Abstract
Background:
Several non-invasive methods for measuring pulmonary vascular resistance (PVR) have been proposed to date, but they remain empirical, lacking sufficient accuracy to be used in clinical practice. The aims of this study were to propose a novel echocardiographic measurement of PVR based on a theoretical formula and investigate the feasibilty and accuracy of this method in patients with heart failure.
Methods and Results:
Echocardiography was performed in 27 patients before right heart catheterization. Peak tricuspid regurgitation pressure gradient (TRPG), pulmonary regurgitation pressure gradient in end-diastole (PRPGed), and cardiac output derived from the time-velocity integral and the diameter in the left ventricular outflow tract (COLVOT) were measured. PVR based on a theoretical formula (PVRtheo) was calculated as (TRPG–PRPGed)/3COLVOT
in Wood units (WU). The results were compared with PVR obtained by right heart catheterization (PVRcath) using linear regression and Bland-Altman analysis. Mean PVRcath
was 2.4±1.4 WU. PVRtheo
correlated well with PVRcath
(r=0.83, P<0.001). On Bland-Altman analysis the mean difference was 0.1±0.7 WU. The limits of agreements were smaller than for other non-invasive estimations previously reported.
Conclusions:
The new echocardiographic approach based on a theoretical formula provides a non-invasive and accurate assessment of PVR in patients with heart failure. (Circ J 2015; 79: 2408–2413)
Pulmonary hypertension resulting from heart failure carries a poor prognosis.1,2
Although pulmonary vascular resistance (PVR) is an important pathophysiologic parameter in patients with heart failure as well as with pulmonary hypertension, its use has been limited because of the invasiveness of right heart catheterization required for measurement.3–8
The invasive nature of right heart catheterization is an obstacle to the repeated measurement required for the assessment of therapeutic interventions, as well as the time course of the disease. Doppler echocardiography provides a simple and non-invasive means of assessing hemodynamics.9–11
To date, several non-invasive methods have been proposed to estimate PVR,12–14
but they remain empirical, lacking sufficient accuracy to be used in cardiology practice. In this study, we propose a new echocardiographic measurement of PVR based on a theoretical formula (PVRtheo). We also investigated whether PVRtheo
had improved accuracy in clinical settings by comparing PVRtheo
with PVRcath, and also with earlier non-invasive methods in patients with heart failure.
Editorial p 2324
Methods
Subjects
We consecutively enrolled 27 patients with heart failure who underwent echocardiography and right heart catheterization on the same day. All patients underwent right heart catheterization using a thermodilution catheter within 6 h of echocardiography. Exclusion criteria consisted of tricuspid regurgitation grade >2, shunt disease, aortic stenosis or aortic regurgitation grade>2 to exclude inaccurate measurement of cardiac output (CO) with the thermodilution method.
