Abstract
Background:
In Asian patients in RE-LY, dabigatran etexilate (DE) was as effective as warfarin, with a significantly lower bleeding risk. We evaluated the relationship between baseline renal function or CHADS2
score and efficacy or safety outcomes in these patients.
Methods and Results:
Asian patients (n=2,782) were categorized according to baseline renal function or CHADS2
score, and efficacy and safety outcomes were analyzed for DE (110 mg and 150 mg b.i.d.) vs. warfarin. There was an increase in the rates of stroke/systemic embolism and major bleeding with worsening renal function and CHADS2
score. For stroke/systemic embolism (primary efficacy endpoint), there was no treatment interaction for dabigatran at either 110 or 150 mg b.i.d. compared with warfarin related to patients’ baseline renal function (Pinteraction=0.56 for DE 110 mg and 0.62 for DE 150 mg vs. warfarin) or CHADS2
score (Pinteraction=0.68 for DE 110 mg and 0.31 for DE 150 mg vs. warfarin). For major bleeding, there was no treatment interaction by creatinine clearance category observed for either dose (Pinteraction=0.60 and 0.62 for DE 110 mg and DE 150 mg, respectively). Baseline CHADS2
score had no significant effect on bleeding event rates with DE vs. warfarin.
Conclusions:
Bleeding and stroke rates in Asian patients varied according to renal function and CHADS2
score, but the relative benefits of DE over warfarin were preserved when analyzed by subcategories. (Circ J 2015; 79: 2138–2147)
Atrial fibrillation (AF) is one of the most common cardiac arrhythmias encountered worldwide.1
The overall prevalence of AF is less than 1%, but in people aged ≥80 years, the rate is considerably higher.1
As life expectancy in Asian countries is expected to increase over the next 30 years, there will be a significant rise in patients with AF, especially in countries like Japan, which has a high proportion of elderly citizens.1,2
Editorial p 2098
The Japanese guidelines for the pharmacological management of AF recommend an international normalized ratio (INR) of 2.0–3.0 (similar to the international guidelines) for patients at moderate risk of stroke, and a lower INR of 1.6–2.6 in patients >70 years of age.3
Accordingly, in a prospective, observational study of patients with AF in Japan, 66.0% of patients on warfarin had an INR between 1.6 and 2.6.4
However, the lower target levels were maintained irrespective of patient age, showing only limited adherence to treatment guidelines in clinical practice.1
The updated Japanese guidelines revised in 2013 also highlight the importance of CHADS2
score in the selection of oral anticoagulation therapy.5
Both renal function and CHADS2
score have previously been shown to be predictors of stroke and bleeding events in AF populations.6,7
Dabigatran etexilate (DE), a non-vitamin K antagonist oral anticoagulant (NOAC), is approved for the reduction of stroke risk in non-valvular AF patients in more than 100 countries around the world,8
including the United States, the European Union, Canada, and Japan. In RE-LY (Randomized Evaluation of Long Term Anticoagulant Therapy), a multinational trial conducted in 18,113 patients with non-valvular AF and at least 1 risk factor for stroke, DE 110 mg twice daily (b.i.d.) was non-inferior to warfarin in stroke reduction and superior with regard to major bleeding; DE 150 mg b.i.d. was superior in stroke reduction and non-inferior for major bleeding reduction vs. warfarin.9
A subgroup analysis of RE-LY showed that major, intracranial and total bleeding rates in Asians were significantly higher with warfarin than with both doses of DE (ie, 110 mg and 150 mg).10
Furthermore, the use of NOACs, including DE, strongly reduces the incidence of intracranial bleeding when compared with warfarin in Asian patients.11
As a result, NOACs would appear to be the best option for stroke prevention when treating Asian patients, including Japanese, with non-valvular AF.11
Risk factors for bleeding events, including the CHADS2
score and renal function, should therefore be taken into consideration when managing Asian patients.
We conducted an analysis of Asian patients in RE-LY to evaluate the relationship between baseline renal function or CHADS2
score category and efficacy or safety outcomes. The primary goal of this analysis was to explore if there was consistency in effect for differing renal function and CHADS2
score categories with the overall results of RE-LY Asia. The results of the current analysis are expected to help guide treatment with DE and make improved dosing choices according to the patient’s characteristics.
Methods
Main Outcome Definitions
The study design of the RE-LY has been published previously.9
In the study, 2 fixed doses (110 or 150 mg b.i.d.) of DE administered in a blinded manner were compared with open-label warfarin (target INR of 2.0–3.0) in patients with AF. The Asian countries included in the trial were China, Hong Kong, Japan, South Korea, Taiwan, India, Malaysia, the Philippines, Singapore, and Thailand. The Asian subanalysis of RE-LY involved 2,782 patients.10
The primary efficacy endpoint was the occurrence of stroke or systemic embolism.10
Stroke was classified as ischemic or hemorrhagic. Major bleeding was defined according to International Society on Thrombosis and Haemostasis criteria: a reduction in the hemoglobin level of ≥20 g/L, transfusion of ≥2 units of blood, or symptomatic bleeding in a critical area or organ. Life-threatening bleeding, a subcategory of major bleeding, consisted of fatal bleeding, symptomatic intracranial hemorrhage, bleeding with a decrease in the hemoglobin level of ≥50 g/L, or bleeding requiring transfusion of ≥4 units of blood or inotropic agents or necessitating surgery. All other bleeding was considered as minor bleeding, which was reported by the investigators. All major bleeds were adjudicated blindly by ≥2 adjudicators.10
Statistical Analysis
The study outcomes of the RE-LY Asian analysis have been published previously.10
Here, we reanalyzed the Asian data according to baseline renal function or CHADS2
score. Cox regression models were used to calculate hazard ratios (HRs), confidence intervals (CIs), and P values. For analyses on creatinine clearance (CrCl) within the Asian population, the model contained terms for treatment, CrCl categories (<50 ml/min, 50 to <80 ml/min, ≥80 ml/min), and the interaction. CrCl was calculated according to Cockcroft-Gault. Separate models were used to derive results for DE 110 mg b.i.d. vs. warfarin, and DE 150 mg b.i.d. vs. warfarin. For analyses by CHADS2
within the Asian population, the model again contained terms for treatment, CHADS2
score category (0–1, 2, 3–6) and the interaction.
As this was a post-hoc subgroup analysis with limited sample size, all P values should be viewed cautiously. All analyses were performed using SAS software, version 9.2 or higher (SAS Institute, Cary, NC, USA).
Results
Patients Disposition and Baseline Characteristics
There were 2,782 Asian patients from 10 Asian countries (15% of all RE-LY patients) in this RE-LY subanalysis population. Asian patients had a mean age of 68 years and a mean body weight of 66.3 kg. The baseline demographic characteristics of the patients randomized to the 3 treatment groups (DE 110 mg b.i.d., DE 150 mg b.i.d., or warfarin) were comparable (Table 1).
