Recently, ultrafast cardiac gamma cameras using semi-conductor (cadmium zinc telluride: CZT) detectors have been introduced to clinical imaging practice. Advantages of this system are high spatial resolution1,2
and high energy resolution.3
The former makes either the acquisition time shorter or the radiotracer dose smaller. Even a mixture of both may be possible.4,5
The latter makes a dual isotope study (eg, 99mTc and 123I) using very close photo peaks possible.3
The shorter acquisition time is not only patient-friendly but also beneficial to the facility in terms of study throughput. Besides, it leads to less likelihood of motion artefacts.6
Article p 2727
In addition to these advantages, good diagnostic yield in assessing coronary artery disease (CAD) has been reported as compared with conventional gamma cameras, especially when combined with prone imaging.7,8
However, good diagnostic yield has been proved using 99mTc agents, so the diagnostic performance of CZT camera using thallium-201 had not been elucidated.
Invasive coronary angiography (CAG) is usually cited as the gold standard for detecting CAD; however, CAG is not perfect for assessing ischemia because of its “2-D” nature. Moderate stenoses between 50% and 90% narrowing do not always induce ischemia, and such “stenotic but not ischemic lesions” need not show immediate reperfusion in terms of prognosis.9
Therefore, an ischemia-guided gold standard is necessary to validate diagnostic accuracy in detecting significant CAD.
In this issue of the Journal, Tanaka et al defined a significant stenosis as ≥90% narrowing on visual estimation on invasive CAG or as a lesion of <90% and ≥50% stenosis with a fractional flow reserve (FFR) <0.75.10
This definition is reasonable and superior to a visual estimation of CAG only. These authors demonstrate that CZT SPECT using a smaller dose of thallium-201 with short acquisition time combined with prone imaging yields high diagnostic performance in detecting “significant” CAD. Although SPECT can detect physiologically significant stenosis with good diagnostic accuracy, detecting a perfusion defect in the inferior wall is problematic because of soft tissue attenuation and/or scatter radiation from extra cardiac activity, such as liver and bowel. Thallium-201 has lower photon energy, which is prone to be absorbed by soft tissue such as the diaphragm, and prone imaging improves diaphragmatic attenuation and minimizes scatter radiation by pushing it caudally. Compared with supine imaging alone, Tanaka et al successfully improved the diagnostic accuracy of detecting inferior wall ischemia more than 10% by using prone imaging. In addition, because they used a reasonable and practical definition of significant stenosis, their data are reliable and may promote more widespread use of ultrafast CZT cameras.