Right Heart Catheterization
Right heart catheterization was performed using a thermodilution catheter (Goodman, Tokyo, Japan) with jugular venous access. The following pressure measurements were obtained: right atrial pressure (RAP), right ventricular pressure (RVP), pulmonary artery systolic pressure (PASP), pulmonary artery end-diastolic pressure (PADP), mean pulmonary artery pressure (MPAP) and right pulmonary capillary wedge pressure (PCWP). CO was determined using a standard thermodilution technique (mean of 3 consecutive measurements).4,5
All patients were in a stable condition between echocardiography and right heart catheterization. Neither volume loading nor bolus injection of diuretics was done between echocardiography and right heart catheterization. PVRcath
was obtained using right heart catheterization as: (MPAP–PCWP)/CO.4,5
Transthoracic Echocardiography
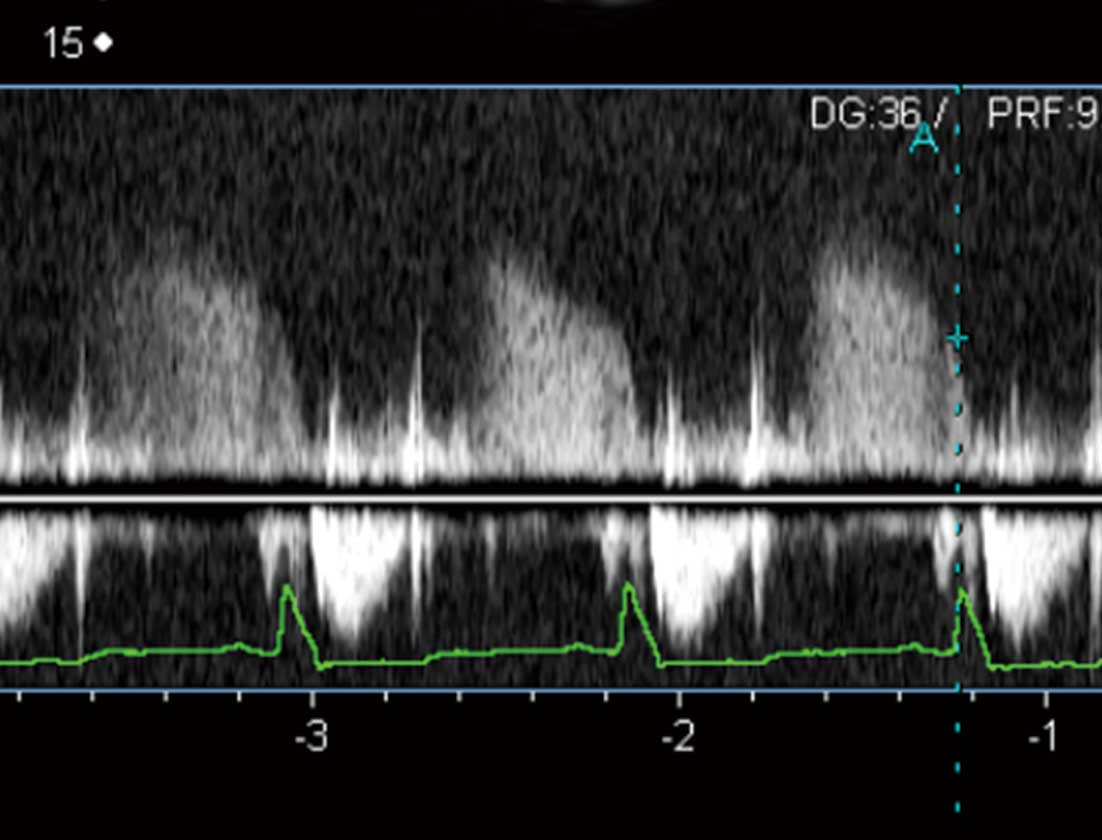
Comprehensive 2-D Doppler echocardiography was performed using a commercially available ultrasound apparatus (Artida or Aplio, Toshiba Medical Systems, Tochigi, Japan). We measured peak tricuspid regurgitation pressure gradient (TRPG), pulmonary regurgitation pressure gradient in end-diastole (PRPGed), and CO derived from the diameter and the time-velocity integral (TVI) in the left ventricular outflow tract (COLVOT) on echocardiography. PRPGed
was measured using a continuous wave Doppler technique and pressure gradient was calculated using the simplified Bernoulli equation in end-diastole (Figure 1). In patients with atrial fibrillation, echocardiographic parameters were obtained when the preceding RR interval and the pre-preceding RR interval were equal to the average RR interval.
Theoretical Formula for PVR
PVR was defined as: (MPAP–PCWP)/CO.4,5,12
Echocardiographic PVR (PVRtheo) was determined based on several theoretical assumptions: (1) pressure gradient was calculated from the Doppler-derived regurgitation velocity using the simplified Bernoulli equation;15
(2) mean blood pressure was weighted 2:1 in favor of the diastolic blood pressure: MPAP was derived from the estimated PADP and PASP according to the formula MPAP=DPAP+1/3(PASP–PADP);13
(3) PCWP was equal to PADP; and (4) the RV end-diastolic pressure and RAP were equal in end-diastole.16
Based on these assumptions, the following calculations were made: PADP=PRPGed+RAP; PASP=TRPG+RAP. TVI from a pulsed Doppler technique and the LV outflow tract (LVOT) diameter were calculated in the LVOT, and provided for CO calculation because there were no shunt diseases involved. Given that the RV outflow tract (RVOT) diameter is more difficult to measure than LVOT diameter, particularly in adults, we chose to measure CO in the LVOT rather than in the RVOT provided that there was no shunt disease involved.14
Using these parameters, PVR was therefore calculated as:
PVR=(MPAP–PCWP)/CO
={[PADP+(PASP–PADP)/3]–(PRPGed+CVP)}/CO
={[PRPGed+CVP+(TRPG+CVP–PRPGed–CVP)/3]–(PRPGed+CVP)}/CO
=(TRPG–PRPGed)/(3×COLVOT).
