Abstract
To date, limited drug information is available for the individual optimization of pharmacotherapy. The author attempted multiple evaluations of patient data on factors related to the pharmacokinetics, drug efficacy, and adverse reactions observed in clinical settings. Through the clinical studies, drug information on the individual optimization of pharmacotherapy needed by health professionals including physicians and pharmacists was identified. Major findings were: 1) Cachectic cancer patients had high plasma concentrations of oxycodone via the reduction of CYP3A activity. The metabolic reduction in cachectic cancer patients was potentially related to the elevated serum level of interleukin-6. 2) Dopamine receptor D2 (DRD2) genetic mutations and being female led to poor antiemetic efficacy of the treatment of opioid-induced nausea in prochlorperazine-treated patients. The opioid receptor μ1 (OPRM1) wild genotype in addition to being female and having high plasma concentrations of prochlorperazine increased prolactin secretion during oxycodone treatment. 3) Rheumatoid arthritis patients with a genetic mutation of ATP-binding cassette subfamily B member 1 (ABCB1) had high plasma concentrations of tacrolimus and its 13-O-demethylate. The ABCB1 genetic mutation and associated high plasma concentration of tacrolimus decreased kidney function. 4) Chronic inflammation increased the plasma voriconazole concentration via its poor metabolism, whereas it did not alter the plasma itraconazole concentration. Although co-administration of prednisolone did not affect the plasma concentration of triazole antifungals, it weakly increased voriconazole metabolism. 5) In breastfeeding women, the median milk/plasma concentration ratio of amlodipine was 0.85. However, the observed relative infant dose of amlodipine in most patients was less than 10%.
1. INTRODUCTION
Patient data observed in clinical settings are diverse and complex. Multiple evaluations of patient data including host factors (gender, age, pregnancy, obesity, hepatic and renal function, etc.), environmental factors (concomitant drugs, supplements, food, alcohol consumption, smoking, etc.), disease factors (cancer, cachexia, inflammation, diabetes mellitus, etc.), and genetic factors (genetic variants and epigenetic factors) and their appropriate applications to each patient are needed for the individual optimization of pharmacotherapy1,2) (Fig. 1). To date, limited clinical evidence and drug information are available for the individual optimization of pharmacotherapy. The appropriateness of the clinical evidence and uniform drug information for analyzing diverse and complex individual patient data has not been fully evaluated and validated in clinical situations. The author attempted multiple evaluations of patient factors related to pharmacokinetic disposition, drug efficacy, and adverse reactions observed in clinical settings. Additionally, drug information required by health professionals including physicians and pharmacists on the proper use of pharmaceuticals was obtained in clinical settings. Through the clinical research in collaboration with physicians, the author provided drug information on the individual optimization of pharmacotherapy for health professionals.
Our research has mainly addressed the challenges of cancer pain relief in palliative care,3–8) immunosuppressive therapy for autoimmune diseases,9,10) antimicrobial therapy for serious conditions,11,12) and pharmacotherapy during the perinatal period.13–15) In the present review, the author describes five achievements in recent clinical research on patient factors associated with pharmacokinetics, drug efficacy, and adverse reactions as well as information on the appropriate use of pharmaceuticals. The clinical studies reviewed were conducted in accordance with the principles of the Declaration of Helsinki and its amendments and the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan. The Ethics Committee of Hamamatsu University School of Medicine approved the study protocols.
2. OXYCODONE TREATMENT IN CANCER CACHEXIA7)
Oral oxycodone is converted primarily to inactive noroxycodone by hepatic CYP3A, while CYP2D6 participates in oxycodone conversion to oxymorphone.16) Cancer patients show great variability in oxycodone pharmacokinetics.17) Our previous study revealed that genetic polymorphisms of CYP2D6 and CYP3A5 have no effects on oxycodone pharmacokinetics.3) Generally, most cachectic cancer patients receive opioid analgesics such as morphine and oxycodone for severe cancer pain relief in clinical situations. In cachectic conditions, proinflammatory cytokines such as interleukin (IL)-6, IL-1β, and tumor necrosis factor-α are secreted into the circulating blood.18) The serum levels of proinflammatory cytokines are inversely related to hepatic CYP3A-associated drug elimination.19) Elevated proinflammatory cytokine levels are potentially responsible for a large variation in plasma oxycodone exposure in cancer patients. Cachectic cancer patients occasionally exhibit central nervous system symptoms such as depression, sleepiness, and somnolence.20,21) These symptoms may be related to treatment with central nervous system depressants such as opioid analgesics or to increased proinflammatory cytokines in the blood. Our study investigated the associations between plasma oxycodone, central symptoms, cachexia stage, and serum levels of proinflammatory cytokines in patients with cancer pain.