Table 1.
Baseline Demographic Characteristics of RE-LY Asian Patients
| |
DE 110 mg b.i.d.
(n=923) |
DE 150 mg b.i.d.
(n=933) |
Warfarin
(n=926) |
Total Asian patients10
(n=2,782) |
| Age, years; mean (SD) |
67.9 (9.5) |
67.6 (9.9) |
68.5 (9.9) |
68.0 (9.8) |
| <65, n (%) |
247 (26.8) |
270 (29.0) |
229 (24.8) |
746 (26.8) |
| 65–74, n (%) |
436 (47.2) |
420 (45.0) |
417 (45.0) |
1,273 (45.8) |
| ≥75, n (%) |
240 (26.0) |
243 (26.0) |
280 (30.2) |
763 (27.4) |
| Weight (kg), mean (SD) |
66.1 (12.6) |
66.7 (12.7) |
66.2 (12.9) |
66.3 (12.8) |
| Seated blood pressure, mmHg |
| Systolic, mean (SD) |
128.9 (17.2) |
129.3 (17.6) |
128.8 (17.7) |
129.0 (17.5) |
| Diastolic, mean (SD) |
77.5 (10.6) |
77.5 (11.0) |
77.6 (10.6) |
77.6 (10.7) |
| Sex |
| Male (n, %) |
583 (63.2) |
613 (65.7) |
579 (62.5) |
1,775 (63.8) |
| Type of AF |
| Persistent, n (%) |
388 (42.0) |
378 (40.5) |
385 (41.6) |
1,151 (41.4) |
| Paroxysmal, n (%) |
252 (27.3) |
252 (27.0) |
266 (28.7) |
770 (27.7) |
| Permanent, n (%) |
283 (30.7) |
303 (32.5) |
275 (29.7) |
861 (30.9) |
| Creatinine clearance, ml/min |
| Mean, SD |
65.4 (22.3) |
65.7 (22.3) |
64.8 (21.8) |
65.3 (22.1) |
| <50, n (%) |
256 (27.7) |
240 (25.8) |
244 (26.3) |
740 (26.6) |
| 50–<80, n (%) |
457 (49.5) |
488 (52.3) |
482 (52.1) |
1,427 (51.3) |
| ≥80, n (%) |
204 (22.1) |
203 (21.8) |
199 (21.5) |
606 (21.8) |
| CHADS2 score |
| 0–1, n (%) |
297 (32.2) |
280 (30.0) |
264 (28.5) |
841 (30.2) |
| 2, n (%) |
293 (31.7) |
295 (31.6) |
329 (35.5) |
917 (33.0) |
| 3, n (%) |
203 (22.0) |
227 (24.3) |
204 (22.0) |
634 (22.8) |
| 4–6, n (%) |
130 (14.1) |
131 (14.0) |
129 (13.9) |
390 (14.0) |
| Previous stroke, n (%) |
221 (23.9) |
233 (25.0) |
218 (23.5) |
672 (24.2) |
| Previous myocardial infarction, n (%) |
95 (10.3) |
83 (8.9) |
82 (8.9) |
260 (9.3) |
| Heart failure, n (%) |
350 (37.9) |
331 (35.5) |
330 (35.6) |
1,011 (36.3) |
| Diabetes, n (%) |
243 (26.3) |
230 (24.7) |
225 (24.3) |
698 (25.1) |
| Hypertension, n (%) |
647 (70.1) |
681 (73.0) |
652 (70.4) |
1,980 (71.2) |
| Medications |
| ASA, n (%) |
441 (47.8) |
418 (44.8) |
452 (48.8) |
1,309 (47.1) |
| ARB, n (%) |
306 (33.2) |
311 (33.3) |
297 (32.1) |
914 (32.9) |
| ACEI, n (%) |
274 (29.7) |
261 (28.0) |
255 (27.5) |
790 (28.4) |
| β-blocker, n (%) |
409 (44.3) |
445 (47.7) |
432 (46.7) |
1,286 (46.2) |
| Amiodarone, n (%) |
142 (15.4) |
123 (13.2) |
129 (13.9) |
394 (14.2) |
| Verapamil, n (%) |
43 (4.7) |
42 (4.5) |
45 (4.9) |
130 (4.7) |
| Proton pump inhibitor, n (%) |
70 (7.6) |
80 (8.6) |
72 (7.8) |
222 (8.0) |
| H2 blocker, n (%) |
58 (6.3) |
49 (5.3) |
48 (5.2) |
155 (5.6) |
| Long term (>12 months) VKA use at entry, n (%) |
235 (25.5) |
226 (24.2) |
228 (24.6) |
689 (24.8) |
Patients with missing data are not shown. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; ASA, acetylsalicylic acid; CrCl, creatinine clearance; DE, dabigatran etexilate; SD, standard deviation; VKA, vitamin K antagonist.
In Asian patients, the mean CrCl was 65.3 ml/min, and >70% of patients had a CrCl ≥50 ml/min (Table 1). The mean CHADS2
score was 2.2 and the majority (>80%) of patients in each of the treatment groups had a CHADS2
score in the range of 0–3. The prevalence of history of stroke or transient ischemic attack (TIA) in the CHADS2
4–6 stratum in the DE and warfarin groups was as high as 92.8%. A history of stroke/TIA is the only component of the CHADS2
score contributing as many as 2 points to the total score. As expected, its prevalence strongly correlated with CHADS2
severity, decreasing to 57.6% in patients with a score of 3, and 15.7% in those with a score of 2. According to the definition of CHADS2, no patients with a history of stroke or TIA had a score of 0 or 1.