Finally, PVRtheo
was defined as: (TRPG–PRPGed)/(3×COLVOT).
PVR was also calculated based on the earlier methods proposed by Abbas et al, Scapellato et al, Haddad et al and Kouzu et al in the same cohort of patients.12,13,17,18
In brief, PVR by Abbas et al (PVRAbbas) was based on the ratio of peak tricuspid regurgitant velocity (TRV) to TVI in the RV outflow tract. PVR by Scapellato et al (PVRScapellato) was based on a ratio of systolic time interval involving the pre-ejection period (PEP), acceleration time (AcT), ejection time, and total systolic time (TT): index=([PEP/AcT]/TT). PVR by Haddad et al (PVRHaddad) was based on the index of SPAP/(HR×TVI), where SPAP is systolic pulmonary artery pressure and HR is heart rate. SPAP was estimated as RV systolic pressure, which equals the sum of the trans-tricuspid regurgitation gradient based on the simplified Bernoulli equation and the echocardiographically estimated RAP. PVR by Kouzu et al (PVRKouzu) was based on the ratio of TRPG to TVI.
This study was approved by the institutional review board, and written informed consent was obtained from each patient.
Statistical Analysis
All statistical analysis were performed using SPSS (SPSS version 22; Chicago, IL, USA). Categorical values are expressed as absolute and relative frequencies. Continuous values are expressed as mean ± SD. Linear regression analysis was generated between PVRcath
and the PVRs (PVRtheo, PVRAbbas, PVRScapellato, PVRHaddad, and PVRKouzu) non-invasively obtained by the earlier methods. Pearson’s correlation coefficients were then obtained. The 95% CI are reported when required. Bland-Altman analysis was carried out for invasive PVR and the non-invasively obtained PVRs.19
Results
Patient Characteristics
Of the 27 patients who underwent right heart catheterization, 5 patients (19%) were excluded because PRPGed
was unmeasurable. Clinical characteristics are presented in
Table 1. Referral diagnosis included ischemic heart disease (n=6), dilated cardiomyopathy (n=6), hypertrophic cardiomyopathy (n=2), valvular heart disease (n=2), hypertensive heart disease (n=2), tachycardia-induced cardiomyopathy (n=1), cardiac sarcoidosis (n=1), pulmonary hypertension (n=1), and other (n=1). Hemodynamic and echocardiographic characteristics are given in
Table 2.
Table 1.
Patient Characteristics
| Characteristics |
Results |
| Age (years) |
65±12 |
| Male |
12 (55) |
| Height (cm) |
161±11 |
| Body weight (kg) |
63±18 |
| NYHA class |
| I |
1 (5) |
| II |
14 (64) |
| III |
6 (27) |
| IV |
1 (5) |
| Heart rate (beats/min) |
68±14 |
| Atrial fibrillation |
6 (27) |
| BNP (pg/ml) |
367±280 |
Data given as mean ± SD or n (%). BNP, brain natriuretic peptide; NYHA, New York Heart Association.
Table 2.