The observational study (UMIN000020723) was conducted at Hamamatsu University Hospital (Hamamatsu, Japan). Forty-seven Japanese patients receiving oxycodone extended-release tablets (OxyContin, Shionogi & Co., Ltd., Osaka, Japan) twice a day for severe cancer pain were enrolled. The patients had advanced cancer stages according to the tumor-node-metastasis staging classification. The degree of cachexia was classified into three stages, precachexia, cachexia, and refractory cachexia, using clinical symptom-based diagnostic criteria.22) The numbers of patients with precachexia, cachexia, and refractory cachexia were 10, 24, and 13, respectively. The serum level of C-reactive protein (CRP) was significantly higher in cancer patients with refractory cachexia and cachexia than in those with precachexia (p < 0.001 and p < 0.001, respectively). Cancer patients with refractory cachexia and cachexia had higher plasma concentrations of oxycodone than those with precachexia (p < 0.01 and p = 0.04, respectively). Cancer patients with cachexia had a lower noroxycodone metabolic ratio than those with precachexia (p = 0.04). The serum IL-6 level was significantly higher in cancer patients with cachexia and refractory cachexia than in those with precachexia (p < 0.01 and p < 0.01, respectively), although the serum levels of IL-1β and tumor necrosis factor-α did not differ. The serum IL-6 level was positively associated with the plasma oxycodone concentration (r = 0.49, p < 0.01) and negatively associated with the metabolic ratio to noroxycodone (r=−0.35, p = 0.02) (Fig. 2). The plasma oxycodone concentration was not related to the incidence of somnolence. The incidence of somnolence was associated with the cachexia stage and serum IL-6 level (p < 0.01 and p < 0.01, respectively).
In summary, the progression of cancer cachexia increased the plasma oxycodone concentration via the reduction of hepatic CYP3A activity. The metabolic decrease in cancer patients with higher cachexia stage was related to the elevated serum level of IL-6. The symptom of somnolence was observed in cachectic cancer patients with higher plasma oxycodone and higher serum IL-6 levels.
3. CLINICAL RESPONSES TO PROCHLORPERAZINE WITH OXYCODONE TREATMENT6)
Patients treated with opioid analgesics frequently experience adverse drug reactions leading to nonadherence.23,24) Digestive symptoms such as nausea and vomiting are adverse reactions commonly observed early after the introduction of opioid analgesics.24,25) Opioid-induced nausea and vomiting (OINV) are caused by direct stimulation of the chemoreceptor trigger zone, enhancement of vestibular sensitivity, and reduction of gastrointestinal motility.26) Prochlorperazine (PCZ), a dopamine receptor D2 (DRD2) antagonist, is routinely prescribed for OINV prophylaxis in Japan.27) PCZ efficacy and adverse reactions exhibit interindividual variations during treatment with opioid analgesics. In contrast, PCZ enhances prolactin secretion into the circulating blood through the inhibition of dopaminergic systems in the anterior lobe of the pituitary gland.28,29) The hypothalamus controls the serum prolactin level via dopamine secretion.30) Opioid analgesics bind to opioid receptor μ1 (OPRM1) expressed on the hypothalamus and inhibit the dopaminergic systems.31,32) A few significant genetic mutations of DRD2 and OPRM1 have been found in humans.33,34) The associations between DRD2 and OPRM1 genotypes, antiemetic efficacy of PCZ, and serum prolactin elevation have not been fully evaluated during treatment with opioid analgesics. This study investigated the impacts of nongenetic and genetic factors on clinical responses to PCZ in cancer patients receiving oral oxycodone.
This observational study (UMIN000011323) was performed at Hamamatsu University Hospital. A total of 70 Japanese patients treated with oral PCZ tablets (Novamin, Shionogi & Co., Ltd.) three times daily for OINV prophylaxis were enrolled. All received oral PCZ tablets concomitantly with oxycodone tablets for severe cancer pain. The antiemetic efficacy of PCZ for OINV was observed for 14 d after starting PCZ treatment. The oxycodone dose and plasma PCZ concentration were not related to the incidence of OINV. Patients with the DRD2 TaqIA A1A2 + A1A1 alleles and with the DRD2 TaqIB B1B2 + B1B1 alleles had a higher incidence of nausea than those with the A2A2 allele and the B2B2 allele, respectively (Table 1). A higher incidence of vomiting was observed in women than in men. Women had higher serum levels of prolactin than men before and after PCZ administration (p < 0.01 and p < 0.01, respectively). The serum prolactin level was mutually related to plasma PCZ concentration (ρ = 0.24, p = 0.04). Serum levels of prolactin were significantly higher in patients with the OPRM1 118AA allele than in those with the 118AG + 118GG alleles (p < 0.01), while the levels were not associated with the DRD2 genotypes (Fig. 3).
Table 1. Influences of Gender and OPRM1 and DRD2 Genetic Mutations on the Incidences of Opioid-Induced Nausea and Vomiting in Oxycodone and Prochlorperazine-Cotreated Patients
| n | Nausea | Vomiting |
|---|
| n | (%) | p | n | (%) | p |
|---|
| Gender | | | | | | | | |
| Male | 45 | 14 | 31 | 0.31 | 3 | 7 | < 0.01 |
| Female | 25 | 11 | 44 | | 9 | 36 | |
| OPRM1 | | | | | | | | |
| A118G | AA | 25 | 11 | 44 | 0.31 | 5 | 20 | 0.74 |
| AG + GG | 45 | 14 | 31 | | 7 | 16 | |
| DRD2 | | | | | | | | |
| TaqIA | A2/A2 | 29 | 6 | 21 | 0.04 | 2 | 7 | 0.11 |
| A1/A2 + A1/A1 | 41 | 19 | 46 | | 10 | 24 | |
| TaqIB | B2/B2 | 29 | 6 | 21 | 0.04 | 2 | 7 | 0.11 |
| B1/B2 + B1/B1 | 41 | 19 | 46 | | 10 | 24 | |
Our subsequent research including CYP genotype analyses showed that homozygotes for CYP3A5*3 alleles tended to increase the plasma concentration of PCZ and its active metabolite in cancer patients.8) In summary (Fig. 4), being female and having the DRD2 TaqIA and TaqIB mutations attenuated the antiemetic efficacy of PCZ for OINV. Additionally, the OPRM1 wild genotype, in addition to being female and high plasma PCZ exposure, increased the serum prolactin level. These observations indicate that genetic polymorphisms of DRD2 and OPRM1 are responsible for the large interindividual variations in PCZ responses during oxycodone treatment.
