ABSTRACT
Objectives: Osteoporotic vertebral compression fractures (OVCFs) are
common in older individuals and lead to pain, spinal deformities, and limited
mobility. Paraspinal muscle function correlates with fracture severity, and this
association may be more significant in patients with lumbar spinal stenosis
(LSS). However, studies on the effects of OVCFs are lacking. This study aimed to
investigate the relationship between OVCFs, fat infiltration, and muscle atrophy
in patients with LSS.
Methods: This study included 177 patients with preoperative LSS, of
whom 16 had OVCFs and 161 did not. Lumbar lordosis angle, fat infiltration, and
paraspinal muscle atrophy were evaluated in these patients. Information on
patient characteristics such as smoking, diabetes, hemodialysis, steroid use,
American Society of Anesthesiologists score, and bladder or bowel dysfunction
were obtained from medical records. Logistic regression analysis was conducted
to identify factors independently associated with OVCF.
Results: Patients in the OVCF group were significantly older
(P=0.006) than those without fractures, and a higher proportion of the OVCF
group showed muscle atrophy (P=0.034). Significant variables and those with
moderate effect sizes were included in the logistic regression analysis. Muscle
atrophy (P=0.028) was independently associated with OVCF.
Conclusions: Muscle atrophy was associated with preoperative OVCFs
in patients with LSS. Identifying OVCFs in these patients may underscore the
importance of tailored treatment and rehabilitation strategies for the
paraspinal muscles.
INTRODUCTION
Vertebral compression fractures (VCFs) can cause severe pain, spinal deformities, and
limited mobility.1,2) In Japan, the prevalence of VCFs is reported to
range between 3.2% and 26.3% in males and between 9.5% and 19.6% in females, with
incidence increasing with age.3,4,5,6) VCFs occur when a significant axial compressive
force is applied to the vertebral body. However, in individuals with osteoporosis,
VCFs may be caused by minor external forces such as forward bending of the trunk or
sneezing. These fractures can affect spinal alignment, resulting in paraspinal
muscle dysfunction. Postinjury physical therapy is often necessary.7,8,9)
The paraspinal muscles, which run along the spine, play critical roles in maintaining
posture and controlling spinal movement. Research has indicated that fat
infiltration in these muscles increases following osteoporotic vertebral compression
fractures (OVCFs).10,11) The replacement of muscle with fat can result in
functional impairment and decreased spinal stability.12) Furthermore, it has been reported that
not only fat infiltration but also muscle atrophy or a reduced muscle
cross-sectional area is more likely to occur in patients with OVCFs12) and is associated with
OVCF severity.10) These
effects may be more pronounced in cases in which OVCFs coexist with lumbar
disorders.
The impact of fat infiltration and muscle atrophy in the paraspinal muscles has also
been demonstrated in patients with lumbar spinal stenosis (LSS),13,14,15,16) prompting the
development of specialized rehabilitation strategies. In patients with LSS, a
reduction in the paraspinal muscle cross-sectional area on preoperative magnetic
resonance imaging (MRI) is an indicator of poor surgical outcomes, as measured using
the Oswestry Disability Index and Core Outcome Measures Index.17)
Preoperative evaluation of the paraspinal muscles in patients with LSS complicated by
an OVCF is therefore essential to understand the condition of the patient and select
an appropriate postoperative rehabilitation strategy. However, there is currently a
lack of research on the relationship between OVCFs and LSS. This study aims to
clarify the association between preoperative OVCF and paraspinal muscle fat
infiltration and muscle atrophy in patients with LSS. We hypothesized that
preoperative patients with LSS and OVCF would demonstrate increased fat infiltration
and muscle atrophy in the paraspinal muscles. The findings of this study should
enhance our ability to predict patient outcomes and suggest opportunities for more
effective treatment and rehabilitation strategies.
MATERIALS AND METHODS
Study Design
This retrospective study was approved by the Ethics Review Committee of Saitama
Medical Center, Saitama Medical University (No. 1969-III). The study was
conducted in accordance with the principles outlined in the Declaration of
Helsinki. The requirement for written informed consent was waived by the Ethics
Review Committee because of the retrospective nature of the study. Instead, a
disclosure statement was posted on the Saitama Medical Center website, with
contact information for patients who wished to opt out; the data of eligible
patients who provided notification of their refusal would not be used in the
study.