Hemodynamic and Echocardiographic Characteristics
| |
Data |
| Hemodynamic parameters |
| Heart rate (beats/min) |
71±16 |
| PASP (mmHg) |
32.2±16.8 |
| PADP (mmHg) |
15.1±12.1 |
| MPAP (mmHg) |
21.5±13.3 |
| PCWP (mmHg) |
11.8±10.6 |
| RAP (mmHg) |
4.2±4.6 |
| PVR (WU) |
2.4±1.4 |
| CO (L/min) |
4.0±0.8 |
| Echocardiographic parameters |
| Heart rate (beats/min) |
68±14 |
| EF (%) |
43.3±12.4 |
| LAD (mm) |
46.7±12.4 |
| TRPG (mmHg) |
24.8±6.0 |
| PRPGed (mmHg) |
4.7±2.9 |
| COLVOT (L/min) |
3.1±0.7 |
Data given as mean ± SD. CO, cardiac output; COLVOT, CO from the time-velocity integral at the LV outflow tract; EF, ejection fraction; LAD, left atrial diameter; MPAP, mean pulmonary artery pressure; PADP, pulmonary artery diastolic pressure; PASP, pulmonary artery systolic pressure; PCWP, pulmonary capillary wedge pressure; PRPGed, pulmonary regurgitation pressure gradient at end-diastole; PVR, pulmonary vascular resistances; RAP, right atrial pressure; TRPG, tricuspid regurgitation pressure gradient; WU, Wood units.
Linear regression analysis indicated a significant correlation between PVRcath
and PVRtheo
(r=0.83, 95% CI: 0.64–0.93, P<0.001,
Figure 2). The equation of the regression line was: PVRcath=1.16×PVRtheo+0.23. The 95% CI for slope and intercept included 1 and 0, respectively. On Bland-Altman analysis the mean difference was −0.1 Wood units (WU) ±1.6 WU (2 SD limit of agreement;
Figure 3). In contrast, PVRAbbas, PVRScapellato, PVRHaddad
and PVRKouzu
had modest correlations with PVRcath
although this was statistically significant (PVRAbbas: r=0.52, 95% CI: 0.13–0.773, P=0.013; PVRHaddad: r=0.51, 95% CI: 0.12–0.77, P=0.13; PVRKouzu: r=0.68, 95% CI: 0.36–0.86, P<0.001). On Bland-Altman plots, PVRAbbas, PVRScapellato, PVRHaddad
and PVRKouzu
appeared to have larger differences in measurement than PVRtheo
(Figure 3).


Intraobserver and interobserver variability of measurements for PVRtheo
were also assessed in 10 randomly allocated patients. The mean intraobserver difference between the measurements was 0.10±0.53 WU. Intraclass correlation (ICC) was 0.89 (P<0.001). The mean difference between the 2 independent observers (T.K. and Y.M.) was 0.53±0.68 WU. ICC was 0.69 (P<0.001).
Discussion
We have proposed a new method for the non-invasive estimation of PVR based on a theoretical formula (PVRtheo). We found that (1) PVRtheo
was significantly correlated with invasive PVR, with the regression line close to y=x in a cohort of patients with left heart failure; and (2) PVRtheo
appeared to be accurate compared with earlier non-invasive methods.
PVR is calculated invasively as the ratio of transpulmonary pressure gradient to transpulmonary flow.4,5
Catheter-derived measurement remains the gold standard, which hampers routine use at the bedside. Accordingly, several non-invasive methods have been proposed to date. Among them, non-invasive estimations of PVR by Abbas et al, Scapellato et al, Haddad et al and Kouzu et al have shown relatively good agreement with invasive PVR. Nonetheless, the accuracy of these non-invasive methods remains suboptimal with regard to use in cardiology practice.14,17,18
Part of the difficulty was that those non-invasive PVRs remained empirical, and were not based on theory. Hence, in this study, we utilized theoretical formulae as far as possible in order to achieve accurate PVR measurement. Concurrently, we use measurements that were feasible on transthoracic echocardiography in the majority of adult patients. We used 3 parameters, TRPG, PRPGed
and COLVOT, to calculate PVRtheo. These are well established echocardiographic parameters that are easy to measure. Tricuspid regurgitation exists in the majority of patients with pulmonary hypertension.20
In addition, trivial-mild forms of pulmonary regurgitation are present in almost every patient.21
Although pulmonary regurgitation may be difficult to detect on Doppler echocardiography throughout diastole, it is relatively easy to detect if the measurement is limited to the end-diastole.
