A man in his seventies presented to the Department of General Internal Medicine with a fever persisting for two weeks. He had been well until one month earlier, when he noticed headache and general fatigue. As his symptoms deteriorated with appetite and weight loss, he was admitted to the department. On admission, he appeared ill. His body temperature was 37.7°C, blood pressure was 99/56 mmHg, pulse was 86 beats/min, and oxygen saturation was 97%. No surface lymphadenopathy was noted. The liver and spleen were not palpable. His ECOG performance status (PS) was 3.
His hemoglobin level was 9.1 g/dL, white cell count was 1.47 × 103/μL, and platelet count was 63 × 103/μL. The white cell differential was 25.0% lymphocytes, with 2.0% atypical lymphocytes, 8.0% monocytes, 1.0% basophils, 47.0% segmented neutrophils, 15.0% band neutrophils, and 2.0% metamyelocytes. The level of lactate dehydrogenase (LDH) was 545 U/L, aspartate aminotransferase was 49 U/L, alanine aminotransferase was 37 U/L, alkaline phosphatase was 66 U/L, total bilirubin was 0.5 mg/dL, total protein was 3.7 g/dL, albumin was 1.8 g/dL, globulin was 1.9 g/dL, creatinine was 0.8 mg/dL, uric acid was 2.5 mg/dL, C-reactive protein (CRP) was 11.26 mg/dL, soluble interleukin-2 receptor (sIL-2R) was 10,547 U/mL (reference range, 145 to 519 U/mL), and ferritin was 3,913 ng/mL (reference range, 10 to 260 ng/mL).
18F-fluorodeoxyglucose positron emission tomography combined with computed tomography (18F-FDG-PET/CT) revealed diffuse increased uptake of FDG throughout the bone marrow (BM) space in the central skeleton, with a maximum standardized uptake value (SUVmax) of 6.0 at a thoracic vertebra and 5.5 at the sacrum (Key Figure). The spleen was homogeneously labeled with the tracer with an SUVmax of 10.8 (Key Figure). The liver was not affected, and no FDG-avid lymph nodes were noted.
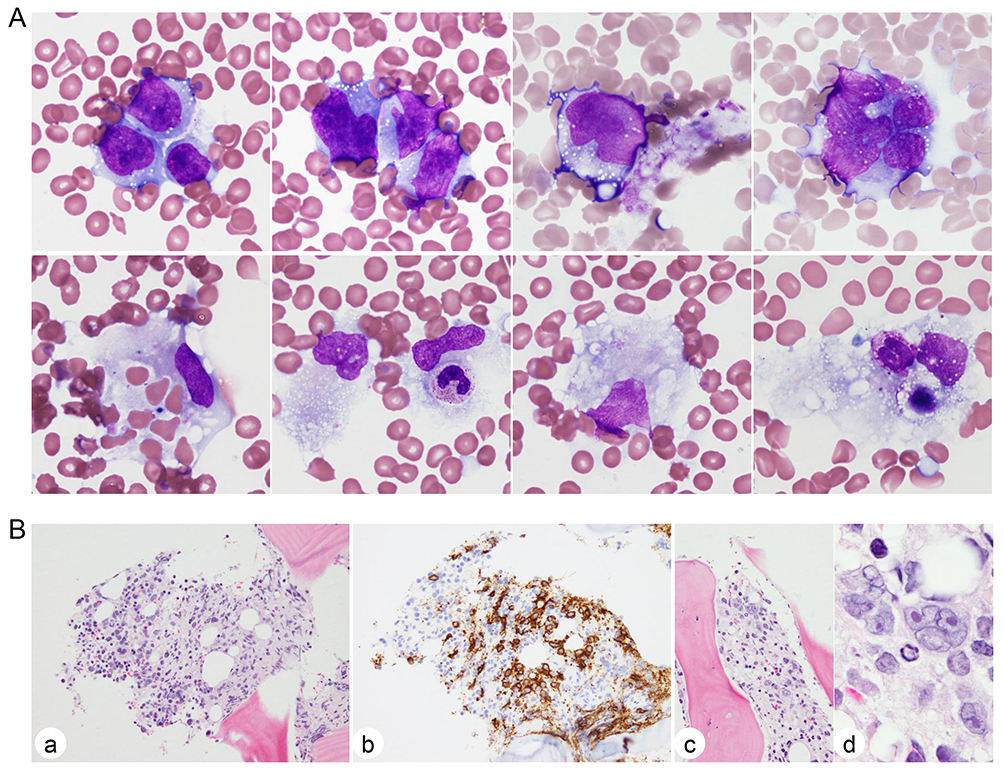
Examination of BM aspirate smears revealed 14.9% lymphoma cells. The cells were medium to large and had irregular nuclei with dispersed chromatin and inconspicuous nucleoli and basophilic cytoplasm containing vacuoles (Figure 1A, top). Some cells were clustered or multinucleated. There were macrophages phagocytizing blood cells (Figure 1A, bottom). The biopsy specimen showed 30% cellularity with infiltration of CD20+ large cells (Figure 1B, a and b). Some cells, including multinucleated cells, formed paratrabecular aggregates (Figure 1B, c and d). Flow cytometry isolated a lymphoma cell fraction exhibiting the CD19+, CD20+, CD5−, CD10−, CD38+, and HLA-DR++ immunophenotype and surface immunoglobulin κ light-chain restriction.