Patients
This study reviewed the medical records of 221 patients with LSS (143 men and 78
women) scheduled for lumbar surgery at Saitama Medical Center between July 2013
and June 2017. Patients were excluded based on the following criteria: absence
of preoperative MRI data, aged less than 35 years, history of lumbar spine
surgery. The diagnosis of OVCF was double-checked by a physician and a physical
therapist (K. Suzuki. and S. Ogihara). The semiquantitative method, which
utilizes MRI, was employed, with cases corresponding to Grade 1 or higher
considered as OVCF. Patients were divided into two groups based on the absence
(non-OVCF group) or presence (OVCF group) of OVCF.
Data Collection
Patient clinical characteristics were collected from medical records completed by
the attending physician. This information included data on age, sex, body mass
index, smoking status, diabetes, hemodialysis, steroid use, American Society of
Anesthesiologists physical status score, and bladder or bowel dysfunction.
Outcome Measures
Fat Infiltration
The classification proposed by Kjaer et al.18) was used to assess fat
infiltration of the lumbar region paraspinal muscles. Our focus on the L4/5
level was based on reports suggesting a higher susceptibility to fat
infiltration in the lower lumbar vertebrae than in the upper lumbar
vertebrae.19) This method, which has been validated by
several previous studies,20,21,22,23,24) categorizes fat infiltration in the
paraspinal muscles into three grades based on the amount of fat within the
paraspinal muscles: grade 0, 0%–10%; grade 1, 10%–50%; and grade 2, >50%.
This assessment was conducted visually using MRI (Fig. 1).
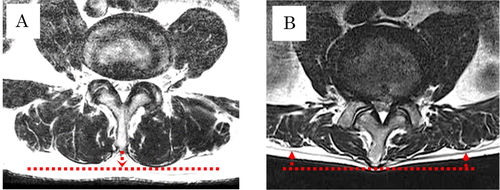
Muscle Atrophy
Takayama et al.24) proposed a method to evaluate paraspinal
muscle atrophy based on the correlation between the distance from the
posterior end of the spinous process to the bulge of the bilateral
paraspinal muscles and the cross-sectional area of the paraspinal muscles in
the lumbar region, as visualized using T2-weighted MRI.19) Subsequently,
Hasebe et al.25) proposed the visual confirmation of whether
the posterior end of the spinous process is positioned behind the posterior
end of the paraspinal muscles as a practical method of identifying severe
paraspinal muscle atrophy. They reported its utility as a tool for
interprofessional communication.25) In the current study, we adopted this
visual assessment method (Fig. 2).
In the evaluation of muscle atrophy, cross-sectional images were assessed at
multiple levels, including L1/2, L2/3, L3/4, and L4/5. This approach was
adopted to investigate the impact on the lumbar muscles. If muscle atrophy
was identified at any of these levels, the patient was classified as having
muscle atrophy for the purposes of the current study. A physician and a
physical therapist (S. Ogihara and K. Suzuki.) collaboratively assessed fat
infiltration and muscle atrophy.
The lumbar lordosis angle (LLA) was measured from lateral preoperative
radiographs in the standing position, as described previously.26,27) The
intersection angle was measured between the extension lines of the upper end
of L1 and the lower end of L5. Angle measurements were performed by a single
spine surgeon (S. Ogihara).
Statistical Analysis
Data are expressed as mean ± standard deviation or number (percentage). The
normality of the data was assessed using the Shapiro–Wilk test. Categorical
variables were compared using the χ2 test, whereas continuous
variables were compared using either the Mann–Whitney U test or
t-test, depending on the distribution. Logistic regression
analysis was conducted to identify factors independently associated with OVCF.
The explanatory variables were those with P<0.20 after univariate regression
analysis, and an effect size (ES) greater than 0.5 after a
t-test or greater than 0.3 after a χ2 test. In
addition, the Hosmer-Lemeshow test of the logistic regression model was
conducted to assess the goodness of fit used in this study. In this test, when
P>0.05, the null hypothesis is not rejected, and the model is considered to
be a good fit. Statistical analyses were performed using SPSS version 26.0 (IBM
Japan, Tokyo, Japan), with the significance level set at 5%. Post-hoc power
analysis was conducted using G*Power software version 3.1.9.7
(http://www.gpower.hhu.de/).