Efficacy Outcomes and Bleeding Events in Asian Patients According to Baseline Renal Function
Efficacy Outcomes
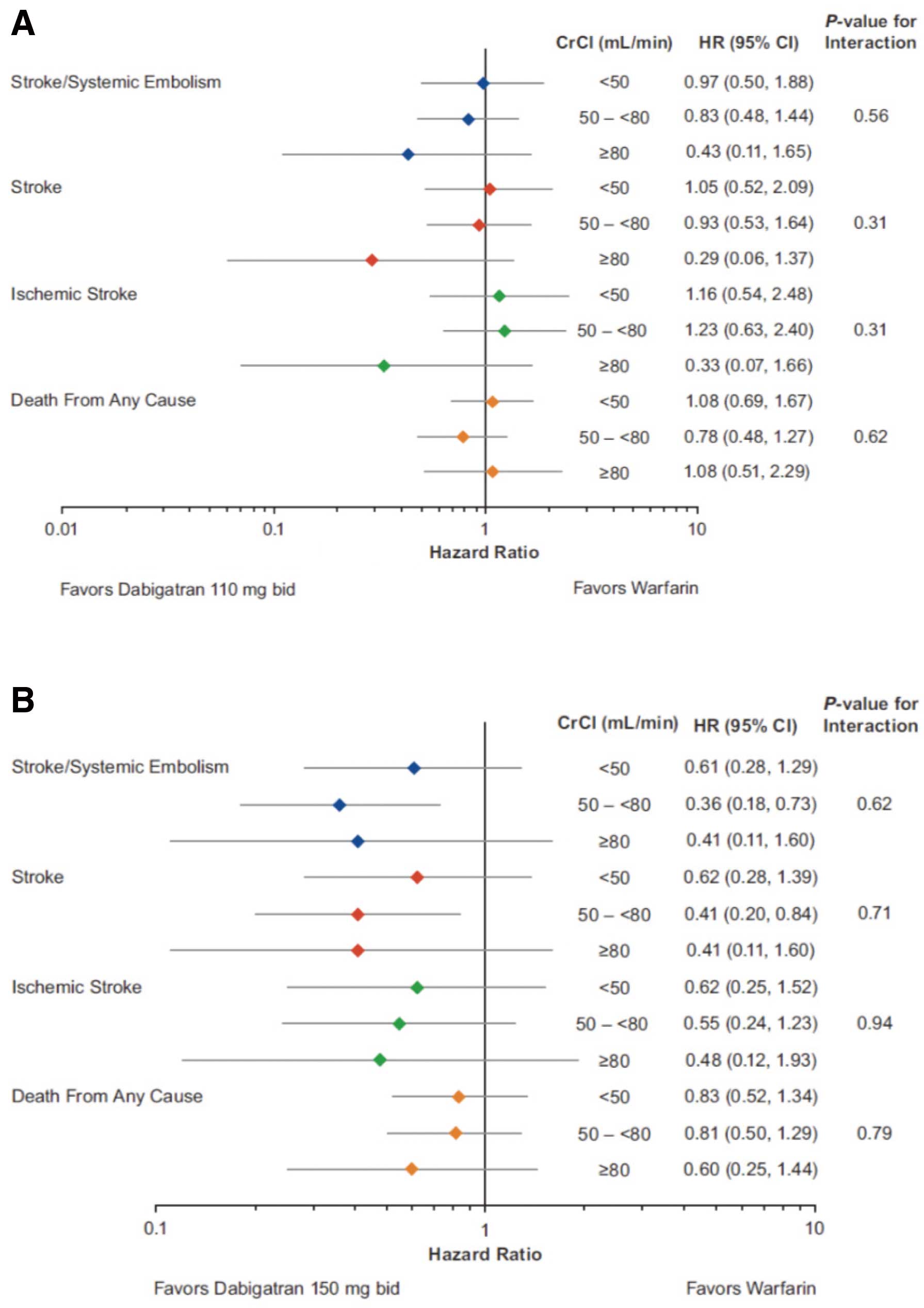
There was an increase in the absolute rates of stroke/systemic embolism with worsening renal function (Table 2). As expected for an older population that will have decreasing renal function, similar results were observed for the other efficacy parameters (Table 2). For stroke/systemic embolism, the HRs for the comparisons between DE 110 mg and warfarin ranged between 0.43 (95% CI: 0.11–1.65) and 0.97 (95% CI: 0.50–1.88) across the CrCl subgroups and between 0.36 (95% CI: 0.18–0.73) and 0.61 (95% CI: 0.28–1.29) for the DE 150 mg vs. warfarin comparison, with treatment benefits of DE vs. warfarin being consistent across renal function subgroups (Figures 1A,B); no treatment interaction was found for both 110 mg and 150 mg DE doses and efficacy outcomes (Pinteraction
for primary efficacy endpoint=0.56 and 0.62 for DE 110 mg and DE 150 mg, respectively).
Table 2.
Incidence of Efficacy Outcomes With DE vs. Warfarin in RE-LY Asian Patients by Baseline CrCl Category or CHADS
2 Score
| |
DE 110 mg (n=923) |
DE 150 mg (n=933) |
Warfarin (n=926) |
| Patients with event (%/year) |
Patients with event (%/year) |
Patients with event (%/year) |
| CrCl category (ml/min) |
| Stroke/systemic embolism |
| <50 |
18 (3.78) |
11 (2.42) |
17 (3.88) |
| 50–<80 |
23 (2.62) |
11 (1.17) |
28 (3.10) |
| ≥80 |
3 (0.77) |
3 (0.75) |
7 (1.82) |
| Stroke |
| <50 |
17 (3.57) |
10 (2.20) |
15 (3.43) |
| 50–<80 |
23 (2.62) |
11 (1.17) |
25 (2.76) |
| ≥80 |
2 (0.51) |
3 (0.75) |
7 (1.82) |
| Ischemic stroke |
| <50 |
15 (3.15) |
8 (1.76) |
12 (2.74) |
| 50–<80 |
19 (2.16) |
9 (0.96) |
16 (1.77) |
| ≥80 |
2 (0.51) |
3 (0.75) |
6 (1.56) |
| Death from any cause |
| <50 |
43 (9.03) |
32 (7.05) |
37 (8.45) |
| 50–<80 |
29 (3.30) |
32 (3.42) |
38 (4.20) |
| ≥80 |
14 (3.58) |
8 (2.01) |
13 (3.38) |
| CHADS2 score |
| Stroke/systemic embolism |
| 0–1 |
11 (1.92) |
7 (1.30) |
8 (1.66) |
| 2 |
10 (1.85) |
8 (1.42) |
16 (2.60) |
| 3 |
11 (2.82) |
4 (0.91) |
18 (4.56) |
| 4–6 |
12 (4.72) |
6 (2.35) |
11 (4.62) |
| Stroke |
| 0–1 |
11 (1.92) |
6 (1.12) |
7 (1.46) |
| 2 |
9 (1.66) |
8 (1.42) |
15 (2.43) |
| 3 |
10 (2.56) |
4 (0.91) |
17 (4.31) |
| 4–6 |
12 (4.72) |
6 (2.35) |
9 (3.78) |
| Ischemic stroke |
| 0–1 |
11 (1.92) |
6 (1.12) |
5 (1.04) |
| 2 |
6 (1.11) |
7 (1.24) |
11 (1.79) |
| 3 |
8 (2.05) |
3 (0.68) |
13 (3.30) |
| 4–6 |
11 (4.33) |
4 (1.56) |
6 (2.52) |
| Death from any cause |
| 0–1 |
26 (4.55) |
17 (3.16) |
19 (3.95) |
| 2 |
28 (5.17) |
20 (3.56) |
28 (4.54) |
| 3 |
21 (5.38) |
23 (5.25) |
22 (5.58) |
| 4–6 |
13 (5.12) |
12 (4.69) |
19 (7.97) |
The numbers of patients assigned to the treatment groups per CrCl category (<50 ml/min, 50–<80 ml/min, ≥80 ml/min) were as follows, respectively: DE 110 mg: 256, 457, and 204; DE 150 mg: 240, 488 and 203; warfarin: 244, 482 and 199. Overall, 9 Asian patients had missing data for CrCl and are not included in the data. The numbers of patients assigned to the treatment groups per CHADS2 score categories (0–1, 2, 3, 4–6) were as follows, respectively: DE 110 mg: 297, 293, 203, and 130; DE 150 mg: 280, 295, 227, and 131; warfarin: 264, 329, 204, and 129. Ischemic stroke does not include uncertain classification. Abbreviations as in Table 1.