G-banding of metaphase spreads obtained from BM demonstrated t(3;22)(q27;q11.2), leading to the 3q+ and 22q− morphology (Figure 2A). Fluorescence in situ hybridization (FISH) using the BCL6 (Abbott Laboratories, Abbott Park, IL, USA) and IGL (Empire Genomics, Williamsville, NY, USA) break-apart (BA) probes demonstrated that red-labeled telomeric 5′ BCL6 was translocated to der(22)t(3;22) and green-labeled telomeric 3′ IGL was translocated to der(3)t(3;22), indicating the generation of 3′ BCL6::3′ IGL on der(3) and 5′ IGL::5′ BCL6 on der(22) (Figure 2B and C). Additional abnormalities included +X, add(4)(q32), add(6)(q23), del(8)(p21), +9, add(19)(q13), and a double minute chromosome. The complete karyotype was: 48,XY,+8,t(3;22)(q27;q11.2),add(4)(q32),add(6)(p23),del(8)(p21),+9,add(19)(q13),dmin[8]/46,XY[2].

The patient was transferred to the Department of Hematology. He had a hemorrhagic A1-stage gastric ulcer in the body of the stomach and visible vessels were thermo-coagulated under endoscopy. Following the prophase use of prednisolone and rasburicase prophylaxis, we initiated rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP). Although he developed a grade 2 infusion reaction and marked and prolonged cytopenia after the first dose of the treatment, his constitutional symptoms were readily resolved, and appetite gradually recovered with improvement of severe hypoalbuminemia. Tumor lysis syndrome did not occur. The patient completed 6 cycles of R-CHOP and received two additional cycles of high-dose methotrexate for prophylaxis of central nervous system (CNS) involvement. 18F-FDG-PET/CT after treatment confirmed a complete metabolic response.
We proposed the BM, spleen, and liver (MSL)-type diffuse large B-cell lymphoma (DLBCL) that primarily involves BM, the spleen, and liver but lacks involvement of lymph nodes and other extranodal organs,1 and our proposal has been referred to in the literature.2-4 MSL-type DLBCL is best recognized by an 18F-FDG-PET/CT imaging study, in which BM, the spleen, and liver were homogeneously stained by the tracer, even though activities of the spleen and liver are variable among cases.1 The disease affects middle-aged to elderly people and patients often present with “B” symptoms, poor PS, and hepatosplenomegaly. Abnormal laboratory data include pancytopenia and increased levels of LDH, CRP, and sIL-2R. A high level of ferritin may indicate the presence of hemophagocytic syndrome. Diagnostic materials are obtained from BM, demonstrating infiltration of large lymphoma cells of the non-germinal center B-cell phenotype, and cytogenetic abnormalities involving 3q27/BCL6 are often noted.1 The initial treatment response to R-CHOP is favorable, but relapse involving BM and CNS is frequent. Because these clinical and laboratory features of MSL-type DLBCL overlap with those of intravascular large B-cell lymphoma,1,3-5 it remains to be determined whether these two diseases are distinctive conditions. Nevertheless, knowledge of this rare DLBCL subtype showing aggressive clinical behavior can lead to prompt diagnosis and initiation of effective treatment for the disease.
