Abstract
Background:
Active fixation pacing leads with silicon cylinder tips have been used for their safety and flexibility. Measurement of baseline sensing/pacing characteristics before fixation of helix helps to identify the optimal pacing site, but we encountered difficulties in making these measurements despite multiple attempts with the model LPA 1200M lead. To identify the cause and overcome this complication, we compared 4 different retractable active fixation lead models, which enabled baseline sensing/pacing measurements before extension of helix.
Methods and Results:
We immersed 4 different lead tips and rings in a 0.18% saline solution, and measured the lead impedance before and after flushing of air bubble visible inside the lead tip. Before evacuation of the air bubble, the impedance of the model LPA 1200M lead was >4,000 Ω in 8 out of 10 measurements, although that of the other leads was within the measurable range. After evacuation of the air bubble, the lead impedance returned to within the measurable range. There was no prominent change in the impedance of the metal cylinder tip lead.
Conclusions:
Air bubbles may interfere with the measurement of baseline sensing/pacing characteristics before active fixation of pacing leads with cylindrical silicon tips. In the case of high impedance beyond the measurable range before extension of helix, the measurement should be repeated after fixation into the myocardium before suspecting lead dysfunction. (Circ J 2014; 78: 2862–2866)
The choice of permanent fixation site of a retractable screw-in lead is usually based on the sensing and pacing measurements made before extension of the helix. Furthermore, given that the paced QRS morphology can distinguish septal from free wall pacing, pace-mapping before fixation of the lead elsewhere than at the right ventricular apex is most useful and safe.1
We report, however, a case in which, during use of an intact retractable screw-in lead, pace-mapping and measurements of the sensing and pacing characteristics were unable to be done before extension of the helix. We also conducted an experiment to clarify the causes of this phenomenon.
Editorial p 2834
Methods
Case Report
A 59-year-old man who presented with sick sinus syndrome underwent implantation of a dual-chamber pacemaker. After testing the mechanical function and complete retraction of the helix, a Tendril MRITM
LPA 1200M (St. Jude Medical, St. Paul, MN, USA) ventricular pacing lead was inserted from the left subclavian vein, using a 7-F sheath with a hemostatic valve (PI80Z15TSM; Medikit, Tokyo, Japan). We placed the lead tip on the right ventricular mid-septum, using a pre-shaped stylet, and attempted to measure the R-wave amplitude and capture threshold before screwing the helix into the myocardium. The sensing signal, however, was absent and high-output pacing was associated with a >4,000-Ω lead impedance without myocardial capture (Figure 1). This phenomenon persisted despite all trouble-shooting maneuvers and pacing attempts from various endocardial sites. The lead impedance remained unchanged when the helix was extended inside the atrial cavity without screwing it to the wall.

The lead, suspected of being defective, was replaced by another of the same model from a different production lot, although the impedance remained above the upper limit of the measurable range (>4,000 Ω) and the sensing signal continued to be absent. Despite the inability to obtain acceptable baseline measurements, the helix was ultimately screwed into the right ventricular mid-septum, and the lead impedance immediately fell to 1,300 Ω, a 4.9-mV R-wave appeared, the myocardium was captured at a 1.0-V/0.4-ms threshold, and the lead was left in that position.
We examined the originally extracted pacing lead, and immersed its electrodes into saline fluid to test the hypothesis that air bubbles may affect the measurement of lead impedance. The initial lead impedance was >4,000 Ω and an air bubble surrounding the helix was observed inside the silicon sleeve. After evacuation of the air by shaking the lead, the impedance immediately fell to 800 Ω. Additional testing by the manufacturer indicated no lead dysfunction. Based on these reproducible observations among the several production lots of the lead, we hypothesized that an air bubble developing around the helix insulated the conductor in the Tendril MRITM
LPA 1200M lead. To test this hypothesis, we performed an experiment to compare the insulation created by air bubbles among several models of retractable screw-in leads.
Experiment
We compared 4 unused different retractable screw-in leads manufactured by St. Jude Medical, including (1) the Tendril SDXTM
model 1688T; (2) the DurataTM
model 7122; (3) the Tendril STSTM
model 2088; and (4) the Tendril MRITM
model LPA 1200M. The specifications of these 4 leads indicate that the measurements of the sensing/pacing characteristics made before extension of the helix can be used as a baseline from which to choose the site of permanent pacing. We immersed the lead tips and rings, without using introducer sheath, perpendicularly in a 0.18% saline solution based on the standardized Irnich model.2
The lead impedance during bipolar pacing at a 5.0-V/0.5-ms pulse amplitude in the saline solution was measured 10 times in each lead: (experiment A) before extension of the helix; (experiment B) after extension of the helix; (experiment C) after evacuation of the air bubble by shaking the lead while the helix remained extended; and (experiment D) after evacuation of the air bubble and retraction of the helix.