Bleeding Events
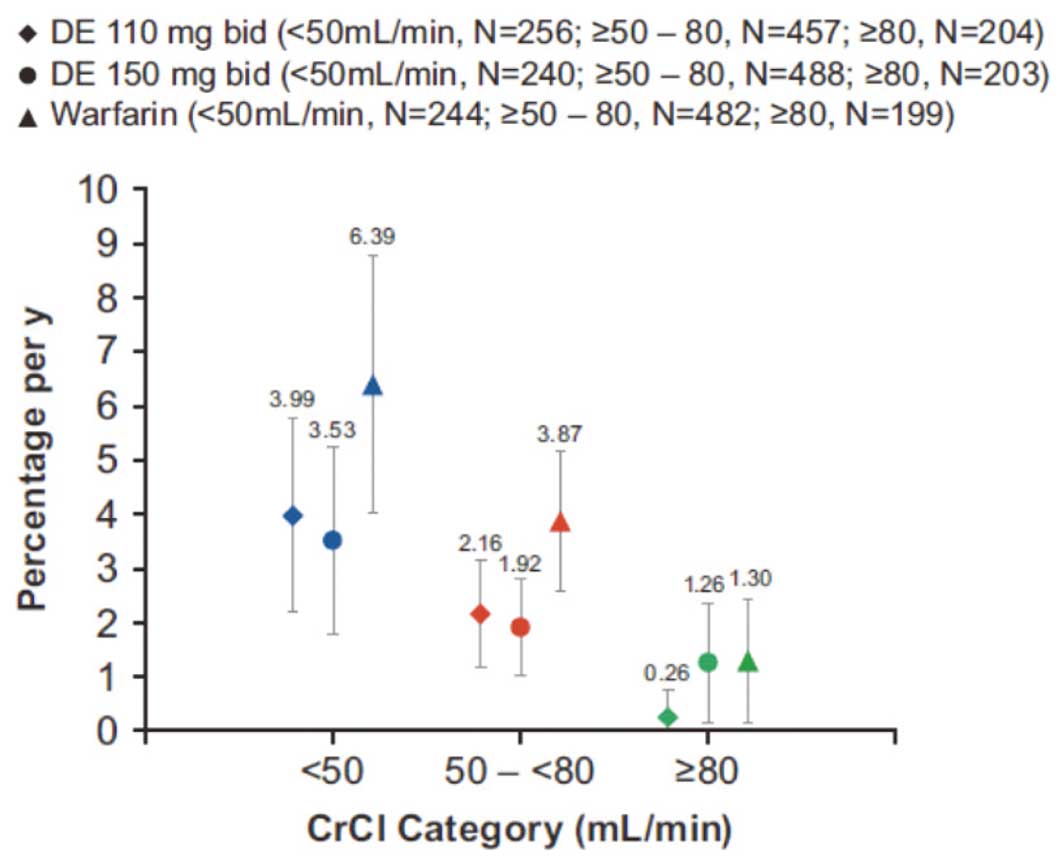
Similar to the total RE-LY,12
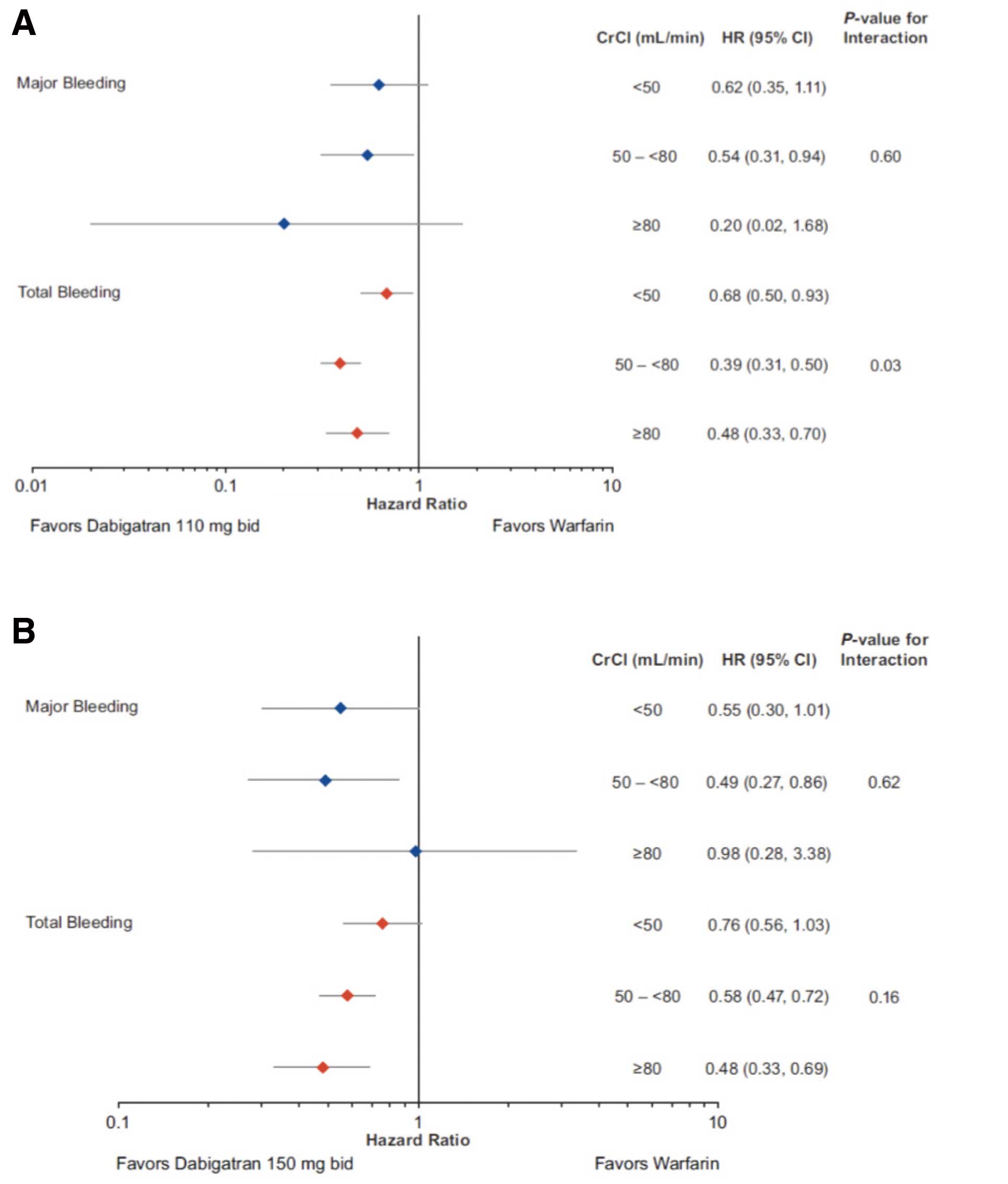
there was an increase in the rates of major bleeding with worsening renal function in both DE groups, as well as the warfarin arm, in the Asian population (Figure 2). For major bleeds, the HR for DE 110 mg vs. warfarin ranged between 0.20 (95% CI: 0.02–1.68) and 0.62 (95% CI: 0.35–1.11) across the CrCl categories (Figure 3A), and for DE 150 mg between 0.49 (95% CI: 0.27–0.86) and 0.98 (95% CI: 0.28–3.38) (Figure 3B); however, the interaction P-values for major bleeds were non-significant (Pinteraction=0.60 and 0.62 for DE 110 mg and DE 150 mg, respectively).
