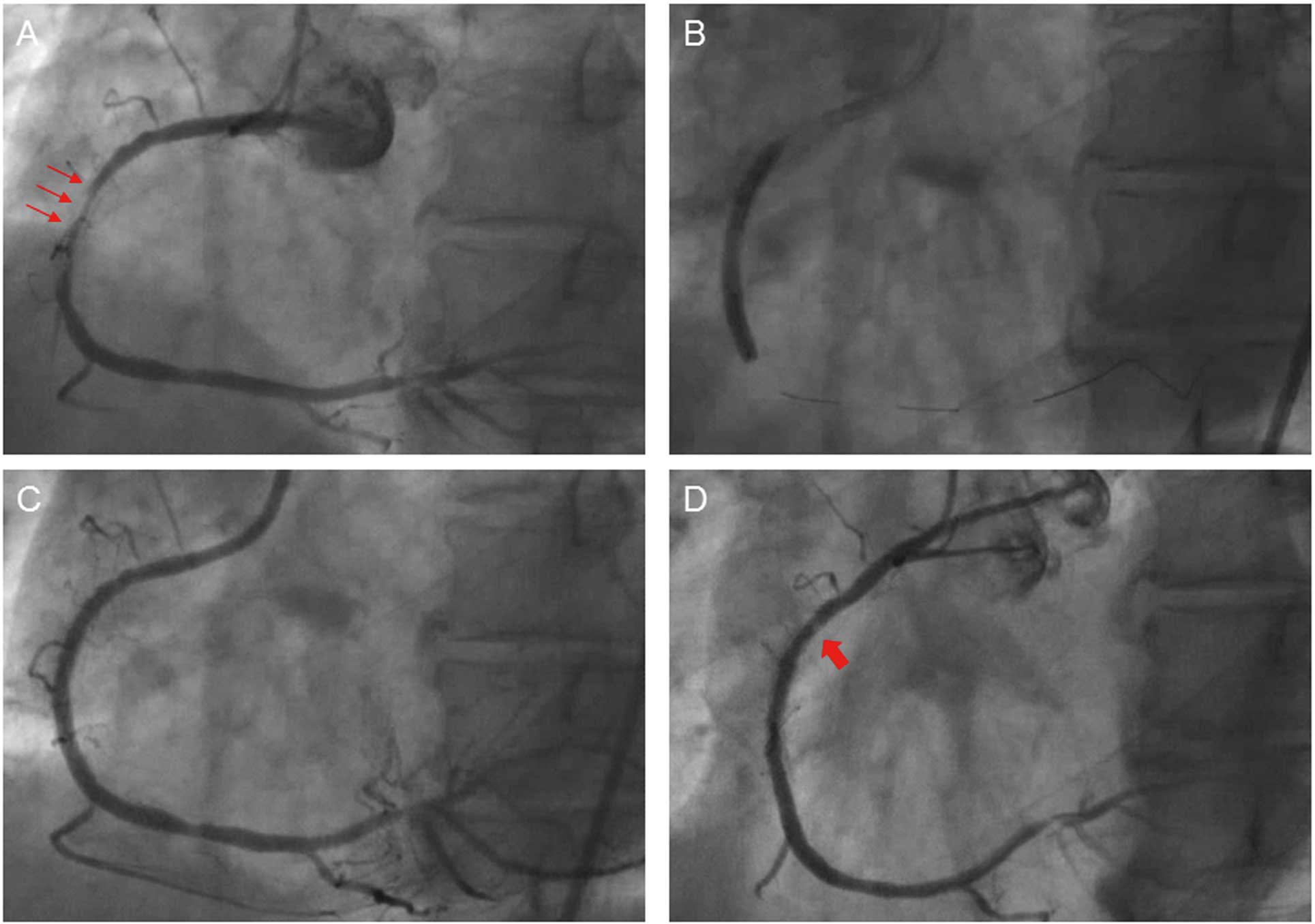
A 70-year-old man received a 3.0×33-mm sirolimus-eluting stent (SES) implant for in-stent restenosis of a bare-metal stent (Figures 1A–C). Coronary angiography was carried out 94 months later, which showed translucency at the proximal edge of the SES (Figure 1D). Coronary angioscopy (CAS) demonstrated presence of light yellow material with an irregular surface protruding into the lumen (Figure 2A). It was also noted on optical frequency domain imaging (OFDI) that the protruding material showed some attenuation in depth and it was partially covered by a surface layer with a clear border (Figure 2C). Judging from these findings, we diagnosed this material as representing a calcified nodule. Follow-up catheterization was performed again 105 months after SES implantation. CAS demonstrated red thrombus layered over the calcified nodule (Figure 2B;
Movie S1). Lumen area narrowing was detected at the site of the calcified nodule on OFDI (3.47 mm2→3.04 mm2;
Figure 2D).

