Abstract
-
INTENTION: A lead in this study means an electric wire connected to an electric circuit at one point. Every part of a lead is equipotential because of the absence of current. This equipotentiality is termed the lead effect. We investigated through the recording of compound muscle action potentials (CMAPs) and electrocardiography (ECG) whether this characteristic nature of the lead is applicable in the human body.
-
METHODS: First, we recorded CMAPs from two male persons connected to each other. Stimulation was delivered to subject 1 alone and subject 2 assumed the role of a lead. CMAPs of subject 1 were recorded from the abductor pollicis brevis muscle with the belly-tendon method. While subject 2 was touching the belly area of subject 1 with his right index finger, the potential was led from the left forearm of subject 2 with a reference on the tendon area of subject 1. When subject 2 was touching the tendon area, the potential was recorded from the belly area of subject 1 with a reference on the left forearm of subject 2. Second, we recorded ECG simultaneously from the two subjects connected to each other by their hands.
-
RESULTS: The recording from the left forearm of subject 2 demonstrated potentials almost identical to the CMAPs of subject 1. This suggested that the potential at the area of subject 1 touched by subject 2 was ‘transmitted’ without significant alteration to the left forearm of subject 2, which was far from the generator of the CMAP. ECG activity of one person was also ‘transmitted’ to another.
-
CONCLUSION: This study suggested that the human body works well as a lead. An area far away from a generator can register some potential through the lead or lead-like structure, such as extremities, and does not necessarily constitute an inactive site.
Translated Abstract
-
【目的】本研究でいうリード線とは一端が電気回路に接続されながら他端はフリーになっている導線のことである.リード線はオームの法則に従って全体が等電位となる.このような等電位化を本研究ではリード線効果と呼ぶ.生体においてリード線効果が成立するか,複合筋活動電位(CMAP)と心電図(ECG)を用いて検証した.
-
【方法】2名の被験者が指や手で相互に接触した状態を作りCMAPとECGの記録を行った.(1)CMAP:被験者1の左正中神経を電気刺激し左短母指外転筋(APB)から被験者1のCMAPを導出した.この際,被験者2は右示指で被験者1の左母指球に触れリード線の役割を担った.被験者2が被験者1のAPB筋腹部に触れているときは,被験者2の左前腕部と被験者1の筋腱部の間で電位を導出した.被験者2が被験者1の筋腱部に触れているときは,被験者1の筋腹部と被験者2の左前腕部間で電位を記録した.さらに被験者2の左右前腕部間の電位記録も行った.(2)ECG:被験者同士が手で相互に接触した状態を作り2名からECGを同時記録した.
-
【結果】(1)CMAP:被験者2の左前腕部から記録された電位は,被験者1から記録されたCMAPとほぼ同振幅同波形であった.被験者2の左右前腕部は等電位となっていた.(2)ECG:被験者1のECGが被験者2へ,被験者2のECGが被験者1へ,ほぼ同振幅同波形で伝達して記録された.
-
【結論と考察】CMAPとECGを用い,生体においてもリード線効果が成立することを確認した.リード線効果を介して,電位発生源から遠く離れた部位からも電位変化が記録された.電位発生源から遠く離れた領域はほぼゼロ電位で電気的に不活性であるとする考え方があるが、本研究は,この考え方が必ずしも正しくない場合があることを示している.
INTRODUCTION
The term lead effect was introduced by Cunningham et al. in the study of somatosensory-evoked far-field potentials,
1
but it is not widely known. Thus, we will first explain what the lead and lead effect are in this study.
The lead in this study means a conductor connected to an electric circuit at one point but not at any other site. There is an electric current flowing in the circuit but no current in the lead because of the lack of a circuit for current flow. An example of a lead is illustrated in Figure 1. The current is flowing in the electric circuit (X-A-Y-Z circuit including a battery), but there is no current in the lead line (A-B-C line). Thus, any site of the lead is equipotential according to Ohm's law irrespective of the resistance in the lead. The potential difference, e.g., between A-Y, is equal to that between B-Y or C-Y, and the potential at site A is ‘transmitted’ or ‘projected’ to site B or C without amplitude reduction. This equipotentiality of a lead or the ‘transmission’ of a potential is referred to as the lead effect in this study.