Statistical Analysis
The data are presented as median and interquartile range. The mean lead impedance was compared among the groups using analysis of variance. The Games-Howell test was used for post-hoc multiple comparisons in view of the unequal variances of the groups. P<0.05 was considered significant.
Results
The 4 studied lead tips are shown in
Figure 2A. The metallic tip of the lead model 1688T is used as a distal electrode. The tips of the other leads are silicon cylindrical sleeves covering the helix, used as the distal electrode. The silicon cylinder of the LPA 1200M is larger, with 4 higher protrusions.

The impedance of each lead under various experimental conditions is shown in
Figure 3
and compared in
Table. When the LPA 1200M lead was immersed perpendicularly in 0.18% saline before extension of the helix (experiment A), its impedance was >4,000 Ω in 8 out of 10 attempts. In contrast, the impedance of the other leads remained within the measurable range.
Figure 2B
shows an air bubble occluding the silicon cylinder of the LPA 1200M lead and completely hiding the helix. After the helix was extended inside the saline (experiment B), the impedance of all leads decreased, although some air remained consistently trapped around the helix (Figure 2C) in all of the leads except the 1688T model. After evacuation of the air bubble by shaking the lead (experiment C), the impedance did not change significantly. After retraction of the helix (experiment D), the impedance of each lead increased slightly, although remaining within the measurable range.
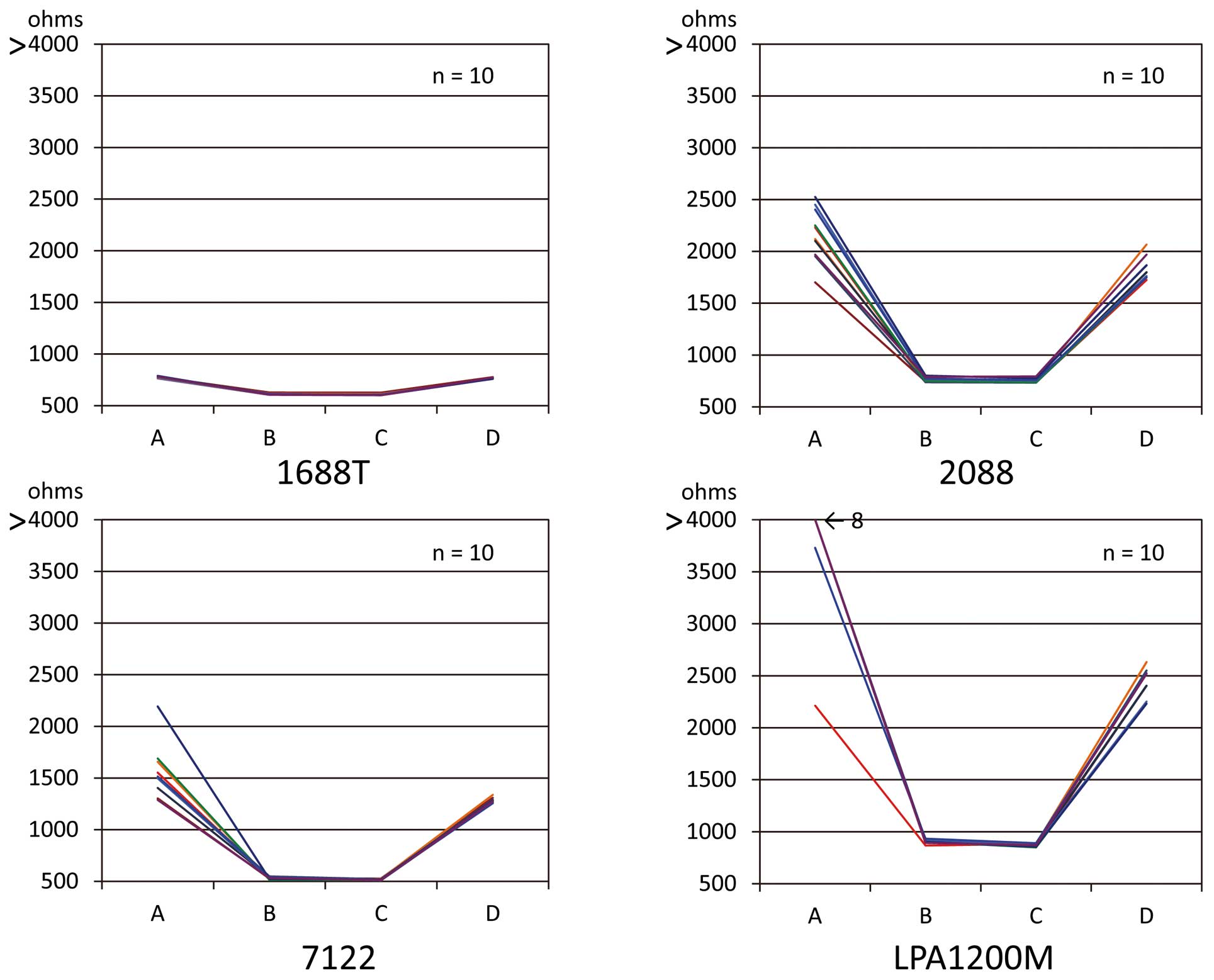
Table.