To the best of our knowledge, this is the first case of calcified nodule rupture in vivo. One of the underlying mechanisms of arterial calcification is inflammation,1
and a previous study showed that inflammation may be observed on pathology after SES implantation.2
The present calcified nodule may have occurred in response to the inflammation caused by SES implantation. It is possible that the material was organized thrombus but, because dynamic intra-vascular status can be visualized on CAS,3–5
judging from the angioscopy, the mobility was poor compared with the organized thrombus. Therefore, this material was identified as a calcified nodule. Hao et al reported on the histopathology of calcified nodule and found that in addition to calcification, neovascularization within a myxomatous matrix was observed.6
Libby observed that intraplaque neovascular channels are prone to rupture, and stated that some episodes of sudden plaque expansion may result from hemorrhage due to such microvessel rupture.7
In the present case, intraplaque hemorrhage within the calcified nodule followed by lumen narrowing, was suggested by the red thrombus layered over the calcified nodule. Therefore, we speculated that this phenomenon may be due to rupture of calcified nodule. Calcified nodule can be one of the factors associated with very late stent thrombosis, especially after drug-eluting stent implantation. Furthermore, given that silent plaque rupture causes stenosis,8
calcified nodule can become a cause of late catch-up. We should provide close follow-up for patients with calcified nodule.
Disclosures
Name of Grant: None.
Supplementary Files
Supplementary File 1
Movie S1.
Coronary angioscopy of the calcified nodule 105 months after sirolimus-eluting stent implantation, showing red thrombus layered over the calcified nodule.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-15-0228
References
- 1.
New SE, Aikawa E. Cardiovascular calcification: An inflammatory disease. Circ J 2011; 75: 1305–1313.
- 2.
Nakazawa G, Finn AV, Vorpahl M, Ladich ER, Kolodgie FD, Virmani R. Coronary responses and differential mechanisms of late stent thrombosis attributed to first-generation sirolimus- and paclitaxel-eluting stents. J Am Coll Cardiol 2011; 57: 390–398.
- 3.
den Heijer P, Foley DP, Hillege HL, Lablanche JM, van Dijk RB, Franzen D, et al. The ‘Ermenonville’ classification of observations at coronary angioscopy: Evaluation of intra- and inter-observer agreement: European working group on coronary angioscopy. Eur Heart J 1994; 15: 815–822.
- 4.
Ichikawa M, Takei Y, Hamasaki T, Kijima Y. Characterization of patients with angioscopically-detected in-stent mural thrombi. Circ J 2014; 79: 85–90.
- 5.
Akazawa Y, Matsuo K, Ueda Y, Nishio M, Hirata A, Asai M, et al. Atherosclerotic change at one year after implantation of Endeavor zotarolimus-eluting stent vs. everolimus-eluting stent. Circ J 2014; 78: 1428–1436.
- 6.
Hao H, Fujii K, Shibuya M, Imanaka T, Kawakami R, Hatakeyama K, et al. Different findings in a calcified nodule between histology and intravascular imaging such as intravascular ultrasound, optical coherence tomography, and coronary angioscopy. JACC Cardiovasc Interv 2014; 7: 937–938.
- 7.
Libby P. Molecular bases of the acute coronary syndromes. Circulation 1995; 91: 2844–2850.
- 8.
Burke AP, Kolodgie FD, Farb A, Weber DK, Malcom GT, Smialek J, et al. Healed plaque ruptures and sudden coronary death: Evidence that subclinical rupture has a role in plaque progression. Circulation 2001; 103: 934–940.