4. TACROLIMUS TREATMENT IN RHEUMATOID ARTHRITIS10)
Rheumatoid arthritis (RA) is caused by T cell-mediated inflammation in the synovial membrane of the joints.35) Tacrolimus is a T cell-targeted immunosuppressive drug for RA treatment.36) In organ transplantation, a large variation in blood tacrolimus exposure was observed among recipients.37) Tacrolimus administration occasionally causes blood exposure-associated adverse reactions such as infectious complications, nephrotoxicity, and cardiotoxicity.38) Oral tacrolimus is principally eliminated by the hepatic CYP3A4 and 3A5 metabolism.39) In organ transplant recipients, the homozygotes for the CYP3A5*3 alleles require a lower dose of tacrolimus to reach the target range of blood concentration than the *1 allele carriers.40–43) Tacrolimus is an intestinal P-glycoprotein substrate, and its gene is encoded by the ATP-binding cassette subfamily B member 1 (ABCB1).44) Some studies in organ transplant recipients demonstrated poor associations between the genetic polymorphisms of ABCB1 and blood tacrolimus exposure.40,41,45) There is still controversy about whether ABCB1 genotypes contribute to the pharmacokinetic variability of tacrolimus in organ transplant recipients.42,43) To date, few significant factors determining tacrolimus pharmacokinetics and clinical responses have been found in RA patients. This study investigated the impacts of CYP3A5 and ABCB1 genetic mutations on blood tacrolimus exposure and metabolism in RA patients. It also evaluated the contributions of their genetic polymorphisms to tacrolimus efficacy and kidney function.
This observational study was performed at Hamamatsu University Hospital. Seventy Japanese RA patients initiating oral tacrolimus capsule (Prograf, Astellas Pharma, Tokyo, Japan) treatment once a day in the evening were enrolled. In this study, the incidence of drug resistance or intolerance within 28 d after starting the medication was considered to indicate tacrolimus discontinuation. Sixty-four of 70 RA patients achieved disease remission with tacrolimus dose titration. Patients with the homozygous CYP3A5*3 allele had a higher dose-adjusted blood concentration of tacrolimus than those with the *1 allele (p = 0.03). The 13-O-demethylate metabolic ratio in patients with the homozygous CYP3A5*3 allele was lower than that in patients with the CYP3A5*1 allele (p < 0.01). Higher dose-adjusted blood concentrations of tacrolimus and its 13-O-demethylate were observed in patients with the homozygous ABCB1 3435T allele (p = 0.03 and p = 0.03, respectively). The absolute blood concentration of tacrolimus was inversely correlated with the estimated glomerular filtration rate (eGFR), while it was not associated with the serum CRP level (Fig. 5). The presence of the homozygous ABCB1 3435T allele was associated with a decreased eGFR, while the CYP3A5 genotype was not (Fig. 6). Six RA patients underwent discontinuation within 4 weeks after starting the medication because of a poor response to tacrolimus. A higher incidence of tacrolimus discontinuation was observed in patients carrying the homozygous CYP3A5*1 than carrying the homozygous *3 allele (odds ratio, 61.5, p < 0.01). The ABCB1 genotype was not associated with the incidence of oral tacrolimus discontinuation among patients enrolled.
In summary, CYP3A5*3 was associated with a high blood concentration of tacrolimus due to poor metabolism. In contrast, ABCB1 C3435T raised blood concentrations of tacrolimus and its 13-O-demethylate. These observations indicate that the ABCB1 genetic mutation and its associated higher blood exposure of tacrolimus are involved in the deterioration of kidney function in RA patients.
5. TRIAZOLE ANTIFUNGAL THERAPY UNDER INFLAMMATORY CONDITIONS12)
Voriconazole (VRCZ) is a second-generation broad-spectrum triazole antifungal agent with potent activity against Candida, Cryptococcus, and Aspergillus species.46) VRCZ is mainly used for the treatment of serious and invasive fungal infections, which are occasionally observed during immunosuppressant therapy.47) A nonlinear pharmacokinetic profile of VRCZ was observed in clinical situations.48,49) CYP2C19 and CYP3A4 are important CYP enzymes involved in VRCZ elimination.50) Itraconazole (ITCZ) is also a triazole antifungal agent with potent activity against systemic and superficial mycoses including Candida and Aspergillus species.51) Hepatic CYP3A4 is the major CYP enzyme responsible for ITCZ metabolosm.52) Generally, most immunocompromised patients receiving immunosuppressant therapy also receive a triazole antifungal for prophylaxis or for the treatment of fungal infections, and the alterations in CYP3A4 activity may influence drug elimination.50,53) Immunocompromised patients are at risk for infectious and inflammatory diseases. Inflammation and its associated secretion of proinflammatory cytokines into the circulating blood are related to decreased CYP3A4 expression.19) Additionally, most patients receiving a triazole antifungal concomitantly receive glucocorticoids including prednisolone and methylprednisolone. Glucocorticoids are characterized as potential inducers of CYP enzymes such as CYP2C19 and CYP3A4.54,55) However, few clinical studies have evaluated the impact of concomitant glucocorticoid administration on plasma concentrations of triazole antifungals. This study investigated the pharmacokinetic characteristics of triazole antifungals under the conditions of inflammation and concomitant glucocorticoid administration.