RESULTS
Following the exclusion of 44 patients, a total of 177 participants were included in
this study. Of these, 161 did not have OVCF (non-OVCF group) and 16 did (OVCF
group). The number of compression fractures included 13 cases of single compression
fractures, 1 case of two compression fractures, and 2 cases of three compression
fractures. In our study, OVCF was identified at various vertebral levels,
encompassing Th11 to L5, which includes the thoracolumbar transition.
Comparison of Non-OVCF and OVCF Groups
The results of the univariate analysis are presented in Table 1. Patients in the OVCF group were
significantly older than those in the non-OVCF group (74.1 ± 5.8 vs. 69.2 ± 9.9
years, P=0.006) and a significantly higher proportion exhibited muscle atrophy
(50.0% vs. 23.6%, P=0.034). In addition, the proportion of female patients was
higher in the OVCF group than in the non-OVCF group (ES=0.53), and the LLA was
smaller (ES=0.50). These moderate effect sizes were observed despite the
differences failing to reach statistical significance. No significant
differences or effect sizes were observed in the other measurements.
Table 1. Characteristics of patients in non-OVCF and OVCF groups
| Characteristic |
non-OVCF (n=161) |
OVCF (n=16) |
P value |
ES |
1−β |
| Age (years) |
69.2 ± 9.9 |
74.1 ± 5.8 |
0.006 |
0.60 |
0.63 |
| Sex (male/female) |
110 (68.3)/51 (31.7) |
7 (43.8)/9 (56.2) |
0.057 |
0.53 |
1.00 |
| Body mass index
(kg/m2) |
24.6 ± 3.8 |
23.8 ± 2.6 |
0.40 |
0.25 |
0.15 |
| Smoking |
27 (16.8) |
1 (6.3) |
0.47 |
0.28 |
0.96 |
| Diabetes |
39 (24.2) |
2 (12.5) |
0.37 |
0.27 |
0.95 |
| Hemodialysis |
4 (2.5) |
0 |
1.00 |
N/A |
N/A |
| Steroid use |
8 (5.0) |
1 (6.3) |
0.58 |
0.06 |
0.12 |
| ASA score (1 / 2–4) |
23 (14.3)/138 (85.7) |
1 (6.3)/15 (93.7) |
0.70 |
0.23 |
0.86 |
| Bladder bowel dysfunction |
64 (39.8) |
6 (37.5) |
1.00 |
0.05 |
0.09 |
| LLA (degrees) |
21.2 ± 13.5 |
14.6 ± 13.2 |
0.06 |
0.50 |
0.47 |
| Fat infiltration (0 or 1 / 2) |
33 (20.5)/128 (79.5) |
2 (12.5)/14 (87.5) |
0.74 |
0.20 |
0.75 |
| Muscle atrophy |
38 (23.6) |
8 (50.0) |
0.034 |
0.62 |
1.00 |
Data are expressed as mean ± standard deviation or number (percentage).
ASA, American Society of Anesthesiologists.
Based on the results of the univariate analysis, age, muscle atrophy, sex, and
LLA were incorporated into the multivariate logistic regression analysis. Muscle
atrophy (P=0.028; odds ratio, 3.237; 95% confidence interval, 1.138–9.207) was
identified as an independent associated factor of OVCF(Table 2). The Hosmer–Lemeshow test for this model
showed a P value of 0.366, indicating a good fit for the regression model; the
correct classification rate was 91.0%.
Table 2. Multivariate logistic regression analysis to identify factors
associated with OVCF
| Characteristic |
Odds ratio (95% CI) |
P value |
B |
| Muscle atrophy |
3.237 (1.138–9.207) |
0.028 |
1.175 |
| Age |
|
0.061 |
|
| Sex |
|
0.098 |
|
| LLA |
|
0.355 |
|
| Constant |
- |
<0.001 |
−2.733 |
Hosmer–Lemeshow test of the model, P=0.366; correct classification rate,
91.0%. CI, confidence interval; B, regression coefficient.