The principle of the lead effect is not widely considered in the field of electrophysiological recording. However, it is plausible that the potential at a remote area from the electric generator is influenced by the lead effect even in the human body. This idea may be against the generally accepted view that any area far from an electric generator is almost zero in potential and electrically inactive.
In this study, we investigated through the recording of compound muscle action potentials (CMAPs) and electrocardiography (ECG) whether the lead effect functions in the human body, and whether a remote area from the generator is electrically influenced and not necessarily zero in potential.
MATERIALS AND METHODS
CMAPs
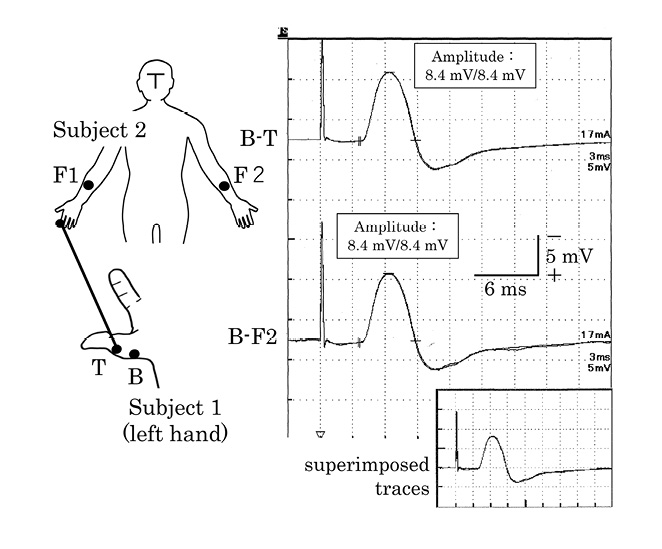
Two male subjects were involved in this study, and both are the authors of this paper (SH and YS). The study was approved by the local ethics committee of Tenri Hospital (No. 1222). We recorded potentials from the two subjects through AC differential amplifiers with a band pass from 3 kHz to 5 Hz. The ground electrode was placed on the left wrist of subject 1. The recording electrodes were disc electrodes of 7 mm in diameter with conductive paste filling their metal parts. The stimulation pulse, 0.2 msec in duration, was delivered to the left median nerve at the wrist of the stimulated person (subject 1) and stimulus intensity was adjusted to evoke the maximum CMAP amplitude of the abductor pollicis brevis muscle (APB). We recorded CMAPs with the standard belly-tendon method from the left APB of subject 1. Electrode B was attached to the belly area and electrode T was attached to the tendon area of subject 1. Electrode F1 was placed on the volar side of the right mid-forearm and electrode F2 was placed on the left of subject 2 (Figure 2).

We recorded the potentials with F2-T and F2-F1 derivations simultaneously with CMAPs of subject 1 while subject 2 was gently touching the region just near the electrode B of subject 1 with his right index finger. There was a small amount of conductive paste slightly extruded from beneath electrode B and subject 2 touched this part of the paste.
Next, subject 2 touched the area just near electrode T instead of electrode B with his right index finger and the potentials were led with the B-F2 derivation simultaneously with CMAPs of subject 1 (Figure 3).
ECG
We recorded ECG activity simultaneously from subjects 1 and 2 (Figures 4 and 5). The electric activity was amplified through AC differential amplifiers with a bandpass of 200 Hz to 0.05 Hz. The ground electrode was placed on the right ankle of subject 1. First, subject 2 directly touched the left hand of subject 1 with his right hand without conductive paste between both hands (Figure 4). ECG activity was recorded from the left forearm of subject 1 (area B) and right upper arm of subject 2 (area D) with a common reference electrode placed on the right forearm of subject 1 (area A). We also recorded a potential difference between the left upper arm (area C) and the left forearm (area B) of subject 1.

Next, subject 2 touched the left hand of subject 1 with his left hand (Figure 5). ECG of subject 1 was obtained with B-A derivation and that of subject 2 with C-D derivation. In addition, we simultaneously recorded ECG activity from the right forearm of subject 2 (C) with the reference at the right forearm of subject 1 (A), as shown in the C-A trace.