The observational study was performed at Hamamatsu University Hospital. Forty-one Japanese patients receiving VRCZ (Vfend tablet and injection, Pfizer Japan Inc., Tokyo, Japan) and 42 patients receiving ITCZ (Itrizole oral solution, Janssen Pharmaceutical K.K., Tokyo, Japan) for prophylaxis or treatment of an invasive fungal infection were enrolled. Thirty-five patients (10 in the VRCZ treatment group and 25 in the ITCZ treatment group) were co-treated with oral prednisolone (Predonine, Shionogi & Co., Ltd.). No correlation was observed between the plasma concentrations of VRCZ and its N-oxide. The serum level of CRP was positively correlated with the dose-adjusted plasma concentration of VRCZ (r = 0.61, p < 0.01), while it was negatively correlated with the metabolic ratio of VRCZ N-oxide (r=−0.52, p < 0.01) (Fig. 7). In glucocorticoid co-treated patients, a higher daily dose of prednisolone led to a higher metabolic ratio of VRCZ N-oxide (r = 0.72, p = 0.02). A positive correlation was observed between the plasma concentration of ITCZ and its hydroxide (r = 0.89, p < 0.01). There were no associations between plasma ITCZ exposure and metabolism and serum CRP level or prednisolone daily dose.
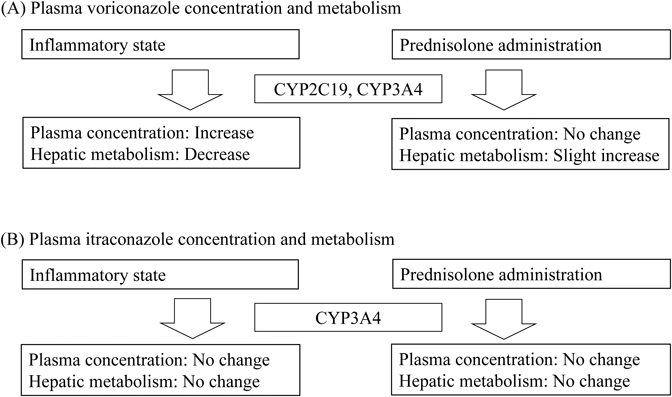
In summary (Fig. 8), chronic inflammation increased the plasma VRCZ concentration via its poor metabolism, whereas it did not alter the plasma ITCZ exposure. Although co-administration of prednisolone did not alter the plasma concentration of triazole antifungals, it weakly increased VRCZ metabolism.
6. AMLODIPINE TRANSFER TO HUMAN BREAST MILK13)
Postpartum women with pregnancy-induced hypertension (PIH) commonly receive long-acting dihydropyridine calcium channel blockers including amlodipine (AML) and extended-release nifedipine.56,57) According to the U.S. National Library of Medicine Drugs and Lactation Database,58) more data on safety are required for the clinical administration of AML to lactating women. However, no adverse reactions in breastfed infants have been reported with the empirical maternal use of AML for PIH while breastfeeding.59–61) Few well-designed clinical studies have been conducted on AML transfer to maternal breast milk. Oral AML is largely absorbed from the intestine, mainly metabolized by hepatic CYP3A4,62) and slowly eliminated with a long plasma half-life.63) Additionally, pregnancy and its related hormones increase hepatic CYP3A4 activity.64,65) However, the plasma disposition of AML has not been fully characterized in lactating hypertensive women.
Determination of the relative infant dose (RID) is one useful method for estimating breastfed infant risk.66) When the RID is less than 10%, the medication is generally considered safe while breastfeeding because of unlikely adverse reactions in infants.66) In one case report, AML in infant plasma samples was not found after breastfeeding for 4 d.59) There have been few clinical reports on the RID of AML. Breastfeeding has many health benefits for both mothers and their infants. Medication to treat hypertension during pregnancy and after delivery is required from the viewpoint of preventing maternal cerebrovascular disorders. We performed a study to determine the plasma disposition of AML and its transfer to maternal breast milk in PIH and estimated the breastfed infant risk in clinical settings.