DISCUSSION
This study aimed to compare preoperative OVCF in patients with LSS. Preoperative
OVCFs were more prevalent in patients with paraspinal muscle atrophy. Furthermore,
the univariate analysis and effect size showed that OVCF tended to be associated
with older age, female sex, and a decreased LLA.
Patients with LSS complicated by OVCF were more likely to experience muscle atrophy
than those without OVCF. This is consistent with the results of previous
studies.13)
Non-union rates of 13.5% at 6 months and 17.5% at 1 year post-injury have been
reported in patients with OVCF who received conservative therapy.28,29) Moreover, evidence
suggests a five-fold increased risk of recurrent compression fractures following an
initial OVCF.30) Hence,
identification of OVCF in the preoperative stage may allow adaptation of treatment
and rehabilitation strategies such as targeted exercises to improve core strength,
balance training, and nutritional interventions to support bone health. Core
exercises may include combinations of draw-in, breathing exercises, and upper and
lower extremity movements with breathing. For balance training, exercises on a
balance board or uneven surfaces could be beneficial for fall prevention and
stability improvement. Particularly in physical therapy, it is necessary to
incorporate preoperative axial elongation and hip disassociation. If these exercises
are challenging in the preoperative stage, it may be necessary to initiate exercises
early in the postoperative period based on the patient’s condition. Furthermore,
modifying lifestyle habits, including eating a well-balanced diet rich in calcium
and vitamin D along with the use of medications to enhance bone density, is crucial
for supporting bone health.
Prior research has also identified spinal kyphosis as a risk factor for compression
fractures.31)
This is consistent with the moderate effect size observed for the LLA in our study.
In addition, a reduction in spinal erector muscle function can lead to conditions
such as low back pain and spinal kyphosis and progress to fat
infiltration.18,32,33) These findings suggest that preoperative OVCF may
increase the risk of qualitative changes in muscle tissue and recurrence of
compression fractures, both before and after surgery. The identification of
preoperative OVCF may be valuable for predicting a decrease in muscle function. To
address these issues, a rehabilitation and treatment plan focusing on muscle atrophy
is crucial. Rehabilitation in patients with muscle atrophy and fat infiltration
commonly involves resistance training,34,35) and it may be necessary for physical therapists and
physicians to collaborate on rehabilitation interventions from the preoperative
stage.
Another significant finding of our study was that both age and sex had moderate
effect sizes. The higher prevalence of preoperative OVCF in older female patients
reflects the age-related decline in bone density and is consistent with previous
studies that have highlighted the significant impact of postmenopausal and
osteoporosis-related factors.4,36,37) Decreased bone density increases the risk of OVCF.
These findings underscore the importance of bone density assessment and osteoporosis
management, particularly in older female patients with LSS. Early intervention and
appropriate preventive measures to address reduced bone density are essential for
reducing the risk of OVCF. Early intervention and preventive measures play a crucial
role in reducing the risk of OVCF. Specific approaches include pharmacological
treatments such as bisphosphonates, selective estrogen receptor modulators, or
parathyroid hormone to improve bone density. Furthermore, addressing bone density
decline in exercise therapy requires incorporating mechanical stress along the
longitudinal axis of the bone. Therefore, exercise programs involving weight-bearing
activities and strength training contribute to bone health. Regular monitoring
through bone density scans allows for treatment adjustments, emphasizing the
importance of a customized and comprehensive approach tailored to individual needs.
These measures not only contribute to the success of the surgery but also facilitate
a smooth postoperative recovery.
Previous studies have shown an increased risk of fractures in patients undergoing
hemodialysis, with at least one spinal fracture observed in 21% of these
patients.38) In
addition, it has been suggested that diabetes39,40) and smoking41) increase the risk of fractures through effects
on bone density. In contrast, our study found no significant differences between the
two groups in terms of hemodialysis, diabetes, or smoking. However, caution should
be exercised when generalizing these findings because our study did not investigate
the relationship between these factors and other aspects of LSS, such as disease
duration or medication history.