There is plenty of diagnostic and prognostic evidence in the field of nuclear cardiology. However, relatively high radiation exposure and long acquisition times are major disadvantages. The ultrafast CZT gamma camera can solve these problems with conventional gamma cameras by the shortening acquisition time and reducing the radiation dose without any cost to image quality5
or diagnostic performance.4,10
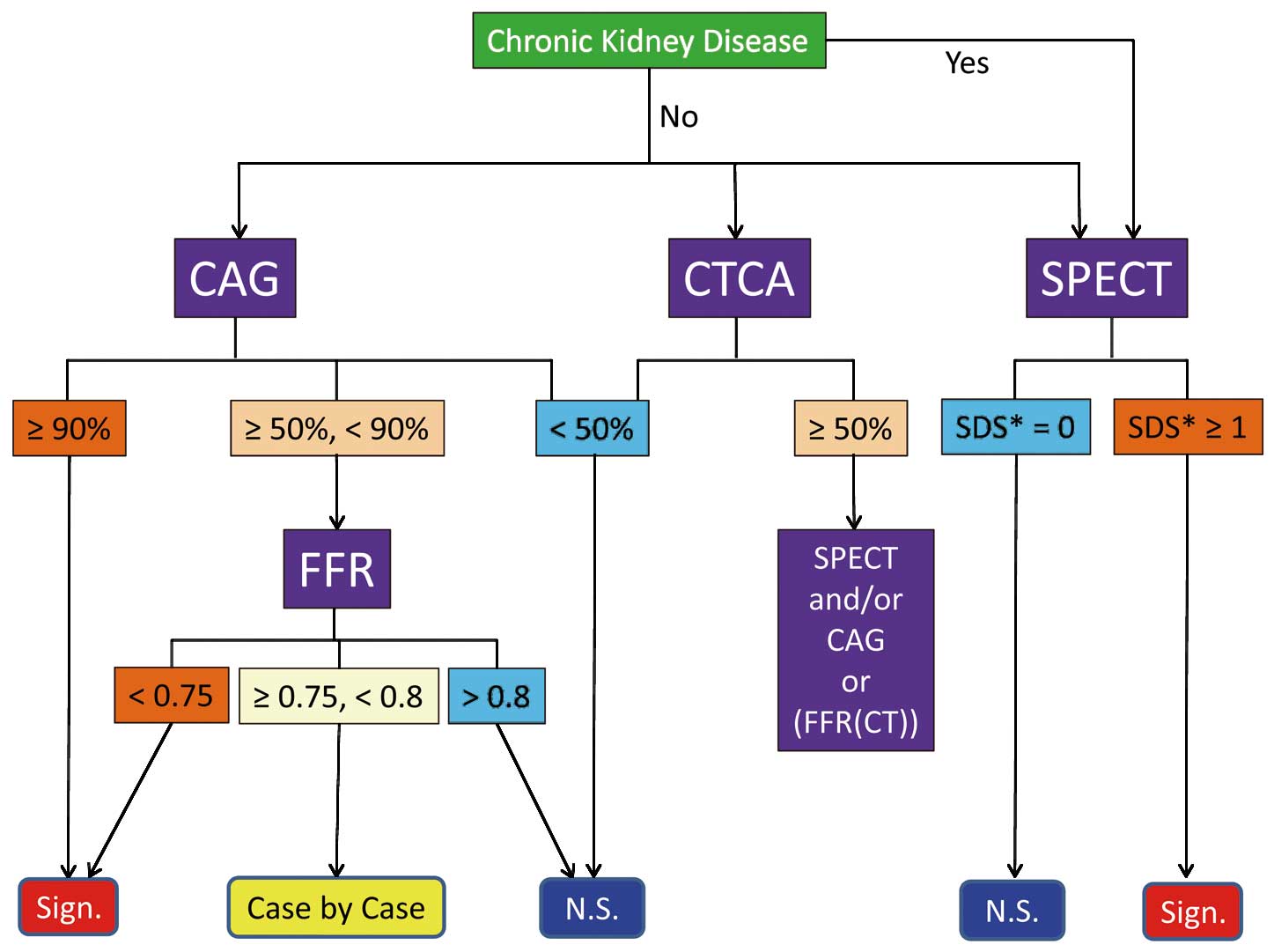
To evaluate CAD, we have to select appropriate the diagnostic tests in the appropriate order, which may depend on the equipment in each facility. Myocardial perfusion SPECT, coronary computed tomography angiography (CTCA), and invasive CAG with FFR measurement play a central role. First of all, when kidney function is impaired, contrast media should not be used, so SPECT would be selected.11,12
If ischemic findings are obtained, such as SDS score ≥1 in each coronary territory, the lesion is a significant stenosis. If kidney function is normal, any test can be selected based on guidelines or the likelihood of CAD and/or clinical risks. If CTCA is selected as a first test, <50% stenosis can be regarded as a non-significant lesion because CTCA has excellent negative predictive value. If the lesion shows ≥50% stenosis, either SPECT or CAG can be selected. If FFR derived from CTCA (FFR(CT)) is available, FFR(CT) can be selected as an alternative test to SPECT and/or CAG.13
The NXT trial demonstrated that FFR(CT) provides high diagnostic accuracy and discrimination of hemodynamically significant CAD.14
For CAG, ≥90% or <50% narrowing on visual estimation are obviously a significant or non-significant flow-limiting stenosis, respectively. For moderate stenosis between 50% and 90% narrowing, FFR is required to determine whether the lesion is physiologically significant or not (Figure).
FFR also has limitations. If a non-culprit diseased vessel with a stenotic lesion supplies collateral flow to a culprit vessel in patients with multivessel disease, FFR may underestimate the culprit lesion and overestimate the non-culprit lesion because of the steal phenomenon. In addition, if left ventricular intramural pressure is elevated, such as in severe aortic stenosis and hypertrophic obstructive cardiomyopathy, FFR may underestimate the lesion. Tanaka et al successfully eliminated this population from their investigation.10
Every diagnostic test has advantages, disadvantages, and limitations. In addition, appropriate-use criteria for multimodality imaging in detecting CAG have been published, and a “choosing wisely campaign” is prevalent in the United States these days. Therefore, we have to have a proper understanding of each diagnostic test in advance and consider appropriateness when selecting the optimal test.