The beneficial effect of both doses of DE vs. warfarin on total bleeding was more pronounced in patients with a CrCl ≥50 ml/min compared with patients with levels <50 ml/min (Figures 3A,B). For DE 110 mg vs. warfarin, the HR ranged between 0.39 (95% CI: 0.31–0.50) and 0.68 (95% CI: 0.50–0.93) across the CrCl categories (Figure 3A), and for DE 150 mg between 0.48 (95% CI: 0.33–0.69) and 0.76 (95% CI: 0.56–1.03) (Figure 3B). A statistically significant treatment interaction by CrCl category was observed for the DE 110 mg b.i.d. dose (P=0.03), and a non-significant trend for the 150 mg b.i.d. dose (P=0.16).
Efficacy Outcomes and Bleeding Events in Asian Patients According to Baseline CHADS2
Score
Efficacy Outcomes
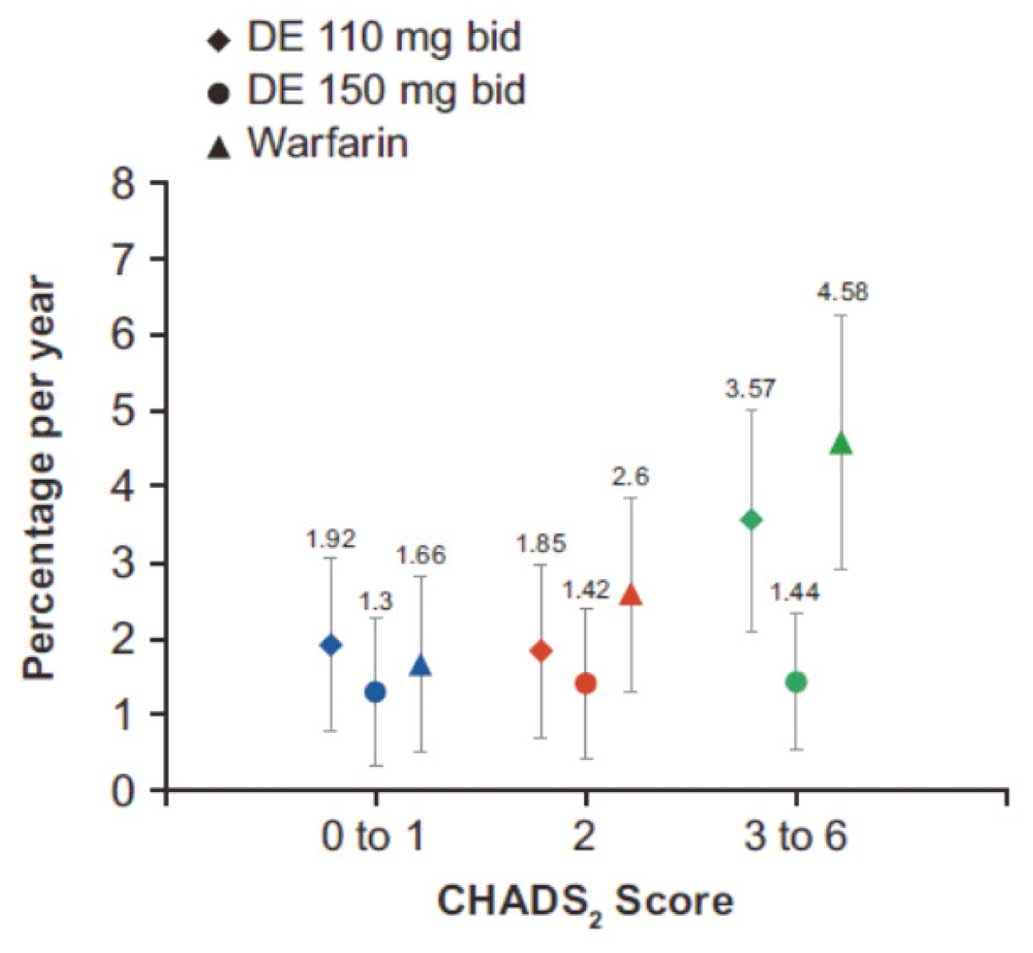
As expected, there was an increase in the rates of stroke/systemic embolism with worsening CHADS2
score (Figure 4). Although there was also an increase in the DE arms, this effect was less pronounced than with warfarin, particularly with the 150 mg b.i.d. dose, for all CHADS2
score categories (Figure 4), with a statistically significant risk reduction vs. warfarin in the CHADS2
3–6 category (HR 0.31, 95% CI 0.15–0.63). However, as for the overall RE-LY,13
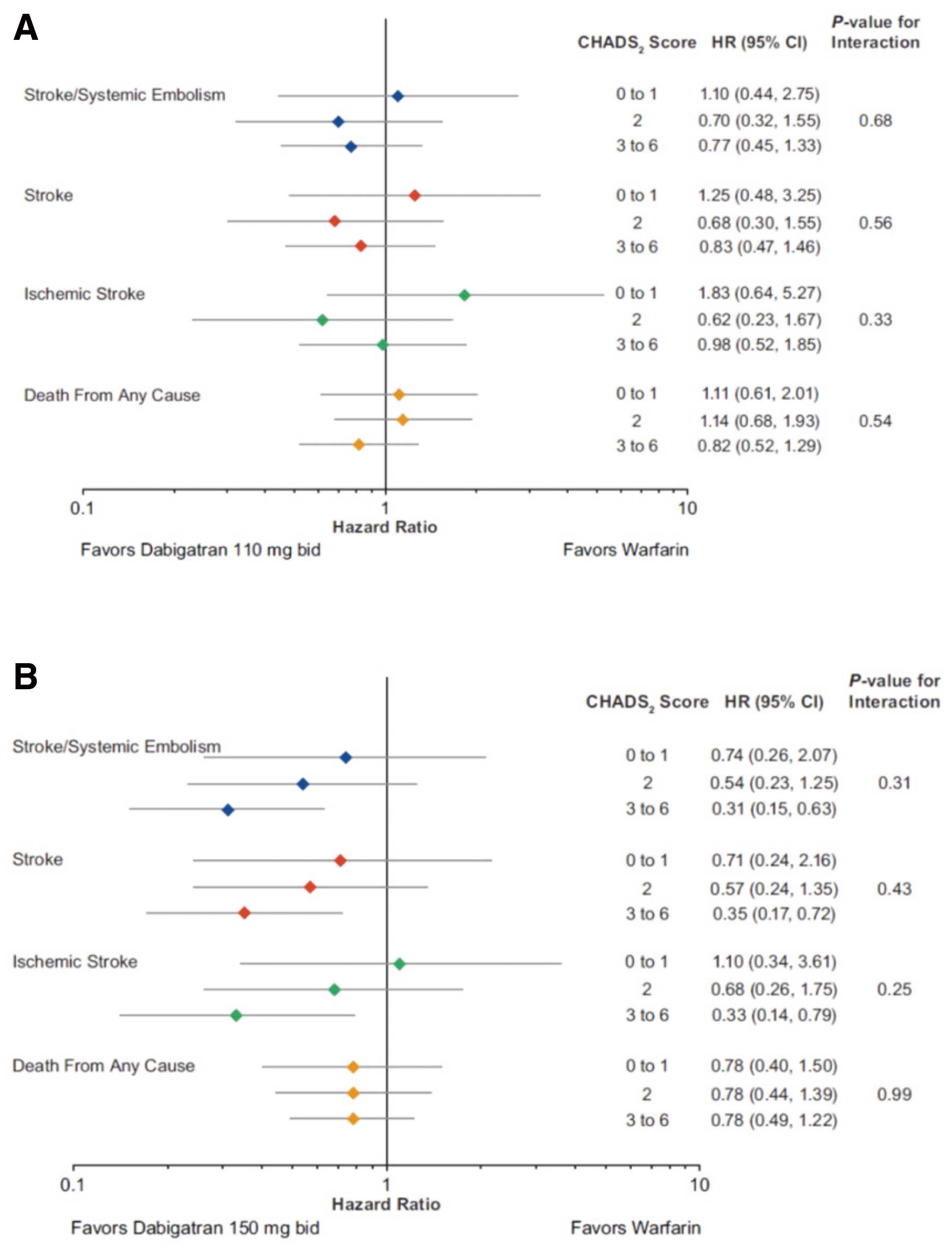
there was no significant interaction for both DE doses, and the primary endpoint (Pinteraction