This study has several limitations. First, it was a retrospective, single-center
study, which may be subject to inherent bias. Second, the OVCF group consisted of a
relatively small number of participants, potentially limiting the precision of the
comparisons. However, it is worth noting that logistic regression analysis requires
a sample size of at least ten times the number of explanatory variables.42) Although a sample size
calculation was not performed in advance, the number of participants was considered
sufficient for logistic regression analysis. Third, the method used in this study to
determine muscle atrophy has not yet been validated in the paraspinal muscles.
Takayama et al.24)
reported a strong correlation between the distance from the posterior edge of the
paraspinal muscles to the spinous process and the cross-sectional area of the
paraspinal muscles, noting that this distance was approximately 4–9 mm in
individuals aged approximately 70 years, similar to those in our study. If the
posterior edge of the paraspinal muscles is located anterior to the posterior end of
the spinous process, there is a stronger likelihood of muscle atrophy. Therefore,
the method used to identify muscle atrophy in our study may reflect more pronounced
muscle atrophy. The final limitation is that we did not investigate the presence of
pseudarthrosis in compression fractures or the duration of LSS and OVCF. These
aspects may contribute to qualitative changes in lumbar muscles and should be
considered for future research. One of the strengths of this study was the use of
assessment methods shared by physicians and physical therapists.
CONCLUSION
Our study suggests an association between muscle atrophy in the paraspinal erector
spinae muscles and OVCF in preoperative patients with LSS. Older women demonstrated
a higher prevalence of OVCF, and there was a trend of decreased LLA in these
patients. The presence of OVCF in preoperative LSS patients may serve as an
indicator of potential paraspinal muscle involvement, highlighting the importance of
tailored treatment and rehabilitation strategies. However, given the observational
nature of our study, further research is warranted to elucidate the causal
relationships and to assess the impact of OVCF and muscle atrophy on postoperative
outcomes, including quality of life, patient satisfaction, and functional
impairment.
ACKNOWLEDGMENTS
We thank the study participants for their invaluable contributions. Special
appreciation goes to the healthcare professionals and our collaborators for their
support.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- 1. Burger H, Van Daele PL, Grashuis K,
Hofman A, Grobbee DE, Schütte HE, Birkenhäger JC, Pols HA: Vertebral deformities
and functional impairment in men and women. J Bone Miner Res 1997;12:152–157.
PMID:9240738, DOI:10.1359/jbmr.1997.12.1.152
- 2. Silverman S: The clinical consequences of
vertebral compression fracture. Bone 1992;13:S27–S31. PMID:1627411,
DOI:10.1016/8756-3282(92)90193-Z
- 3. Yoshimura N, Muraki S, Oka H, Mabuchi A,
En-Yo Y, Yoshida M, Saika A, Yoshida H, Suzuki T, Yamamoto S, Ishibashi H,
Kawaguchi H, Nakamura K, Akune T: Prevalence of knee osteoarthritis, lumbar
spondylosis, and osteoporosis in Japanese men and women: the research on
osteoarthritis/osteoporosis against disability study. J Bone Miner Metab
2009;27:620–628. PMID:19568689, DOI:10.1007/s00774-009-0080-8
- 4. Horii C, Asai Y, Iidaka T, Muraki S, Oka
H, Tsutsui S, Hashizume H, Yamada H, Yoshida M, Kawaguchi H, Nakamura K, Akune
T, Tanaka S, Yoshimura N: Differences in prevalence and associated factors
between mild and severe vertebral fractures in Japanese men and women: the third
survey of the ROAD study. J Bone Miner Metab 2019;37:844–853. PMID:30607619,
DOI:10.1007/s00774-018-0981-5
- 5. Fujiwara S, Kasagi F, Masunari N, Naito
K, Suzuki G, Fukunaga M: Fracture prediction from bone mineral density in
Japanese men and women. J Bone Miner Res 2003;18:1547–1553. PMID:12929946,
DOI:10.1359/jbmr.2003.18.8.1547
- 6. Kadowaki E, Tamaki J, Iki M, Sato Y,
Chiba Y, Kajita E, Kagamimori S, Kagawa Y, Yoneshima H: Prevalent vertebral
deformity independently increases incident vertebral fracture risk in
middle-aged and elderly Japanese women: the Japanese Population-based
Osteoporosis (JPOS) Cohort Study. Osteoporos Int 2010;21:1513–1522.
