harmonica, board games, driving, watching TV or movies, guitar, reading, horse racing, cooking, pachinko, photography, sewing, music appreciation, watercolor painting, patchwork, pressing flowers, haiku, investing, knitting, newspapers, touring, hot springs, watching sports, playing a musical instrument, pencil drawing, Internet browsing, tea ceremony, boat racing |
| Active | Bowling, golf, table tennis, softball, kendo, gateball, volunteer work, aikido, baseball, ground golf, basketball, badminton, gymnastics, fishing, mountain climbing, farm work, dog walking, jogging, carpentry, travel, gardening, cycling, walking, shopping, visiting Buddhist temples, visiting castles, yard work, pruning, aerobics, picking wild vegetables, DIY (do-it-yourself) activities, dancing, weeding, swimming, windsurfing |
Table 2. Comparison of characteristics between the three patient groups
| Overall
n=269 | No hobby
n=77 (28.6%) | Non-active hobby
n=64 (23.8%) | Active hobby
n=128 (47.6%) | P value |
| Age (years) | 68.4 ± 11.5 | 64.9 ± 12.3 | 69.6 ± 12.7 | 69.9 ± 10.0 | 0.01 |
| Male | 195 (72.2) | 48 (62.3) | 44 (68.8) | 103 (80.5) | 0.01 |
| BMI (kg/m2) | 23.0 ± 3.7 | 23.4 ± 3.7 | 22.6 ± 3.9 | 23.1 ± 3.5 | 0.27 |
| Employed | 116 (43.0) | 38 (49.4) | 27 (42.2) | 51 (39.8) | 0.406 |
| Disease | | | | | 0.03 |
| Ischemic heart disease | 77 (28.6) | 31 (40.3) | 24 (37.5) | 54 (42.2) | |
| Heart failure | 64 (23.8) | 26 (33.8) | 19 (29.7) | 21 (16.4) |
| Other disease | 128 (47.6) | 20 (26.0) | 21 (32.8) | 53 (41.4) |
Left ventricular ejection
fraction (%) | 50.9±14.2 | 46.9±14.4 | 50.4±14.1 | 53.5±13.8 | <0.01 |
| Length of hospital stay (days) | 18 [12–25] | 17 [11–25] | 18.5 [13–30.5] | 18 [12–25] | 0.51 |
| CFS score before admission | | | | <0.01 |
| 1 | 113 (42.0) | 43 (55.8) | 31 (48.4) | 39 (30.5) | |
| 2 | 70 (26.0) | 30 (39.0) | 24 (37.5) | 16 (12.5) |
| 3 | 46 (17.1) | 0 (0) | 1 (1.6) | 45 (35.2) |
| 4 | 23 (8.6) | 0 (0) | 0 (0) | 23 (18.0) |
| 5 | 11 (4.1) | 3 (3.9) | 6 (9.4) | 2 (1.6) |
| 6 | 6 (2.2) | 1 (1.3) | 2 (3.1) | 3 (2.3) |
| J-CHS at discharge | | | | | <0.01 |
| Robust | 52 (19.3) | 11 (15.7) | 6 (9.7) | 35 (28.7) | |
| Pre-frailty | 146 (54.1) | 43 (61.4) | 33 (53.2) | 70 (57.4) |
| Frailty | 56 (20.7) | 16 (22.9) | 23 (37.1) | 17 (13.9) |
| Low grip strength | 31 (11.5) | 9 (30.0) | 6 (23.1) | 16 (22.9) | 0.73 |
| Slow gait speed | 21 (7.8) | 9 (30.0) | 5 (20.0) | 7 (10.1) | 0.048 |
| Exhaustion | 11 (4.1) | 6 (20.7) | 4 (17.4) | 1 (1.5) | <0.01 |
| Low physical activity | 11 (4.1) | 5 (17.2) | 2 (8.7) | 4 (5.8) | 0.2 |
| Weight loss | 17 (6.3) | 6 (20.7) | 5 (21.7) | 6 (8.7) | 0.15 |
| Isometric knee extensor muscle strength at discharge (kgf) | 27.7 ± 12.1 | 26.3 ± 10.7 | 23.9 ± 11.4 | 30.2 ± 12.6 | <0.01 |
| PHQ-9 score at discharge | 3 [1–7] | 4 [1–7] | 4 [1–9] | 3 [1–6.5] | 0.52 |
| Skeletal muscle mass index at discharge (kg/m2) | 6.7 ± 1.1 | 6.6 ± 1.2 | 6.4 ± 1.1 | 6.9 ± 1.1 | <0.01 |
| Body fat at discharge (%) | 26.3 ± 8.1 | 28.1 ± 8.0 | 26.1 ± 9.6 | 25.4 ± 7.4 | 0.02 |
Data are given as mean ± standard deviation, median [25%–75% percentiles], or number (%percentage). The χ2-test was used for comparisons of proportions, the Kruskal-Wallis test for comparisons of medians, and ANOVA for comparisons of means, with respective P values shown. PHQ-9, Patient Health Questionnaire-9.