for the primary efficacy endpoint was 0.68 and 0.31 for DE 110 mg and DE 150 mg, respectively) (Figures 5A,B). For DE 110 mg vs. warfarin, the HR ranged between 0.70 (95% CI: 0.32–1.55) and 1.10 (95% CI: 0.44–2.75) across the CHADS2
score categories (Figure 5), and for DE 150 mg between 0.31 (95% CI: 0.15–0.63) and 0.74 (95% CI: 0.26–2.07).
Bleeding Events
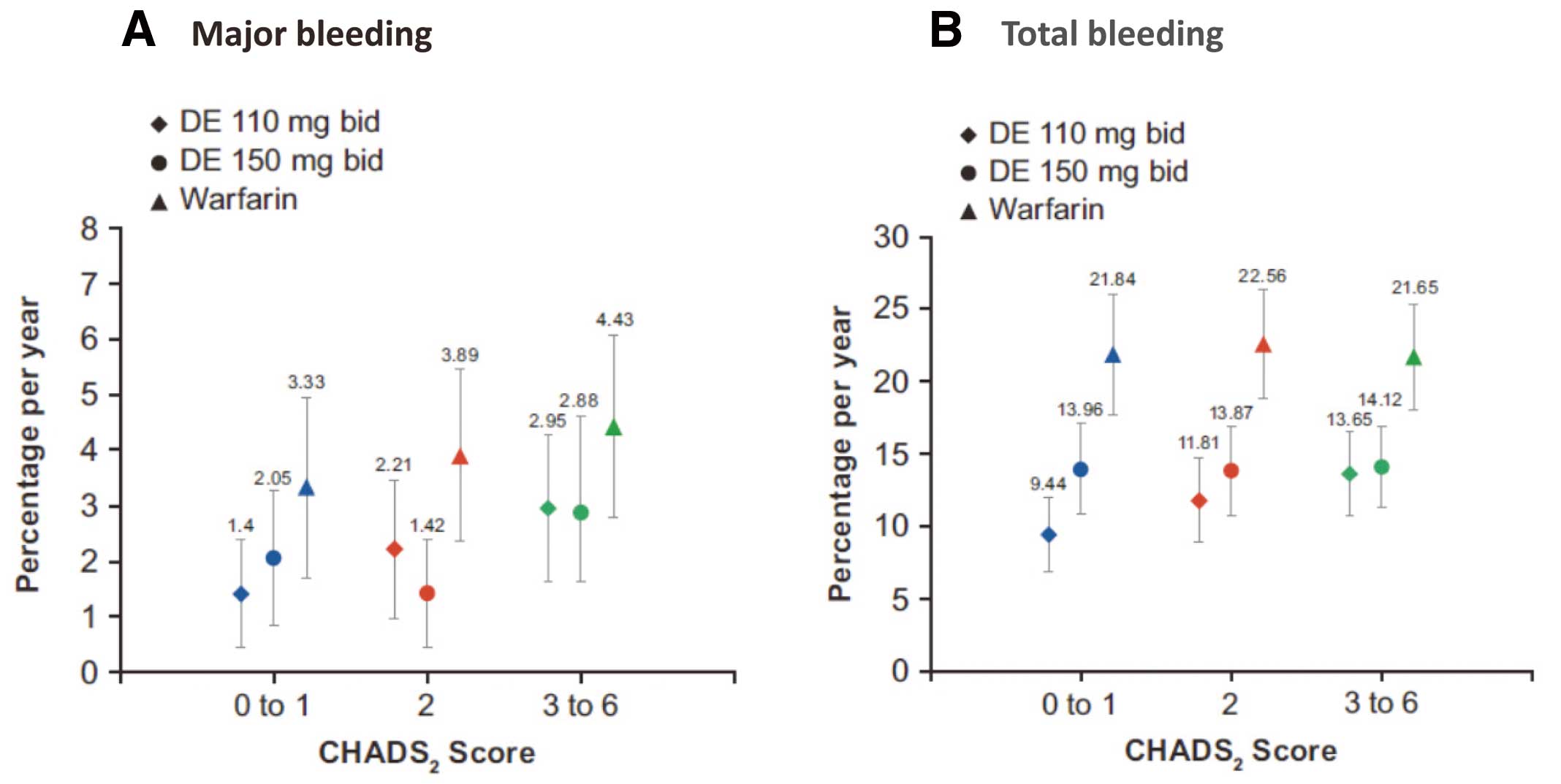
Yearly event rates for major and total bleeding events within the treatment groups (Figures 6A,B) also tended to increase with increasing CHADS2
scores; the increase in risk was less pronounced as for stroke/systemic embolism. The effect of DE was consistent among CHADS2
score categories: there was no significant interaction for both DE doses and major bleeding (Pinteraction
was 0.70 and 0.48 for DE 110 mg and DE 150 mg, respectively, in the CHADS2
categories of 0 or 1, 2, and 3–6) or total bleeding (Pinteraction
was 0.15 and 0.89 for DE 110 mg and DE 150 mg, respectively, in the CHADS2
categories of 0 or 1, 2, and 3–6). For major bleeding events for DE 110 mg vs. warfarin, the HR ranged between 0.40 (95% CI: 0.17–0.94) and 0.66 (95% CI: 0.37–1.18) across the CHADS2
score categories (Figures 6A,B), and for DE 150 mg between 0.36 (95% CI: 0.16–0.81) and 0.66 (95% CI: 0.37–1.16).