PMID:19924494, DOI:10.1007/s00198-009-1113-9
- 7. Pfeifer M, Sinaki M, Geusens P, Boonen S,
Preisinger E, Minne HW, ASBMR Working Group on Musculoskeletal Rehabilitation:
Musculoskeletal rehabilitation in osteoporosis: a review. J Bone Miner Res
2004;19:1208–1214. PMID:15231006, DOI:10.1359/JBMR.040507
- 8. Sinaki M: Exercise for patients with
osteoporosis: management of vertebral compression fractures and trunk
strengthening for fall prevention. PM R 2012;4:882–888. PMID:23174554,
DOI:10.1016/j.pmrj.2012.10.008
- 9. Bennell KL, Matthews B, Greig A, Briggs
A, Kelly A, Sherburn M, Larsen J, Wark J: Effects of an exercise and manual
therapy program on physical impairments, function and quality-of-life in people
with osteoporotic vertebral fracture: a randomised, single-blind controlled
pilot trial. BMC Musculoskelet Disord 2010;11:36. PMID:20163739,
DOI:10.1186/1471-2474-11-36
- 10. Kim JY, Chae SU, Kim GD, Cha MS: Changes
of paraspinal muscles in postmenopausal osteoporotic spinal compression
fractures: magnetic resonance imaging study. J Bone Metab 2013;20:75–81.
PMID:24524061, DOI:10.11005/jbm.2013.20.2.75
- 11. So KY, Kim DH, Choi DH, Kim CY, Kim JS,
Choi YS: The influence of fat infiltration of back extensor muscles on
osteoporotic vertebral fractures. Asian Spine J 2013;7:308–313. PMID:24353848,
DOI:10.4184/asj.2013.7.4.308
- 12. Okuwaki S, Funayama T, Ikumi A, Matsuura
S, Kawamura H, Yamazaki M: Relationship between vertebral instability and the
cross-sectional area of lumbar muscles in postmenopausal acute osteoporotic
vertebral fractures. Spine Surg Relat Res 2022;6:51–57. PMID:35224247,
DOI:10.22603/ssrr.2021-0029
- 13. Fortin M, Lazáry À, Varga PP, Battié MC:
Association between paraspinal muscle morphology, clinical symptoms and
functional status in patients with lumbar spinal stenosis. Eur Spine J
2017;26:2543–2551. PMID:28748488, DOI:10.1007/s00586-017-5228-y
- 14. Xia G, Li X, Shang Y, Fu B, Jiang F, Liu
H, Qiao Y: Correlation between severity of spinal stenosis and multifidus
atrophy in degenerative lumbar spinal stenosis. BMC Musculoskelet Disord
2021;22:536. PMID:34118908, DOI:10.1186/s12891-021-04411-5
- 15. Yarjanian JA, Fetzer A, Yamakawa KS, Tong
HC, Smuck M, Haig A: Correlation of paraspinal atrophy and denervation in back
pain and spinal stenosis relative to asymptomatic controls. PM R 2013;5:39–44.
PMID:23332908, DOI:10.1016/j.pmrj.2012.08.017
- 16. Getzmann JM, Ashouri H, Burgstaller JM,
Valeri F, Winklhofer S, Ulrich NH, Guggenberger R: The effect of paraspinal
fatty muscle infiltration and cumulative lumbar spine degeneration on the
outcome of patients with lumbar spinal canal stenosis: analysis of the Lumbar
Stenosis Outcome Study (LSOS) data. Spine 2023;48:97–106. PMID:36130038,
DOI:10.1097/BRS.0000000000004477
- 17. Zotti MG, Boas FV, Clifton T, Piche M,
Yoon WW, Freeman BJ: Does pre-operative magnetic resonance imaging of the lumbar
multifidus muscle predict clinical outcomes following lumbar spinal
decompression for symptomatic spinal stenosis? Eur Spine J 2017;26:2589–2597.