The observational study (UMIN000013632) was performed at Hamamatsu University Hospital and enrolled 31 Japanese patients starting oral AML besilate tablets (Sawai Pharmaceutical Co., Ltd., Osaka, Japan) for severe PIH after delivery. The AML dose was titrated according to the systolic/diastolic blood pressure goal of less than 140/90 mmHg. The RID (%) was estimated from the following equation: (Cmilk × Vmilk/Dmaternal) × 100%, where Cmilk is the AML concentration in milk, Vmilk the daily volume of milk intake by infants, and Dmaternal the maternal body weight-adjusted AML daily dose.66) The daily volume of milk intake by newborns was assumed to be 150 mL per kg.67) The enrolled women had a median systolic/diastolic blood pressure of 152/94 mmHg before starting the medication and subsequently received a mean maternal dose of 6.0 mg of AML. Maternal blood and milk samples were collected just before dosing on day 10 (interquartile range [IQR], days 8–10) after starting AML. The median plasma concentration of AML was 15.5, while the milk concentration was 11.5 ng/mL (Fig. 9). There were large variations in the AML dose-adjusted plasma (IQR, 135–209 ng/mL per mg/kg) and milk (96.7–205 ng/mL per mg/kg) concentrations in lactating women. The median milk/plasma concentration ratio of AML was 0.85 (IQR, 0.74–1.08) (Fig. 10). The median infant birth weight and estimated AML dose via breast milk were 2170 g and 4.2 µg/kg, respectively. The median RID of AML was 4.2% (IQR, 3.1–7.3%). No circulatory disorders were diagnosed in the breastfed infants during the observation period. In summary, the median milk/plasma concentration ratio of AML was 0.85 in breastfeeding women. However, the observed RID of AML in most newborns was less than 10%.
7. CONCLUSION
Our achievements described in the present review can be summarized as follows.6,7,10,12,13) 1) Cachectic cancer patients exhibited high plasma concentrations of oxycodone via the decrease in CYP3A activity. The metabolic reduction in cachectic cancer patients was potentially related to the elevated serum level of IL-6. 2) DRD2 genetic mutations and being female led to poor antiemetic efficacy for OINV in PCZ-treated patients. The OPRM1 wild genotype, in addition to being female and having high plasma concentration of PCZ, increased prolactin secretion during oxycodone treatment. 3) RA patients with a genetic mutation of ABCB1 had high blood concentrations of tacrolimus and its 13-O-demethylate. The ABCB1 genetic mutation and its related high blood concentration of tacrolimus decreased kidney function. 4) Chronic inflammation increased the plasma VRCZ concentration via its poor metabolism, whereas it did not alter the plasma ITCZ concentration. Although co-administration of prednisolone did not affect the plasma concentration of triazole antifungal agents, it weakly increased VRCZ metabolism. 5) In breastfeeding women, the median milk/plasma concentration ratio of AML was 0.85. However, the observed RID of AML in most newborns was less than 10%.
Acknowledgments
I would like to express my thanks to Dr. Junichi Kawakami, Dr. Yasuaki Mino, Dr. Tatsuya Yagi, Dr. Yoshiaki Takashina, Dr. Takahiro Yamada, Dr. Masaki Tashiro, Dr. Hikaru Sato, Ms. Naoko Kubono, Ms. Satoe Harauchi (Department of Hospital Pharmacy, Hamamatsu University School of Medicine), Dr. Kazunori Ohnishi (Oncology Center, Hamamatsu University School of Medicine), Dr. Noriyoshi Ogawa (Department of Rheumatology, Hamamatsu University School of Medicine), Dr. Hiroaki Itoh (Department of Obstetrics and Gynecology, Hamamatsu University School of Medicine), and Dr. Yoshiyuki Kagawa (Department of Clinical Pharmaceutics and Pharmacy Practice, University of Shizuoka). The studies reviewed were supported by Japan Society for the Promotion of Science (JSPS) KAKENHI Grant numbers JP22926007, JP23790181, JP23926010, JP25928012, JP26460194, and JP26927005.
Conflict of Interest
The author declares no conflict of interest.
Note
This review of the author’s work was written by the author upon receiving the 42nd Sato Memorial Domestic Award.
REFERENCES
- 1) Morse BL, Kim RB. Is personalized medicine a dream or a reality? Crit. Rev. Clin. Lab. Sci., 52, 1–11 (2015).
- 2) Schlender JF, Vozmediano V, Golden AG, Rodriguez M, Samant TS, Lagishetty CV, Eissing T, Schmidt S. Current strategies to streamline pharmacotherapy for older adults. Eur. J. Pharm. Sci., 111, 432–442 (2018).
- 3) Naito T, Takashina Y, Yamamoto K, Tashiro M, Ohnishi K, Kagawa Y, Kawakami J. CYP3A5*3 affects plasma disposition of noroxycodone and dose escalation in cancer patients receiving oxycodone. J. Clin. Pharmacol., 51, 1529–1538 (2011).
- 4) Takashina Y, Naito T, Mino Y, Yagi T, Ohnishi K, Kawakami J. Impact of CYP3A5 and ABCB1 gene polymorphisms on fentanyl pharmacokinetics and clinical responses in cancer patients undergoing conversion to a transdermal system. Drug Metab. Pharmacokinet., 27, 414–421 (2012).
- 5) Yagi T, Naito T, Mino Y, Umemura K, Kawakami J. Impact of concomitant antacid administration on gabapentin plasma exposure and oral bioavailability in healthy adult subjects. Drug Metab. Pharmacokinet., 27, 248–254 (2012).