The results of the logistic regression analysis of the associations between frailty and hobbies are presented in Table 3. The numbers (percentages) of pre-frailty/frailty individuals in the three hobby groups were as follows: no-hobby group, n=43 patients (61.4%)/16 (22.9%); non-active-hobby group, n=33 (53.2%)/23 (37.1%); active-hobby group: n=70 (57.4%)/17 (13.9%). Compared with the no-hobby group, the non-active-hobby group did not show a significant decrease in the OR for pre-frailty and frailty, whereas the active-hobby group exhibited a significantly lower OR for pre-frailty and frailty (OR 0.46, 95%CI: 0.21–0.98). This significance remained unchanged even after the adjustment for confounding factors (OR 0.41, 95% CI: 0.17–0.90).
Table 3. Association between frailty and hobbies
| Hobby | n (%) | Pre-frailty and Frailty
n (%) | | Non-adjusted | | Adjusted |
| Pre-frailty | Frailty | | OR | 95% CI | P value | | OR | 95% CI | P value |
| None | 77 (28.6) | 43 (61.4) | 16 (22.9) | | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 33 (53.2) | 23 (37.1) | | 1.74 | 0.60–5.02 | 0.31 | | 1.56 | 0.52–4.64 | 0.38 |
| Active | 128 (47.6) | 70 (57.4) | 17 (13.9) | | 0.46 | 0.21–0.98 | 0.046 | | 0.41 | 0.17–0.90 | 0.04 |
Adjustment factors: age, sex, BMI, disease, length of hospital stay, employment status, left ventricular ejection fraction at admission, CFS score before admission.
The results of the logistic regression analysis of the association between components of frailty and hobbies are presented in Table 4. After adjustment for confounding factors, the active-hobby group had significantly lower ORs than the no-hobby group for slow gait speed, exhaustion, and low physical activity.
Table 4. Association between components of frailty and hobbies
| Hobby | n (%) | Applicable people
n (%) | Non-adjusted | | Adjusted |
| OR | 95% CI | P value | | OR | 95% CI | P value |
| Low grip strength |
| None | 77 (28.6) | 9 (30.0) | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 6 (23.1) | 2.31 | 1.15–4.63 | 0.02 | | 1.69 | 0.74–3.89 | 0.21 |
| Active | 128 (47.6) | 16 (22.9) | 0.90 | 0.49–1.67 | 0.74 | | 0.56 | 0.25–1.24 | 0.15 |
| Slow gait speed |
| None | 77 (28.6) | 9 (30.0) | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 5 (20.0) | 1.25 | 0.61–2.57 | 0.53 | | 0.91 | 0.40–2.07 | 0.83 |
| Active | 128 (47.6) | 7 (10.1) | 0.49 | 0.25–0.96 | 0.04 | | 0.31 | 0.14–0.71 | 0.006 |
| Exhaustion |
| None | 77 (28.6) | 6 (20.7) | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 4 (17.4) | 1.10 | 0.55–2.19 | 0.79 | | 1.16 | 0.56–2.39 | 0.69 |
| Active | 128 (47.6) | 1 (1.5) | 0.39 | 0.21–0.74 | <0.01 | | 0.47 | 0.23–0.96 | 0.038 |
| Weight loss |
| None | 77 (28.6) | 6 (20.7) | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 5 (21.7) | 1.12 | 0.54–2.32 | 0.77 | | 0.91 | 0.41–2.04 | 0.82 |
| Active | 128 (47.6) | 6 (8.7) | 0.87 | 0.46–1.64 | 0.66 | | 0.78 | 0.37–1.66 | 0.52 |
| Low physical activity |
| None | 77 (28.6) | 5 (17.2) | 1.00 | Ref. | Ref. | | 1.00 | Ref. | Ref. |
| Non-active | 64 (23.8) | 2 (8.7) | 1.10 | 0.55–2.18 | 0.81 | | 1.07 | 0.53–2.21 | 0.88 |
| Active | 128 (47.6) | 4 (5.8) | 0.54 | 0.29–1.00 | 0.051 | | 0.49 | 0.25–0.96 | 0.04 |
Adjustment factors: age, sex, BMI, disease, length of hospital stay, employment status, left ventricular ejection fraction at admission, CFS score before admission.