PMID:28180981, DOI:10.1007/s00586-017-4986-x
- 18. Kjaer P, Bendix T, Sorensen JS, Korsholm
L, Leboeuf-Yde C: Are MRI-defined fat infiltrations in the multifidus muscles
associated with low back pain? BMC Med 2007;5:2. PMID:17254322,
DOI:10.1186/1741-7015-5-2
- 19. Ogon I, Takebayashi T, Takashima H,
Morita T, Yoshimoto M, Terashima Y, Yamashita T: Quantitative analysis
concerning atrophy and fat infiltration of the multifidus muscle with magnetic
resonance spectroscopy in chronic low back pain. Spine Surg Relat Res
2019;3:163–170. PMID:31435570, DOI:10.22603/ssrr.2018-0023
- 20. Liu C, Xue J, Liu J, Ma G, Moro A, Liang
T, Zeng H, Zhang Z, Xu G, Lu Z, Zhan X: Is there a correlation between upper
lumbar disc herniation and multifidus muscle degeneration? A retrospective study
of MRI morphology. BMC Musculoskelet Disord 2021;22:92. PMID:33468108,
DOI:10.1186/s12891-021-03970-x
- 21. Berry DB, Padwal J, Johnson S, Parra CL,
Ward SR, Shahidi B: Methodological considerations in region of interest
definitions for paraspinal muscles in axial MRIs of the lumbar spine. BMC
Musculoskelet Disord 2018;19:135. PMID:29734942,
DOI:10.1186/s12891-018-2059-x
- 22. Suzuki K, Hasebe Y, Yamamoto M, Saita K,
Ogihara S: Inter-rater reliability between two examiners with different
professional roles in the evaluation of fat infiltration in the lumbar
paraspinal muscles using magnetic resonance imaging. J Phys Ther Sci
2021;33:591–595. PMID:34393369, DOI:10.1589/jpts.33.591
- 23. Suzuki K, Hasebe Y, Yamamoto M, Saita K,
Ogihara S: Risk factor analysis for fat infiltration in the lumbar paraspinal
muscles in patients with lumbar degenerative diseases. Geriatr Orthop Surg
Rehabil 2022;13. PMID:35070477, DOI:10.1177/21514593211070688
- 24. Takayama K, Kita T, Nakamura H, Kanematsu
F, Yasunami T, Sakanaka H, Yamano Y: New predictive index for lumbar paraspinal
muscle degeneration associated with aging. Spine 2016;41:E84–E90. PMID:26335668,
DOI:10.1097/BRS.0000000000001154
- 25. Hasebe Y, Suzuki K, Akasaka K, Saita K,
Ogihara S: Inter-examiner reliability in identifying lumbar paraspinal muscle
atrophy by lumbar paraspinal muscle atrophy index, a novel parameter. J Phys
Ther Sci 2022;34:737–740. PMID:36337221,
DOI:10.1589/jpts.34.737
- 26. Ko KJ, Ha GC, Yook YS, Kang SJ: Effects
of 12-week lumbar stabilization exercise and sling exercise on lumbosacral
region angle, lumbar muscle strength, and pain scale of patients with chronic
low back pain. J Phys Ther Sci 2018;30:18–22. PMID:29410558,
DOI:10.1589/jpts.30.18
- 27. Abelin K, Vialle R, Lenoir T,
Thévenin-Lemoine C, Damsin JP, Forin V: The sagittal balance of the spine in
children and adolescents with osteogenesis imperfecta. Eur Spine J
2008;17:1697–1704. PMID:18820952, DOI:10.1007/s00586-008-0793-8
- 28. Tsujio T, Nakamura H, Terai H, Hoshino M,
Namikawa T, Matsumura A, Kato M, Suzuki A, Takayama K, Fukushima W, Kondo K,
Hirota Y, Takaoka K: Characteristic radiographic or magnetic resonance images of
fresh osteoporotic vertebral fractures predicting potential risk for nonunion: a
prospective multicenter study. Spine 2011;36:1229–1235. PMID:21217433,
DOI:10.1097/BRS.0b013e3181f29e8d
- 29. Inose H, Kato T, Ichimura S, Nakamura H,
Hoshino M, Togawa D, Hirano T, Tokuhashi Y, Ohba T, Haro H, Tsuji T, Sato K,