Lead Impedance vs. Model
| Lead model |
Lead impedance (Ω) |
| A |
B |
C |
D |
| Initial immersion |
Helix extension |
Bubble evacuation |
Helix retraction |
| Tendril 1688T |
781 (778–787)* |
607 (607–615)*,# |
607 (602–609)*,# |
765 (760–773)*,# |
| Durata 7122 |
1,515 (1,379–1,664)* |
529 (523–541)*,# |
519 (513–524)*,# |
1,282 (1,274–1,316)*,# |
| Tendril 2088 |
2,176 (1,965–2,416)* |
757 (746–776)*,# |
744 (737–763)*,# |
1,755 (1,742–1,892)*,# |
| Tendril LPA 1200M |
>4,000 (3,933–>4,000) |
908 (898–917)# |
868 (858–883)# |
2,404 (2,247–2,532)# |
Data given as mean (interquartile range). *P<0.05 compared with LPA 1200M under all conditions; #P<0.05 compared with A.
Discussion
Retractable screw-in leads have been developed to enable pacing from sites other than the right ventricular apex or atrial appendage3
as well as to facilitate their extraction. The helix of the lead, however, is a source of complications, such as pericardial effusion4,5
and pneumothorax.6
Furthermore, repetitive extensions and retractions may jam the helix. Therefore, unnecessary extensions should be avoided and, when choosing a pacing site, the measurements of intrinsic intracardiac electrogram amplitude and capture threshold should preferably be made with the helix retracted, as recommended worldwide.
Transient increase of pacing thresholds immediately after screw-in to the myocardium is a well-known phenomenon and is observed commonly in daily practice. This phenomenon has been thought to be caused by acute myocardial injury by the helix. Kashiwase et al studied the evolution of the pacing threshold measured before, immediately after, and 5 and 10 min after the lead was actively fixed in.7
They found that, when the capture threshold was acceptable before screwing the lead in position, the threshold was satisfactory 5 min after it was fixed in. Therefore, it seems reasonable to choose a pacing site before extension of the helix, and to confirm the quality of the choice by repeating the measurements a few minutes after the lead has been screwed in. Those authors also compared the 1688T and 1488T leads manufactured by St. Jude Medical and the model 5076 lead made by Medtronic, Minneapolis, MN, USA. The evolution of the capture threshold was similar, although the prevalence of threshold >1.5 V before the lead was screwed in was significantly higher with the Medtronic than with the St. Jude Medical leads. These differences may be caused by the difference in the metallic cathodal tips of the 1488T and 1688T leads, vs. the silicon-covered, cathodal cylinder tips of the 5076 helix model. Therefore, the metallic cathodal cylinder of the St. Jude Medical leads contacts readily with the myocardium before being screwed in, compared with the silicon cylinder of the Medtronic leads. These observations are concordant with our own. In the case of the silicon cylinder leads, pre-fixation sensing or pacing can be obtained under the following conditions: (1) pacing electrode in direct contact with the myocardial muscle; or (2) pacing electrode in silicon cylinder close to the myocardium surrounded completely by blood, as a virtual electrode.8
We also made the new observation of a varying high impedance among various silicon cylindrical leads, caused by an air bubble trapped in the cylinder of the lead, before extension of the helix. The silicon cylinder of the lead tip prevents the lead perforations that have been observed with metal lead tips.9
The LPA 1200M has the largest silicon rim and 4 higher protrusions compared with the other leads. These characteristics may facilitate the trapping of an air bubble within the cylinder around the helix. In fact, the air bubble could not be evacuated easily unless the lead was strongly flicked during the present experiment. On the basis of the present experiment, this may be one of the reasons why the air bubble adhered to the lead tip in blood flow during lead placement, or even after extension and retraction within the atrium. As shown in
Figure 2, the LPA 1200M tends to have insulation of the electrode by complete air block in the silicon cylinder compared to the other silicon cylinder leads. In the presence of complete air block, it is impossible to measure sensing and pacing thresholds. Incomplete insulation, however, may cause abnormal elevation of lead impedance or pacing thresholds or sensing insufficiency depending on the degree of air block.