DISCUSSION
We believe this study to be the first published investigation into the relationship between pre-admission hobbies categorized by the level of physical activity and the risk of frailty at the time of discharge in cardiovascular disease patients admitted to an acute-care hospital. The results of our analyses revealed that only the patients who had active hobbies had a lower risk of frailty at the time of discharge compared with those without hobbies. Analysis of the components of frailty (i.e., slow gait speed, exhaustion, and low physical activity) demonstrated that only the patients with active hobbies had lower risks for these components.
Characteristics of Hobbies in Patients with Cardiovascular Disease during Acute HospitalizationThe patients’ hobbies varied widely: 192 individuals (71.4%) reported having one or more hobbies, which is comparable with the percentage observed in community-dwelling older adults (71.1%).7) Among the present patients with hobbies, there was a tendency for a higher prevalence of hobbies involving physical activity. Notably, the patients with active hobbies exhibited higher physical function at the time of their discharge than patients of the other two hobby groups. In the active-hobby group, there was a relatively low number of patients with heart failure. Given that heart failure symptoms persist chronically, it is conceivable that many patients with heart failure in this group might not have engaged in active hobbies before admission. Moreover, during hospitalization, periods of inability to engage in high-intensity exercise therapy because of symptoms and treatment of heart failure might be prevalent, potentially resulting in a higher risk of presenting frailty at discharge for groups with a higher proportion of patients with heart failure. Although we analyzed disease classification as an adjusting factor in this study, the active-hobby group had a lower prevalence of heart failure patients and a shorter period of inactivity during hospitalization, which could have contributed to a lower risk of frailty at discharge.
Association between Active Hobbies and FrailtyThe patients with active hobbies had a lower risk of frailty at the time of discharge. This effect was attributed to their lower risks observed in the three components of frailty: slow gait speed, exhaustion, and low physical activity. Physical activity has been known to have a positive impact on muscle strength and balance ability, both of which are related to gait speed.15,16) Therefore, we expected the patients with active hobbies to have better physical function before their hospital admission, and consequently they might have maintained a fast gait speed even after admission. However, there are reports of patients who exhibited hospitalization-associated disability in which their ADLs were decreased after their hospitalization, and it was estimated that this occurs in about 7.5% of patients with a history of heart failure of 20 years or more and in 30%–40% of elderly patients.17,18) In other words, it may be difficult for hospitalized patients to resume an active hobby unless their physical functions are maintained during hospitalization to prevent the functions’ deterioration after hospitalization.