Sasao Y, Takahata M, Otani K, Momoshima S, Yuasa M, Hirai T, Yoshii T, Okawa A:
Risk factors of nonunion after acute osteoporotic vertebral fractures: a
prospective multicenter cohort study. Spine 2020;45:895–902. PMID:32044808,
DOI:10.1097/BRS.0000000000003413
- 30. Lindsay R, Silverman SL, Cooper C, Hanley
DA, Barton I, Broy SB, Licata A, Benhamou L, Geusens P, Flowers K, Stracke H,
Seeman E: Risk of new vertebral fracture in the year following a fracture. JAMA
2001;285:320–323. PMID:11176842, DOI:10.1001/jama.285.3.320
- 31. Zvekic-Svorcan J, Aleksic J, Jankovic T,
Filipovic K, Cvetkovic M, Vuksanovic M, Filipov P: Capture the vertebral
fracture: risk factors as a prediction. J Back Musculoskeletal Rehabil
2019;32:269–276. PMID:30347589, DOI:10.3233/BMR-170898
- 32. Katzman W, Cawthon P, Hicks GE,
Vittinghoff E, Shepherd J, Cauley JA, Harris T, Simonsick EM, Strotmeyer E,
Womack C, Kado DM: Association of spinal muscle composition and prevalence of
hyperkyphosis in healthy community-dwelling older men and women. J Gerontol A
Biol Sci Med Sci 2012;67:191–195. PMID:21878482,
DOI:10.1093/gerona/glr160
- 33. Miki T, Fujita N, Takashima H,
Takebayashi T: Associations between paraspinal muscle morphology, disc
degeneration, and clinical features in patients with lumbar spinal stenosis.
Prog Rehabil Med 2020;5:20200015. PMID:32844128,
DOI:10.2490/prm.20200015
- 34. Welch N, Moran K, Antony J, Richter C,
Marshall B, Coyle J, Falvey E, Franklyn-Miller A: The effects of a
free-weight-based resistance training intervention on pain, squat biomechanics
and MRI-defined lumbar fat infiltration and functional cross-sectional area in
those with chronic low back. BMJ Open Sport Exerc Med 2015;1:e000050.
PMID:27900136, DOI:10.1136/bmjsem-2015-000050
- 35. Ryan A, Harduarsingh-Permaul AS: Effects
of weight loss and exercise on trunk muscle composition in older women. Clin
Interv Aging 2014;9:395–402. PMID:24623974,
DOI:10.2147/CIA.S56662
- 36. Melton JL, III Epidemiology of spinal
osteoporosis. Spine 1997;22:2S–11S. PMID:9431638,
DOI:10.1097/00007632-199712151-00002
- 37. Old JL, Calvert M: Vertebral compression
fractures in the elderly. Am Fam Physician 2004;69:111–116.
PMID:14727827
- 38. Mares J, Ohlidalova K, Opatrna S, Ferda
J: Determinants of prevalent vertebral fractures and progressive bone loss in
long-term hemodialysis patients. J Bone Miner Metab 2009;27:217–223.
PMID:19172222, DOI:10.1007/s00774-008-0030-x
- 39. Yamamoto M, Yamaguchi T, Yamauchi M, Kaji
H, Sugimoto T: Diabetic patients have an increased risk of vertebral fractures
independent of BMD or diabetic complications. J Bone Miner Res 2009;24:702–709.
PMID:19049338, DOI:10.1359/jbmr.081207
- 40. Dede AD, Tournis S, Dontas I, Trovas G:
Type 2 diabetes mellitus and fracture risk. Metabolism 2014;63:1480–1490.
PMID:25284729, DOI:10.1016/j.metabol.2014.09.002
- 41. Ward KD, Klesges RC: A meta-analysis of
the effects of cigarette smoking on bone mineral density. Calcif Tissue Int
2001;68:259–270. PMID:11683532, DOI:10.1007/BF02390832
- 42. Peduzzi P, Concato J, Kemper E, Holford
TR, Feinstein AR: A simulation study of the number of events per variable in
logistic regression analysis. J Clin Epidemiol 1996;49:1373–1379. PMID:8970487,
DOI:10.1016/S0895-4356(96)00236-3