- 6) Tashiro M, Naito T, Ohnishi K, Kagawa Y, Kawakami J. Impact of genetic and non-genetic factors on clinical responses to prochlorperazine in oxycodone-treated cancer patients. Clin. Chim. Acta, 429, 175–180 (2014).
- 7) Sato H, Naito T, Ishida T, Kawakami J. Relationships between oxycodone pharmacokinetics, central symptoms, and serum interleukin-6 in cachectic cancer patients. Eur. J. Clin. Pharmacol., 72, 1463–1470 (2016).
- 8) Tashiro M, Naito T, Kagawa Y, Kawakami J. Influence of cytochrome P450 genotype on the plasma disposition of prochlorperazine metabolites and their relationships with clinical responses in cancer patients. Ann. Clin. Biochem., 55, 385–393 (2018).
- 9) Mino Y, Naito T, Matsushita T, Otsuka A, Ushiyama T, Ozono S, Hishida A, Kagawa Y, Kawakami J. Comparison of pharmacokinetics of mycophenolic acid and its glucuronide between patients with lupus nephritis and with kidney transplantation. Ther. Drug Monit., 30, 656–661 (2008).
- 10) Naito T, Mino Y, Aoki Y, Hirano K, Shimoyama K, Ogawa N, Kagawa Y, Kawakami J. ABCB1 genetic variant and its associated tacrolimus pharmacokinetics affect renal function in patients with rheumatoid arthritis. Clin. Chim. Acta, 445, 79–84 (2015).
- 11) Yagi T, Naito T, Doi M, Nagura O, Yamada T, Maekawa M, Sato S, Kawakami J. Plasma exposure of free linezolid and its ratio to minimum inhibitory concentration varies in critically ill patients. Int. J. Antimicrob. Agents, 42, 329–334 (2013).
- 12) Naito T, Yamada T, Mino Y, Kawakami J. Impact of inflammation and concomitant glucocorticoid administration on plasma concentration of triazole antifungals in immunocompromised patients. Clin. Chim. Acta, 441, 127–132 (2015).
- 13) Naito T, Kubono N, Deguchi S, Sugihara M, Itoh H, Kanayama N, Kawakami J. Amlodipine passage into breast milk in lactating women with pregnancy-induced hypertension and its estimation of infant risk for breastfeeding. J. Hum. Lact., 31, 301–306 (2015).
- 14) Naito T, Kubono N, Ishida T, Deguchi S, Sugihara M, Itoh H, Kanayama N, Kawakami J. CYP3A activity based on plasma 4β-hydroxycholesterol during the early postpartum period has an effect on the plasma disposition of amlodipine. Drug Metab. Pharmacokinet., 30, 419–424 (2015).
- 15) Harauchi S, Osawa T, Kubono N, Itoh H, Naito T, Kawakami J. Transfer of vaginal chloramphenicol to circulating blood in pregnant women and its relationship with their maternal background and neonatal health. J. Infect. Chemother., 23, 446–451 (2017).
- 16) Lalovic B, Phillips B, Risler LL, Howald W, Shen DD. Quantitative contribution of CYP2D6 and CYP3A to oxycodone metabolism in human liver and intestinal microsomes. Drug Metab. Dispos., 32, 447–454 (2004).
- 17) Leow KP, Smith MT, Williams B, Cramond T. Single-dose and steady-state pharmacokinetics and pharmacodynamics of oxycodone in patients with cancer. Clin. Pharmacol. Ther., 52, 487–495 (1992).
- 18) Tisdale MJ. Molecular pathways leading to cancer cachexia. Physiology, 20, 340–348 (2005).
- 19) Rivory LP, Slaviero KA, Clarke SJ. Hepatic cytochrome P450 3A drug metabolism is reduced in cancer patients who have an acute-phase response. Br. J. Cancer, 87, 277–280 (2002).
- 20) Laird BJ, Scott AC, Colvin LA, McKeon AL, Murray GD, Fearon KC, Fallon MT. Pain, depression, and fatigue as a symptom cluster in advanced cancer. J. Pain Symptom Manage., 42, 1–11 (2011).
- 21) Breitbart W, Alici Y. Evidence-based treatment of delirium in patients with cancer. J. Clin. Oncol., 30, 1206–1214 (2012).
- 22) Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, Jatoi A, Loprinzi C, MacDonald N, Mantovani G, Davis M, Muscaritoli M, Ottery F, Radbruch L, Ravasco P, Walsh D, Wilcock A, Kaasa S, Baracos VE. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol., 12, 489–495 (2011).
- 23) McNicol E, Horowicz-Mehler N, Fisk RA, Bennett K, Gialeli-Goudas M, Chew PW, Lau J, Carr D; Americal Pain Society. Management of opioid side effects in cancer-related and chronic noncancer pain: a systematic review. J. Pain, 4, 231–256 (2003).
- 24) Cherny N, Ripamonti C, Pereira J, Davis C, Fallon M, McQuay H, Mercadante S, Pasternak G, Ventafridda V; Expert Working Group of the European Association of Palliative Care Network. Strategies to manage the adverse effects of oral morphine: an evidence-based report. J. Clin. Oncol., 19, 2542–2554 (2001).
- 25) Cepeda MS, Farrar JT, Baumgarten M, Boston R, Carr DB, Strom BL. Side effects of opioids during short-term administration: effect of age, gender, and race. Clin. Pharmacol. Ther., 74, 102–112 (2003).