In the present study, the patients in the active-hobby group had a lower risk of exhaustion. Exhaustion is an indicator with both mental and physical aspects.1) Patients with active hobbies before their hospital admission might have maintained their mental vitality because of the desire to resume their hobbies after discharge, which requires the preservation of high physical function.19) Motivation for physical activity in patients with cardiac disease is positively associated with maximal oxygen uptake.20) Therefore, having active hobbies may serve as motivation for exercise or physical therapy, contributing to the maintenance of physical function. In addition, the presence of physical capacity for performing active hobbies before admission,21) which likely persists until discharge, could also have contributed to the present active-hobby patients’ reduced risk of exhaustion. Although the risks of low grip strength and weight loss tended to be lower in the patients with active hobbies, these associations were not statistically significant. This may be indicative of the challenge facing patients with cardiovascular disease when attempting to maintain their muscle mass and upper limb strength through activities. Further investigations with larger sample sizes are necessary to explore this issue. The patients in this study who had active hobbies before admission may have contributed to the preservation of their physical and mental function from a timepoint before their hospital admission to post-discharge.
Association between Non-active Hobbies and FrailtyThe non-active-hobby group did not exhibit a significantly lower risk of frailty at discharge, and they showed no associations with any of the components of frailty. Non-active, cultural hobbies have positive effects on cognitive function and mental well-being.22,23) However, in this study, no associations were found with frailty components, including exhaustion. One possibility is that subjects in previous studies engaged in non-active hobbies alongside active hobbies, which could have influenced the results. We clearly classified non-active and active hobbies in the present investigation. In addition, although patients received rehabilitation during hospitalization for cardiovascular disease, the level of physical activity of hospitalized patients tends to decrease relative to pre-admission levels. This suggests that the event of hospitalization itself might weaken the positive effects of non-active hobbies on the body.
The high state of objective physical function and exercise tolerance before admission because of activities other than hobbies may have influenced the lower risk of frailty at discharge. Although we could not assess the objective exercise function and exercise tolerance before admission in this study, it was suggested that regardless of the severity of pre-admission frailty, hobbies before admission were associated with frailty at discharge. The “hobbies” addressed in this study are activities enjoyed during leisure, and active hobbies involve physically engaging activities that can be enjoyable for each individual in the community. Therefore, the pursuit of active hobbies should be considered as a valid means to maintain high exercise tolerance or physical function before admission.
Study LimitationsThis study has several limitations. First, in this study, patients requiring assistance with ADL before admission were excluded, and severely ill patients requiring heart transplantation, prolonged use of inotropic drugs, or mechanical ventilation were not included. Therefore, there is a selection bias in this study. Second, we included only patients for whom hobby information was obtained. Cases in which hobby information could not be assessed are likely to exist, making it impossible to generalize our findings. Third, information about the objective physical function of patients before admission was not available. Therefore, it is possible that the results were influenced by the fact that patients with hobbies had good physical function or were not frail when assessed by J-CHS before admission. Fourth, detailed information such as the frequency and duration of the patients’ hobbies was not available. Given that we did not investigate the objective activity levels of active and non-active hobbies, a clear difference in activity levels between the two groups remains unclear. This study is the first to elucidate the relationship between hobbies before admission and frailty at discharge in patients with heart disease. By addressing the limitations of such studies as future research considerations, we believe this work can contribute to the construction of significant evidence for improving post-discharge outcomes.
CONCLUSION
Among 269 patients with cardiovascular disease who were admitted to an acute-care hospital, those with active hobbies before admission had a lower risk of developing frailty at the time of discharge than those without hobbies. However, the patients with non-active hobbies did not exhibit a significantly lower risk of frailty. In future research, it will be important to gather more detailed information about patients’ hobbies, including their frequency, duration, and years of engagement. Further investigation is also necessary to clarify the association between hobbies and long-term outcomes such as post-discharge physical function and readmission rates.