In general, there are 2 kinds of formulae for echocardiographically derived indices: theoretical formulae and empirical formulae. Theoretical formulae are those derived from physics theory. They are accurate as far as the theory can be applied to the particular conditions. The simplified Bernoulli equation to estimate pressure gradient is a good example.22
In contrast, empirical formulae are derived based on experience, that is, the statistical correlation between the parameters. They inherently include substantial errors of estimation. Examples include the estimation of mitral valve area in mitral stenosis using transmitral flow derived pressure half time,23,24
as well as the estimation of mean pulmonary arterial pressure by the AcT of the RV outflow velocity.25,26
In the present study, we exclusively utilized theoretical formulae for calculating PVR in order to minimize the error of estimation. Despite the use of several theoretical assumptions, we successfully estimated PVR by this method. It is noteworthy that 95% CI for slope and intercept included 1 and 0, in contrast to other earlier non-invasive estimation methods for PVR. For the best of our knowledge, this is the first repot of theoretically derived PVR estimation by echocardiography.
Clinical Implications
Because PVRtheo
was found to have substantial accuracy, it can be used to investigate the various conditions of pathophysiology in heart failure and/or pulmonary hypertension in clinical settings.
Study Limitations
There are several limitations in this study. First, the measurement of PRPGed
may encounter problems such as weak pulmonary regurgitant signal and improper Doppler angle. Nonetheless, even a trivial pulmonary regurgitation jet can often be measured if the measurement is limited to the end-diastole. Appropriate PRPGed
was able to be measured in most of the present patients (81%). Second, in patients with tachycardia, mean blood pressure may not be obtained as weighted 2:1 from the peak and nadir pressures. Care should be taken to calculate PVRtheo
under tachycardia. Third, PVRtheo
was tested only in those presenting with relatively mild elevation of PVR due to left heart failure. High PVR as seen in reactive pulmonary hypertension was not included in this study. In patients with reactive pulmonary hypertension, PCWP may not be equal to PADP. Therefore, PVRtheo
remains to be tested in those with pulmonary diseases. Fourth, COLVOT
is not the same as CO obtained using thermodilution catheter in the presence of significant cardiac shunt or aortic valvulopathy. The use of COLVOT
may not be a direct measure of right-sided CO. Nonetheless, we used COLVOT
in the calculation of PVRtheo
because the accuracy of measuring volumetric flow from the LVOT is higher than that measured from the right-sided vessels.14
Last, this pilot study involved a small sample size in a single center. A large-scale, multi-center study should be conducted to validate PVRtheo
in a generalized population.
Conclusions
This new echocardiographic approach based on a theoretical formula provides a non-invasive and accurate assessment of PVR in patients with heart failure.
References
- 1.
Guazzi M, Borlaug BA. Pulmonary hypertension due to left heart disease. Circulation 2012; 126: 975–990.
- 2.
Hirashiki A, Kondo T, Adachi S, Nakano Y, Shimazu S, Shimizu S, et al. Prognostic value of pulmonary hypertension in ambulatory patients with non-ischemic dilated cardiomyopathy. Circ J 2014; 78: 1245–1253.
- 3.
JCS Joint Working Group. Guidelines for treatment of acute heart failure (JCS 2011): Digest version. Circ J 2013; 77: 2157–2201.
- 4.
McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: A report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: Developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009; 119: 2250–2294.
- 5.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013; 62: e147–e239, doi:10.1016/j.jacc.2013.05.019.
- 6.
Braunwald E, Colucci WS. Vasodilator therapy of heart failure: Has the promissory note been paid? N Engl J Med 1984; 310: 459–461.
- 7.
Chemla D, Castelain V, Herve P, Lecarpentier Y, Brimioulle S. Haemodynamic evaluation of pulmonary hypertension. Eur Resp J 2002; 20: 1314–1331.
- 8.
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010; 23: 685–713; quiz 786–788.
- 9.
Eysmann SB, Palevsky HI, Reichek N, Hackney K, Douglas PS. Two-dimensional and Doppler-echocardiographic and cardiac catheterization correlates of survival in primary pulmonary hypertension. Circulation 1989; 80: 353–360.
- 10.
Yeo TC, Dujardin KS, Tei C, Mahoney DW, McGoon MD, Seward JB. Value of a Doppler-derived index combining systolic and diastolic time intervals in predicting outcome in primary pulmonary hypertension. Am J Cardiol 1998; 81: 1157–1161.