Discussion
The RE-LY is one of the largest stroke prevention trials undertaken in AF patients.9,14
Previously, when regional differences between the Asian and non-Asian subgroups in the study were evaluated, no interaction was observed in terms of efficacy endpoints in either the 110 mg or 150 mg dose group of DE.10
However, HRs in the Asian subgroup favored DE vs. warfarin for all primary and secondary bleeding endpoints, suggesting an improved safety benefit of DE. The regional effect was especially marked in the DE 150 mg group; a significantly larger relative risk reduction (RRR) was observed in major bleeding, minor bleeding, and net clinical benefit (composite of stroke, systemic embolism, pulmonary embolism, myocardial infarction including silent myocardial infarction, death, or major bleeding). In terms of total bleeding, a significant interaction was observed in both dose groups, with a larger RRR in Asians compared with non-Asians. In contrast to non-Asians, there was no increase in gastrointestinal bleeding in the Asian subgroup with the higher DE dose (150 mg b.i.d.). These regional differences are considered to be related to the fact that, firstly, the safety profile of warfarin in Asians is inferior to that in non-Asians (for major bleeding, the annual event rate is 3.8% vs. 3.5%, respectively, and for total bleeding, 22.0% vs. 17.7%, respectively).10
Secondly, the safety profile of DE in Asians is superior to that in non-Asians (for total bleeding, the annual event rate of DE 150 mg is 14.0% vs. 17.0%, respectively; the annual event rate of DE 110 mg is 11.7% vs. 15.3%, respectively).10
The subgroup analysis presented here aimed to demonstrate the effect of risk categories based on renal function and CHADS2
score in Asians on the selection of doses of DE.
The main finding of the RE-LY Asian analysis was that there was no treatment interaction for both 110 mg and 150 mg DE compared with warfarin on stroke/systemic embolism in subgroups defined by renal function and CHADS2
score. In Asians, risk categories based on baseline renal function or CHADS2
score at baseline did not have a significant effect on the efficacy of both doses of DE in comparison with warfarin. In comparison, a subgroup analysis of the total RE-LY population showed that the rate of stroke or systemic embolism increased for each 1-point increase in the CHADS2
risk score (P<0.001).13
As expected in this study, there was an increase in the rates of major bleeding with worsening renal function in all treatment arms, with no significant interaction observed in either dose group. Also, a risk reduction of total bleeding was observed in patients with a preserved renal function (CrCl ≥50 ml/min), a statistically significant interaction was observed in the 110 mg group, and a non-significant trend in the 150 mg group.
Although no interaction was observed in other categories, an increase in the rate of stroke/systemic embolism and all deaths associated with an increase in CHADS2
score was consistently observed in the overall RE-LY population,13
as well as in the Asian population. Similar results have been reported previously in other trials and outpatient registries.15–18
There was also a trend for an increase in major bleeding events in Asians with increasing CHADS2
score. Similar to the whole RE-LY trial, there was no significant interaction of CHADS2
score at baseline on efficacy or major bleeding in either DE or warfarin in Asians.13
This subanalysis confirms that both DE 110 mg and 150 mg b.i.d. are reasonable alternatives to warfarin based on the outcome data obtained from various renal function and CHADS2
score categories. No significant interaction associated with CHADS2
severity was confirmed for either DE 110 mg or 150 mg, suggesting consistent efficacy of both doses of DE in comparison with warfarin, regardless of the risk for stroke. These results are supported by those for the total RE-LY population, with no significant interactions for renal impairment with regard to ischemic stroke (P<0.69).19
In addition, in the analysis according to renal function in this study, a significant interaction was not demonstrated for major bleeding, although total bleeding in the DE 110 mg group was significant. In comparison, in the total RE-LY population, there were significant interactions between treatment and renal function for major bleeding according to Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease equations (P<0.05).19
The majority of non-valvular AF patients in clinical settings have normal renal function or mild impairment.20,21
The results of this study indicated that DE may provide a balance between the risk for ischemic stroke and the risk for bleeding in patients with decreased renal function (CrCl <50 ml/min). At the same time, it is suggested that a high dose of DE (150 mg) can be effective and may be recommended for patients with a high risk for stroke and slightly decreased renal function, despite the fact that DE is ~80% eliminated renally. The prevalence of a history of stroke or TIA in patients with a CHADS2
score between 4 and 6 was 92.8%, whereas the incidence of stroke/systemic embolism in patients receiving DE 150 mg was lower than that in patients receiving warfarin or DE 110 mg. This finding also suggests that administration of DE 150 mg may be a particularly desirable treatment strategy for Asian patients with a history of stroke and a high CHADS2
score if the risk for bleeding can be controlled.
Study Limitations
The present study was a post-hoc analysis of a limited sample size, so the results should be interpreted with caution and considered exploratory. Moreover, this study was limited by being a subanalysis of a large randomized trial. HRs in subgroups, in particular, have wide CIs and tests for treatment by CrCl and CHADS2
interaction have a low power to detect heterogeneity of treatment effect for any rare outcome events. Consequently, a non-significant result does not rule out the possibility of treatment heterogeneity. Data therefore need to be interpreted in the context of the overall RE-LY results. Furthermore, when the results of randomized clinical trials for the risk of bleeding are applied to real-world practice, it should be taken into account that assessment of bleeding may not be so rigorous in the real world.