RESULTS
CMAPs
As shown in Figure 2, CMAPs recorded with the belly-tendon method (the B-T derivation) and the potentials with the F2-T derivation were the same in amplitude and wave-form, although some small amplitude reductions were noted in the F2-T tracing. There were no discernible potential differences observed with the F2-F1 derivation.
The same result is shown in Figure 3. The potentials recorded with the B-F2 derivation were almost the same as CMAPs recorded from subject 1 in amplitude and wave-form.
ECG potentials
The D-A tracing shown in Figure 4 revealed almost the same ECG activity as that in the B-A trace, although there was contamination by muscle artifacts due to the hands touching. There was no discernible ECG activity with the C-B derivation. Figure 5 shows ECG activity of subject 1 and subject 2 in the upper two traces. ECG activity was reversed in polarity because of the opposite direction of the derivations, i.e., left to right in subject 1 and right to left in subject 2. The third trace (C-A trace) shows combined ECG activity occurring in both subjects, and the activity was almost identical to that recorded from subject 1 or subject 2 shown in the upper two traces.
DISCUSSION
Our CMAP study demonstrated that the potentials recorded from the unstimulated person (subject 2) were almost identical to those recorded from the stimulated person (subject 1), although some small amplitude differences were observed in Figure 2 but not in Figure 3. This may have been due to a difference in the current density between areas B and T. Area B was an active sink and area T a passive source. An active sink is considered higher in current density than a passive source, thus slight dislocation of the touching point near area B can more easily affect the amplitude of the recorded potentials.
When subject 2 was touching the region near area B of subject 1, area F2 of subject 2 became equipotential to area B, and no discernible potential differences were noted between F1 and F2 regions (Figure 2). When subject 2 was touching the region near area T of subject 1, area F2 became equipotential to area T (Figure 3). These suggest that subject 2 functioned as a lead, and the potentials of subject 1 at the area touched by subject 2 were transmitted to area F2 of subject 2 without significant changes in amplitude or wave-form.
The contact resistance should be mentioned. In the setting of Figure 2, subject 1 had one point of contact resistance between the skin at area B and the input of the amplifier: the contact resistance between the skin and the recording electrode at area B. On the other hand, subject 2 had two points of contact resistance: the contact resistance between the skin at area B and the tip of the right index finger of subject 2, and between the skin and the recording electrode at area F2. Thus, the total contact resistance with the F2-T derivation is considered significantly higher than that with the B-T derivation. However, the recorded potentials were almost equal in amplitude, suggesting that the amplitude was not altered irrespective of the contact resistance, as expected from the principle of the lead effect.
However, the difference between the theoretically defined potentials by Ohm’s law and the recorded potentials should be considered. The theoretical potentials will exhibit no amplitude reduction regardless of contact resistance, but the recorded potentials will decrease in amplitude if the contact resistance is so high as to be comparable with the input resistance of the amplifier. The input resistances of our amplifiers were around 200 MΩ, and the contact resistance between the skin of the two subjects was 30-80 kΩ measured by the electrode resistance-meter using 10-Hz AC current (MaP811; Nihon Santeku, Osaka, Japan). The contact resistance was much lower than the input resistance of the amplifiers. Therefore, variation in the contact resistance hardly affected the amplitude of the recorded potentials in this study.
An additional example of transmission of potentials through a lead was observed in ECG, as shown in Figures 4 and 5. In Figure 4, the D-A tracing shows almost the same ECG activity as that recorded from subject 1 with the B-A derivation. This indicates equipotentiality between areas B and D. In addition, the C-B trace shows no discernible potential differences, which indicates equipotentiality between areas B and C. Thus, both of the left upper extremity of subject 1 and the right upper extremity of subject 2 worked together as a lead in this setting, and the potential at area C was transmitted to area D without significant alterations in amplitude or wave-form.
In Figure 5, the combined ECG recording of both subjects is shown in the C-A tracing. The ECG activity of subject 1 was transmitted to subject 2 and vice versa. The entire body of subject 2 was considered to have functioned as a lead for the action potentials of cardiac muscles of subject 1 and vice versa.