- 11.
D’Alto M, Romeo E, Argiento P, D’Andrea A, Vanderpool R, Correra A, et al. Accuracy and precision of echocardiography versus right heart catheterization for the assessment of pulmonary hypertension. Int J Cardiol 2013; 168: 4058–4062.
- 12.
Abbas AE, Fortuin FD, Schiller NB, Appleton CP, Moreno CA, Lester SJ. A simple method for noninvasive estimation of pulmonary vascular resistance. J Am Coll Cardiol 2003; 41: 1021–1027.
- 13.
Scapellato F, Temporelli PL, Eleuteri E, Corra U, Imparato A, Giannuzzi P. Accurate noninvasive estimation of pulmonary vascular resistance by Doppler echocardiography in patients with chronic failure heart failure. J Am Coll Cardiol 2001; 37: 1813–1819.
- 14.
Roule V, Labombarda F, Pellissier A, Sabatier R, Lognone T, Gomes S, et al. Echocardiographic assessment of pulmonary vascular resistance in pulmonary arterial hypertension. Cardiovasc Ultrasound 2010; 8: 21.
- 15.
Currie PJ, Seward JB, Reeder GS, Vlietstra RE, Bresnahan DR, Bresnahan JF, et al. Continuous-wave Doppler echocardiographic assessment of severity of calcific aortic stenosis: A simultaneous Doppler-catheter correlative study in 100 adult patients. Circulation 1985; 71: 1162–1169.
- 16.
Sakai K, Nakamura K, Satomi G, Kondo M, Hirosawa K. Evaluation of tricuspid regurgitation by blood flow pattern in the hepatic vein using pulsed Doppler technique. Am Heart J 1984; 108: 516–523.
- 17.
Haddad F, Zamanian R, Beraud AS, Schnittger I, Feinstein J, Peterson T, et al. A novel non-invasive method of estimating pulmonary vascular resistance in patients with pulmonary arterial hypertension. J Am Soc Echocardiogr 2009; 22: 523–529.
- 18.
Kouzu H, Nakatani S, Kyotani S, Kanzaki H, Nakanishi N, Kitakaze M. Noninvasive estimation of pulmonary vascular resistance by Doppler echocardiography in patients with pulmonary arterial hypertension. Am J Cardiol 2009; 103: 872–876.
- 19.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–310.
- 20.
Chan KL, Currie PJ, Seward JB, Hagler DJ, Mair DD, Tajik AJ. Comparison of three Doppler ultrasound methods in the prediction of pulmonary artery pressure. J Am Coll Cardiol 1987; 9: 549–554.
- 21.
Masuyama T, Kodama K, Kitabatake A, Sato H, Nanto S, Inoue M. Continuous-wave Doppler echocardiographic detection of pulmonary regurgitation and its application to noninvasive estimation of pulmonary artery pressure. Circulation 1986; 74: 484–492.
- 22.
Berger M, Haimowitz A, Van Tosh A, Berdoff RL, Goldberg E. Quantitative assessment of pulmonary hypertension in patients with tricuspid regurgitation using continuous wave Doppler ultrasound. J Am Coll Cardiol 1985; 6: 359–365.
- 23.
Martin RP, Rakowski H, Kleiman JH, Beaver W, London E, Popp RL. Reliability and reproducibility of two dimensional echocardiograph measurement of the stenotic mitral valve orifice area. Am J Cardiol 1979; 43: 560–568.
- 24.
Nichol PM, Gilbert BW, Kisslo JA. Two-dimensional echocardiographic assessment of mitral stenosis. Circulation 1977; 55: 120–128.
- 25.
Dabestani A, Mahan G, Gardin JM, Takenaka K, Burn C, Allfie A, et al. Evaluation of pulmonary artery pressure and resistance by pulsed Doppler echocardiography. Am J Cardiol 1987; 59: 662–668.
- 26.
Kitabatake A, Inoue M, Asao M, Masuyama T, Tanouchi J, Morita T, et al. Noninvasive evaluation of pulmonary hypertension by a pulsed Doppler technique. Circulation 1983; 68: 302–309.