After the air bubble was released, the impedance normalized immediately. The present representative case also showed that sensing, pacing thresholds and lead impedance decreased satisfactorily soon after active fixation of the lead. But moving the lead tip to different locations or extending the helix without screwing it into the myocardium might not be the solution, because these maneuvers might not release the air bubble surrounding the helix. The physician’s manual, published by the manufacturer, cautions that the design of the lead prohibits immersion of the tip in any fluid before lead implantation because the steroid in the tip of the electrode may be prematurely eluted.10
Dipping and flicking the lead tip in a saline solution prior to implantation, however, may evacuate the air bubble. Therefore, provisional fixation of the lead into the myocardium may be the best means of dislodging the air bubble by moving the lead tip and helix inside the atrial or ventricular chamber, or by means of dipping the lead tip in a saline solution to evacuate the air bubble when satisfactory measurements are unable to be obtained.
Study Limitations
First, the present experiment of placing lead tips in saline solution at a perpendicular angle, was conducted, based on the experience described in the case report, to investigate the possibility of extremely high lead impedance caused by air bubble entrapment among the different designs of retractable screw-in leads. The clinical incidence of sensing and pacing interference caused by air bubble entrapment during lead placement, however, is still unknown. Second, all leads used in the present experiment had a specific normal range of lead impedance according to their materials and/or design, therefore it would be best to use the normal range of lead impedance when comparing particular leads, but unfortunately the normal range of impedance before extension of the helix has not been documented as yet. Third, the relationship between degree of insulation by air bubble and sensing and pacing thresholds could not be elucidated using this experimental system.
Conclusions
Reliable measurements of the baseline sensing/pacing characteristics and lead impedance before the screwing in of a retractable pacing lead with a silicon cylinder tip may not represent the optimal pacing site. Air bubble in the cylinder around the helix is presumed to impede the electrical conduction between the helix and the myocardium, and may cause extremely high lead impedance. In the case of unsatisfactory baseline measurements with a high impedance before extension of the helix, an attempt to screw the lead into the myocardium should be made before suspecting a malfunction, especially when using a Tendril MRITM
model LPA 1200M.
Acknowledgments
Funding Source: This study was supported by unrestricted institutional funds.
Disclosure
The authors have no potential conflict of interest to disclose.
References
- 1.
McGavigan AD, Roberts-Thomson KC, Hillock RJ, Stevenson IH, Mond HG. Right ventricular outflow tract pacing: Radiographic and electrocardiographic correlates of lead position. Pacing Clin Electrophysiol 2006; 29: 1063–1068.
- 2.
Irnich W. Interference in pacemakers. Pacing Clin Electrophysiol 1984; 7(6Pt1): 1021–1048.
- 3.
Minamiguchi H, Abe H, Kohno R, Oginosawa Y, Tamura M, Takeuchi M, et al. Incidence and characteristics of far-field R-wave sensing in low right atrial septum pacing. Circ J 2012; 76: 598–606.
- 4.
Antonelli D, Feldman A, Schliamser JE, Militianu A, Turgeman Y. Acute pericardial tamponade due to screw-in atrial lead heart perforation. Europace 2012; 14: 453–455.
- 5.
Ohlow MA, Lauer B, Brunelli M, Geller JC. Incidence and predictors of pericardial effusion after permanent heart rhythm device implantation: Prospective evaluation of 968 consecutive patients. Circ J 2013; 77: 975–981.
- 6.
Oginosawa Y, Abe H, Nakashima Y. Right pneumothorax resulting from an endocardial screw-in atrial lead in an implantable cardioverter defibrillator system. Pacing Clin Electrophysiol 2002; 25: 1278–1279.
- 7.
Kashiwase K, Kobayashi H, Hirata A, Wada M, Nakanishi H, Ueda Y. Acute changes in pacing threshold after lead implantation: Comparison between retractable and sweet-tip active-fixation leads. Int Heart J 2012; 53: 108–112.
- 8.
Furman S. Basic concepts. In: Furman S, Hayes DL, Holmes DR, editors. A practice of cardiac pacing, 3rd edn. New York: Futura Publishing, 1993; 29–88.
- 9.
Danik SB, Mansour M, Heist EK, Ellinor P, Milan D, Singh J, et al. Timing of delayed perforation with the St. Jude Riata lead: A single-center experience and a review of the literature. Heart Rhythm 2008; 5: 1667–1672.
- 10.
Tendril MRI Model LPA1200M User’s Manual. http://professional-intl.sjm.com/resources/ (accessed June 30, 2014).