- 26) Bhargava KP, Dixit KS, Gupta YK. Enkephalin receptors in the emetic chemoreceptor trigger zone of the dog. Br. J. Pharmacol., 72, 471–475 (1981).
- 27) Ishihara M, Iihara H, Okayasu S, Yasuda K, Matsuura K, Suzui M, Itoh Y. Pharmaceutical interventions facilitate premedication and prevent opioid-induced constipation and emesis in cancer patients. Support. Care Cancer, 18, 1531–1538 (2010).
- 28) Baron JC, Martinot JL, Cambon H, Boulenger JP, Poirier MF, Caillard V, Blin J, Huret JD, Loc’h C, Maziere B. Striatal dopamine receptor occupancy during and following withdrawal from neuroleptic treatment: correlative evaluation by positron emission tomography and plasma prolactin levels. Psychopharmacology (Berl.), 99, 463–472 (1989).
- 29) Ben-Jonathan N. Dopamine: a prolactin-inhibiting hormone. Endocr. Rev., 6, 564–589 (1985).
- 30) Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol. Rev., 80, 1523–1631 (2000).
- 31) Bero LA, Kuhn CM. Differential ontogeny of opioid, dopaminergic and serotonergic regulation of prolactin secretion. J. Pharmacol. Exp. Ther., 240, 825–830 (1987).
- 32) Flores CM, Hulihan-Giblin BA, Hornby PJ, Lumpkin MD, Kellar KJ. Partial characterization of a neurotransmitter pathway regulating the in vivo release of prolactin. Neuroendocrinology, 55, 519–528 (1992).
- 33) Zhang Y, Wang D, Johnson AD, Papp AC, Sadee W. Allelic expression imbalance of human mu opioid receptor (OPRM1) caused by variant A118G. J. Biol. Chem., 280, 32618–32624 (2005).
- 34) Bond C, LaForge KS, Tian M, Melia D, Zhang S, Borg L, Gong J, Schluger J, Strong JA, Leal SM, Tischfield JA, Kreek MJ, Yu L. Single-nucleotide polymorphism in the human mu opioid receptor gene alters beta-endorphin binding and activity: possible implications for opiate addiction. Proc. Natl. Acad. Sci. U.S.A., 95, 9608–9613 (1998).
- 35) Lundy SK, Sarkar S, Tesmer LA, Fox DA. Cells of the synovium in rheumatoid arthritis. T lymphocytes. Arthritis Res. Ther., 9, 202 (2007).
- 36) Fleischmann R, Iqbal I, Stern RL. Tacrolimus in rheumatoid arthritis. Expert Opin. Pharmacother., 7, 91–98 (2006).
- 37) Shuker N, van Gelder T, Hesselink DA. Intra-patient variability in tacrolimus exposure: causes, consequences for clinical management. Transplant. Rev. (Orlando), 29, 78–84 (2015).
- 38) Böttiger Y, Brattström C, Tydén G, Säwe J, Groth CG. Tacrolimus whole blood concentrations correlate closely to side-effects in renal transplant recipients. Br. J. Clin. Pharmacol., 48, 445–448 (1999).
- 39) Gonschior AK, Christians U, Winkler M, Linck A, Baumann J, Sewing KF. Tacrolimus (FK506) metabolite patterns in blood from liver and kidney transplant patients. Clin. Chem., 42, 1426–1432 (1996).
- 40) Hesselink DA, van Schaik RH, van der Heiden IP, van der Werf M, Gregoor PJ, Lindemans J, Weimar W, van Gelder T. Genetic polymorphisms of the CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin. Pharmacol. Ther., 74, 245–254 (2003).
- 41) Haufroid V, Mourad M, Van Kerckhove V, Wawrzyniak J, De Meyer M, Eddour DC, Malaise J, Lison D, Squifflet JP, Wallemacq P. The effect of CYP3A5 and MDR1 (ABCB1) polymorphisms on cyclosporine and tacrolimus dose requirements and trough blood levels in stable renal transplant patients. Pharmacogenetics, 14, 147–154 (2004).
- 42) Zheng H, Webber S, Zeevi A, Schuetz E, Zhang J, Bowman P, Boyle G, Law Y, Miller S, Lamba J, Burckart GJ. Tacrolimus dosing in pediatric heart transplant patients is related to CYP3A5 and MDR1 gene polymorphisms. Am. J. Transplant., 3, 477–483 (2003).
- 43) Macphee IA, Fredericks S, Tai T, Syrris P, Carter ND, Johnston A, Goldberg L, Holt DW. Tacrolimus pharmacogenetics: polymorphisms associated with expression of cytochrome p4503A5 and P-glycoprotein correlate with dose requirement. Transplantation, 74, 1486–1489 (2002).
- 44) Saeki T, Ueda K, Tanigawara Y, Hori R, Komano T. Human P-glycoprotein transports cyclosporin A and FK506. J. Biol. Chem., 268, 6077–6080 (1993).
- 45) Mai I, Perloff ES, Bauer S, Goldammer M, Johne A, Filler G, Budde K, Roots I. MDR1 haplotypes derived from exons 21 and 26 do not affect the steady-state pharmacokinetics of tacrolimus in renal transplant patients. Br. J. Clin. Pharmacol., 58, 548–553 (2004).