ACKNOWLEDGMENTS
We thank the patients and the cardiac rehabilitation staff at Iizuka Hospital for their cooperation in data collection. This research was conducted with the assistance of an Aso Iizuka Hospital Clinical Research Grant (approval date: 1 April, 2023). We received support from Iizuka Hospital for the purchase of literature management software and for the cost of article submission. We thank Iizuka Hospital for financial support.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, Cardiovascular Health Study Collaborative Research Group: Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146–M157. PMID:11253156, DOI:10.1093/gerona/56.3.M146
- 2. Wleklik M, Denfeld Q, Lisiak M, Czapla M, Kałużna-Oleksy M, Uchmanowicz I: Frailty syndrome in older adults with cardiovascular diseases—what do we know and what requires further research? Int J Environ Res Public Health 2022;19:2234. PMID:35206422, DOI:10.3390/ijerph19042234
- 3. Liu X, Tou NX, Gao Q, Gwee X, Wee SL, Ng TP: Frailty and risk of cardiovascular disease and mortality. PLoS One 2022;17:e0272527. PMID:36121826, DOI:10.1371/journal.pone.0272527
- 4. Covinsky KE, Palmer RM, Fortinsky RH, Counsell SR, Stewart AL, Kresevic D, Burant CJ, Landefeld CS: Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc 2003;51:451–458. PMID:12657063, DOI:10.1046/j.1532-5415.2003.51152.x
- 5. Chen S, Honda T, Narazaki K, Chen T, Kishimoto H, Kumagai S: Physical frailty and risk of needing long-term care in community-dwelling older adults: a 6-year prospective study in Japan. J Nutr Health Aging 2019;23:856–861. PMID:31641736, DOI:10.1007/s12603-019-1242-6
- 6. Lohman MC, Sonnega AJ, Resciniti NV, Leggett AN: Frailty phenotype and cause-specific mortality in the United States. J Gerontol A Biol Sci Med Sci 2020;75:1935–1942. PMID:31956891, DOI:10.1093/gerona/glaa025
- 7. Kobayashi T, Tani Y, Kino S, Fujiwara T, Kondo K, Kawachi I: Prospective study of engagement in leisure activities and all-cause mortality among older Japanese adults. J Epidemiol 2022;32:245–253. PMID:33551388, DOI:10.2188/jea.JE20200427
- 8. Zeng P, Han Y, Pang J, Wu S, Gong H, Zhu J, Li J, Zhang T: Sarcopenia-related features and factors associated with lower muscle strength and physical performance in older Chinese: a cross sectional study. BMC Geriatr 2016;16:45. PMID:26879964, DOI:10.1186/s12877-016-0220-7
- 9. Okura M, Ogita M, Yamamoto M, Nakai T, Numata T, Arai H: Community activities predict disability and mortality in community‐dwelling older adults. Geriatr Gerontol Int 2018;18:1114–1124. PMID:29603568, DOI:10.1111/ggi.13315
- 10. Wang Y, Chen Z, Zhou C: Social engagement and physical frailty in later life: does marital status matter? BMC Geriatr 2021;21:248. PMID:33858354, DOI:10.1186/s12877-021-02194-x
- 11. Satake S, Arai H: The revised Japanese version of the Cardiovascular Health Study criteria (revised J‐CHS criteria). Geriatr Gerontol Int 2020;20:992–993. PMID:33003255, DOI:10.1111/ggi.14005
- 12. Makita S, Yasu T, Akashi YJ, Adachi H, Izawa H, Ishihara S, Iso Y, Ohuchi H, Omiya K, Ohya Y, Okita K, Kimura Y, Koike A, Kohzuki M, Koba S, Sata M, Shimada K, Shimokawa T, Shiraishi H, Sumitomo N, Takahashi T, Takura T, Tsutsui H, Nagayama M, Hasegawa E, Fukumoto Y, Furukawa Y, Miura SI, Yasuda S, Yamada S, Yamada Y, Yumino D, Yoshida T, Adachi T, Ikegame T, Izawa KP, Ishida T, Ozasa N, Osada N, Obata H, Kakutani N, Kasahara Y, Kato M, Kamiya K, Kinugawa S, Kono Y, Kobayashi Y, Koyama T, Sas e Sato KSato Shibata SShibata Suzuki TSuzuki Tamaki NTamaki Yamaoka-Tojo DYamaoka-Tojo Nakanishi MNakanishi Nakane MNakane Nishizaki ENishizaki Higo MHigo Fujimi TFujimi Honda KHonda Matsumoto TMatsumoto Matsumoto YMatsumoto Miyawaki NMiyawaki Murata IMurata Yagi MYagi Yanase SYanase Yamada MYamada Yokoyama MYokoyama Watanabe MWatanabe Itoh NItoh Kimura HKimura Kyo TKyo Goto SGoto Nohara YNohara Hirata RHirata KIJapanese Circulation Society/the Japanese Association of Cardiac Rehabilitation Joint Working Group: JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Circ J 2022;87:155–235. PMID:36503954, DOI:10.1253/circj.CJ-22-0234