Conclusions
In Asian patients who participated in the RE-LY, bleeding and stroke rates varied according to renal function and CHADS2
score, but the relative efficacy and safety of DE compared with warfarin were preserved across various renal function and CHADS2
categories.
No interaction was observed between CHADS2
score or renal function category and efficacy or major bleeding outcomes. Both doses of DE can be considered as appropriate alternatives to conventional warfarin therapy. The 110 mg b.i.d. dose can be an attractive treatment option for patients at higher risk of bleeding, and the 150 mg b.i.d. dose can be an attractive treatment option for patients with a history of stroke (ie, patients with a high CHADS2
score and a high risk for ischemic stroke). The findings of this study should be used as a reference for treatment strategy in the clinical setting.
Acknowledgments
All authors were fully responsible for all content and editorial decisions, were involved at all stages of manuscript development and have approved the final version for submission. The authors met the criteria for authorship as recommended by the International Committee of Medical Journal Editors and received no compensation related to the development of the manuscript.
This study was funded by Boehringer Ingelheim. Editorial and writing assistance was provided by Lakshmi Venkatraman, PhD, and Lisa Lovelidge, PhD, of PAREXEL, with funding from Boehringer Ingelheim.
Disclosures
Name of Grant: Nippon Boehringer Ingelheim Co, Ltd.
Conflict of Interest Statement
M.H. has received consultancy fees from Boehringer Ingelheim, Bayer, Bristol-Myers Squibb and Pfizer. T.F. is an employee of Nippon Boehringer Ingelheim. E.K. is an employee of Boehringer Ingelheim. P.A.R. is an employee of Boehringer Ingelheim Pharmaceuticals. M.D.E. has no conflicts to report, S.J.C. reports grants and personal fees from Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Sanofi/Pfizer, Sanofi Aventis, Bayer, and personal fees from Portola, grants from Boston Scientific, outside the submitted work, and an institutional grant from Boehringer Ingelheim.
References
- 1.
Inoue H. Thromboembolism in patients with nonvalvular atrial fibrillation: Comparison between Asian and Western countries. J Cardiol 2013; 61: 1–7.
- 2.
Inoue H, Fujiki A, Origasa H, Ogawa S, Okumura K, Kubota I, et al. Prevalence of atrial fibrillation in the general population of Japan: An analysis based on periodic health examination. Int J Cardiol 2009; 137: 102–107.
- 3.
Ogawa S, Hori M. Urgent statement on antithrombotic therapy of atrial fibrillation. Circ J 2011; 75: 2719–2721.
- 4.
Atarashi H, Inoue H, Okumura K, Yamashita T, Kumagai N, Origasa H. Present status of anticoagulation treatment in Japanese patients with atrial fibrillation: A report from the J-RHYTHM Registry. Circ J 2011; 75: 1328–1333.
- 5.
JCS Joint Working Group. Guidelines for pharmacotherapy of atrial fibrillation (JCS 2013): Digest version. Circ J 2014; 78: 1997–2021.
- 6.
Apostolakis S, Guo Y, Lane DA, Buller H, Lip GY. Renal function and outcomes in anticoagulated patients with non-valvular atrial fibrillation: The AMADEUS trial. Eur Heart J 2013; 34: 3572–3579.
- 7.
Olesen JB, Lip GY, Kamper AL, Hommel K, Kober L, Lane DA, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med 2012; 367: 625–635.
- 8.
Boehringer Ingelheim. Press release archive: SPAF. http://www.boehringer-ingelheim.com/news/news_releases/press_releases/2014/06_march_2014_dabigatranetexilate.html (accessed December 12, 2014).
- 9.
Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009; 361: 1139–1151.
- 10.
Hori M, Connolly SJ, Zhu J, Liu LS, Lau CP, Pais P, et al. Dabigatran versus warfarin: Effects on ischemic and hemorrhagic strokes and bleeding in Asians and non-Asians with atrial fibrillation. Stroke 2013; 44: 1891–1896.
- 11.
Yasaka M, Lip GY. Impact of non-vitamin k antagonist oral anticoagulants on intracranial bleeding in Asian patients with non-valvular atrial fibrillation. Circ J 2014; 78: 2367–2372.
- 12.
Eikelboom JW, Wallentin L, Connolly SJ, Ezekowitz M, Healey JS, Oldgren J, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: An analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trial. Circulation 2011; 123: 2363–2372.
- 13.
Oldgren J, Alings M, Darius H, Diener HC, Eikelboom J, Ezekowitz MD, et al. Risks for stroke, bleeding, and death in patients with atrial fibrillation receiving dabigatran or warfarin in relation to the CHADS2 score: A subgroup analysis of the RE-LY trial. Ann Intern Med 2011; 155: 660–667.
- 14.
Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L. Newly identified events in the RE-LY trial. N Engl J Med 2010; 363: 1875–1876.
- 15.
Fox KA, Piccini JP, Wojdyla D, Becker RC, Halperin JL, Nessel CC, et al. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial fibrillation and moderate renal impairment. Eur Heart J 2011; 32: 2387–2394.
- 16.
Go AS, Fang MC, Udaltsova N, Chang Y, Pomernacki NK, Borowsky L, et al. Impact of proteinuria and glomerular filtration rate on risk of thromboembolism in atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Circulation 2009; 119: 1363–1369.
- 17.
Hohnloser SH, Hijazi Z, Thomas L, Alexander JH, Amerena J, Hanna M, et al. Efficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: Insights from the ARISTOTLE trial. Eur Heart J 2012; 33: 2821–2830.
- 18.
Piccini JP, Stevens SR, Chang Y, Singer DE, Lokhnygina Y, Go AS, et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: Validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation 2013; 127: 224–232.
- 19.
Hijazi Z, Hohnloser SH, Oldgren J, Andersson U, Connolly SJ, Eikelboom JW, et al. Efficacy and safety of dabigatran compared with warfarin in relation to baseline renal function in patients with atrial fibrillation: A RE-LY (Randomized Evaluation of Long-term Anticoagulation Therapy) trial analysis. Circulation 2014; 129: 961–970.
- 20.
Akao M, Chun YH, Wada H, Esato M, Hashimoto T, Abe M, et al. Current status of clinical background of patients with atrial fibrillation in a community-based survey: The Fushimi AF Registry. J Cardiol 2013; 61: 260–266.
- 21.
Toyoda K, Arihiro S, Todo K, Yamagami H, Kimura K, Furui E, et al; SAMURAI Study Investigators. Trends in oral anticoagulant choice for acute stroke patients with nonvalvular atrial fibrillation in Japan: The SAMURAI-NVAF Study. Int J Stroke 2015; 10: 836–842.