- 46) Espinel-Ingroff A, Boyle K, Sheehan DJ. In vitro antifungal activities of voriconazole and reference agents as determined by NCCLS methods: review of the literature. Mycopathologia, 150, 101–115 (2001).
- 47) Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, Kern WV, Marr KA, Ribaud P, Lortholary O, Sylvester R, Rubin RH, Wingard JR, Stark P, Durand C, Caillot D, Thiel E, Chandrasekar PH, Hodges MR, Schlamm HT, Troke PF, de Pauw B; Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med., 347, 408–415 (2002).
- 48) Purkins L, Wood N, Ghahramani P, Greenhalgh K, Allen MJ, Kleinermans D. Pharmacokinetics and safety of voriconazole following intravenous- to oral-dose escalation regimens. Antimicrob. Agents Chemother., 46, 2546–2553 (2002).
- 49) Yamada T, Mino Y, Yagi T, Naito T, Kawakami J. Rapid simultaneous determination of voriconazole and its N-oxide in human plasma using an isocratic high-performance liquid chromatography method and its clinical application. Clin. Biochem., 45, 134–138 (2012).
- 50) Hyland R, Jones BC, Smith DA. Identification of the cytochrome P450 enzymes involved in the N-oxidation of voriconazole. Drug Metab. Dispos., 31, 540–547 (2003).
- 51) Tucker RM, Williams PL, Arathoon EG, Stevens DA. Treatment of mycoses with itraconazole. Ann. N. Y. Acad. Sci., 544 (1 Antifungal Dr), 451–470 (1988).
- 52) Hardin TC, Graybill JR, Fetchick R, Woestenborghs R, Rinaldi MG, Kuhn JG. Pharmacokinetics of itraconazole following oral administration to normal volunteers. Antimicrob. Agents Chemother., 32, 1310–1313 (1988).
- 53) Poirier JM, Cheymol G. Optimisation of itraconazole therapy using target drug concentrations. Clin. Pharmacokinet., 35, 461–473 (1998).
- 54) Chen Y, Ferguson SS, Negishi M, Goldstein JA. Identification of constitutive androstane receptor and glucocorticoid receptor binding sites in the CYP2C19 promoter. Mol. Pharmacol., 64, 316–324 (2003).
- 55) Wright MC, Wang XJ, Pimenta M, Ribeiro V, Paine AJ, Lechner MC. Glucocorticoid receptor-independent transcriptional induction of cytochrome P450 3A1 by metyrapone and its potentiation by glucocorticoid. Mol. Pharmacol., 50, 856–863 (1996).
- 56) Ghanem FA, Movahed A. Use of antihypertensive drugs during pregnancy and lactation. Cardiovasc. Ther., 26, 38–49 (2008).
- 57) Ghuman N, Rheiner J, Tendler BE, White WB. Hypertension in the postpartum woman: clinical update for the hypertension specialist. J. Clin. Hypertens., 11, 726–733 (2009).
- 58) US National Library of Medicine. National Institutes of Health, Health & Human Services. “Drugs and Lactation Database (LactMed) website.”: ‹https://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm.›, accessed September 25, 2018.
- 59) Vasa R, Martha Ramirez M. Amlodipine exposure through breastfeeding in a 32 week preterm newborn. Breastfeed. Med., 8 (Suppl. 1), S15 (2013).
- 60) Ahn HK, Nava-Ocampo AA, Han JY, Choi JS, Chung JH, Yang JH, Koong MK, Park CT. Exposure to amlodipine in the first trimester of pregnancy and during breastfeeding. Hypertens. Pregnancy, 26, 179–187 (2007).
- 61) Szucs KA, Axline SE, Rosenman MB. Maternal membranous glomerulonephritis and successful exclusive breastfeeding. Breastfeed. Med., 5, 123–126 (2010).
- 62) Zhu Y, Wang F, Li Q, Zhu M, Du A, Tang W, Chen W. Amlodipine metabolism in human liver microsomes and roles of CYP3A4/5 in the dihydropyridine dehydrogenation. Drug Metab. Dispos., 42, 245–249 (2014).
- 63) Faulkner JK, McGibney D, Chasseaud LF, Perry JL, Taylor IW. The pharmacokinetics of amlodipine in healthy volunteers after single intravenous and oral doses and after 14 repeated oral doses given once daily. Br. J. Clin. Pharmacol., 22, 21–25 (1986).
- 64) Anderson GD. Using pharmacokinetics to predict the effects of pregnancy and maternal-infant transfer of drugs during lactation. Expert Opin. Drug Metab. Toxicol., 2, 947–960 (2006).
- 65) Papageorgiou I, Grepper S, Unadkat JD. Induction of hepatic CYP3A enzymes by pregnancy-related hormones: studies in human hepatocytes and hepatic cell lines. Drug Metab. Dispos., 41, 281–290 (2013).
- 66) Nice FJ, Luo AC. Medications and breast-feeding: Current concepts. J. Am. Pharm. Assoc., 52, 86–94 (2012).
- 67) Bennet PN. Drugs and Human Lactation. Elsevier, Amsterdam, pp. 325–326 (1988).