- 13. Sternberg SA, Schwartz AW, Karunananthan S, Bergman H, Clarfield AM: The identification of frailty: a systematic literature review. J Am Geriatr Soc 2011;59:2129–2138. PMID:22091630, DOI:10.1111/j.1532-5415.2011.03597.x
- 14. Singh M, Stewart R, White H: Importance of frailty in patients with cardiovascular disease. Eur Heart J 2014;35:1726–1731. PMID:24864078, DOI:10.1093/eurheartj/ehu197
- 15. Morie M, Reid KF, Miciek R, Lajevardi N, Choong K, Krasnoff JB, Storer TW, Fielding RA, Bhasin S, LeBrasseur NK: Habitual physical activity levels are associated with performance in measures of physical function and mobility in older men. J Am Geriatr Soc 2010;58:1727–1733. PMID:20738436, DOI:10.1111/j.1532-5415.2010.03012.x
- 16. Cheng IF, Kuo LC, Tsai YJ, Su FC: The comparisons of physical functional performances between older adults with and without regular physical activity in two different living settings. Int J Environ Res Public Health 2021;18:3561. PMID:33808083, DOI:10.3390/ijerph18073561
- 17. Ogawa M, Yoshida N, Nakai M, Kanaoka K, Sumita Y, Kanejima Y, Emoto T, Saito Y, Yamamoto H, Sakai Y, Hirota Y, Ogawa W, Iwanaga Y, Miyamoto Y, Yamashita T, Izawa KP, Hirata K: Hospital-associated disability and hospitalization costs for acute heart failure stratified by body mass index—insight from the JROAD/JROAD-DPC database. Int J Cardiol 2022;367:38–44. PMID:36029847, DOI:10.1016/j.ijcard.2022.08.044
- 18. Covinsky KE, Pierluissi E, Johnston CB: Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure”. JAMA 2011;306:1782–1793. PMID:22028354, DOI:10.1001/jama.2011.1556
- 19. Dhakal A, Kurisu K, Park S, Yoshiuchi K, Aoyagi Y: Association of psychosocial factors with physical activity among Japanese adults aged 65 and older: a 6-year repeated cross-sectional study from the Nakanojo study. Biopsychosoc Med 2023;17:32. PMID:37700326, DOI:10.1186/s13030-023-00289-y
- 20. Mikkelsen N, Dall CH, Frederiksen M, Holdgaard A, Rasmusen H, Prescott E: The motivation for physical activity is a predictor of VO2peak and is a useful parameter when determining the need for cardiac rehabilitation in an elderly cardiac population. PLoS One 2022;17:e0275091. PMID:36170331, DOI:10.1371/journal.pone.0275091
- 21. Mediano MF, Fleg JL, Wanigatunga AA, Gonçalves TR, Martinez-Amezcua P, Szklo M, Simonsick EM, Ferrucci L, Schrack JA: Association of physical activity with maximal and submaximal tests of exercise capacity in middle- and older-aged adults. J Aging Phys Act 2022;30:271–280. PMID:34407506, DOI:10.1123/japa.2020-0439
- 22. Sugita A, Ling L, Tsuji T, Kondo K, Kawachi I: Cultural engagement and incidence of cognitive impairment: a 6-year longitudinal follow-up of the Japan gerontological evaluation study (JAGES). J Epidemiol 2021;31:545–553. PMID:32963208, DOI:10.2188/jea.JE20190337
- 23. Noguchi T, Shang E: Art engagement and psychological well-being among community-dwelling older adults in Japan: an observational cross-sectional study. Public Health 2023;222:178–185. PMID:37556978, DOI:10.1016/j.puhe.2023.07.018