Four extremities can be considered to act as leads for ECG activity. Each extremity connecting to the trunk at respective sites reflects the potential at its connecting site to the trunk. As there is little or no current arising from the cardiac muscles within a limb due to their lead-like configuration, each extremity will be almost equipotential, as shown in the C-B trace in Figure 4. On the other hand, the truncal area functions as a circuit for the current. Similar considerations are applicable to the palm and a finger. When the generator such as a conducting nerve impulse is located within the palm of a hand, fingers will act as leads and the tip of a finger will register the potential at the base of the finger.
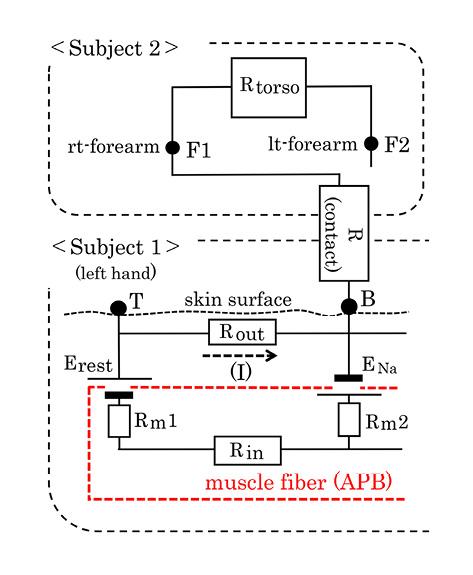
An equivalent electric diagram to explain our CMAP results is illustrated in Figure 6. Subject 2 touching the area just near the electrode B of subject 1 constitutes a lead conductor. There is no current in subject 2 because of the lack of the circuit for current flow. No current produces no potential differences in subject 2 according to Ohm's law and the potential at area B will be transmitted or projected to subject 2, irrespective of the contact resistance. Subject 2 is considered equipotential in every part of the body and to have functioned as a lead. Thus, we confirmed that the lead effect works well in the human body.
The lead effect has been applied to explain why somatosensory-evoked P9 far-field potentials are recordable from the areas at large distances from the active generator site.
1-3
When the action potential is located around the brachial plexus of the stimulated side after stimulation of the median nerve on one side (stimulated side), the P9 far-field potentials are recordable from the head and the upper extremity on the unstimulated side with the knee reference on the unstimulated side.
2, 3
In previous studies, the neck and the unstimulated upper extremity were hypothesized to function as a lead for recording P9 far-field potentials.
2, 3
Yamada et al. reported that P9 far-field potentials were recorded from an unstimulated person connected to the stimulated person while exploring the inactive remote site from the generator.
4
They noted the transmission of P9 far-field potentials from the stimulated person to the unstimulated person.
4
The finding by Yamada et al. is essentially the same as ours in this study. Both studies suggest that even an area far away from an electric generator can be influenced and is not zero in potential because of the transmission of a potential through a lead. In this respect, we consider that the classical view, although not explicitly mentioned, that the potential in a remote area from a generator is nearly zero is not always true.
The zero potential is theoretically defined in infinite medium without boundaries to prevent current flow. This ‘ideal’ medium is not reality in many fields of clinical electrophysiological recording because the human body has lead-like configurations such as limbs, fingers, and a neck. The conductor geometry that may make the current density markedly low or virtually zero in some areas will influence the potential in that area through the lead effect. Therefore, an area far away from a generator is not necessarily zero in potential and does not necessarily constitute an ideal reference site.
C.O.I. DISCLOSURE
The authors have no conflict of interest to disclose.
References
- 1. Cunningham K, Halliday AM, Jones SJ.Simulation of 'stationary' SAP and SEP phenomena by 2-dimensional potential field modelling.Electroencephalogr Clin Neurophysiol1986;65:416-428.
- 2. Hashimoto S, Kawamura J, Segawa Y, et al.Possible model for generation of P9 far-field potentials.Muscle Nerve1992;15:106-110.
- 3. Hashimoto S, Segawa Y.Model of generation of P9 far-field potentials using an electric circuit diagram. In: Kimura J, Shibasaki H, eds.Recent advances in clinical neurophysiology. Amsterdam: Elsevier;1996:251-254.
- 4. Yamada T, Machida M, Oishi M, et al.Stationary negative potentials near the source vs. positive far-field potentials at a distance.Electroencephalogr Clin Neurophysiol1985;60:509-524.