Abstract
Background:
Predictors of worsening renal function (WRF: increase in serum creatinine ≥0.3 mg/dl from the value on admission) in patients with acute decompensated heart failure (ADHF) treated by low-dose carperitide (0.01–0.05 μg/kg/min) are unclear.
Methods and Results:
We retrospectively investigated predictors of WRF within the first 24 h of low-dose carperitide therapy in 205 patients (mean age, 75.6±12.1 years) hospitalized for ADHF and treated with low-dose carperitide between January 2006 and April 2014. WRF occurred in 14 patients (7%). A multivariate adjustment analysis showed that independent predictors of WRF within 24 h were hypotension (systolic blood pressure <90 mmHg) within 12 h (odds ratio, 8.7; 95% confidence interval, 2.38–35.88; P=0.0012) and serum creatinine on admission (odds ratio, 3.64; 95% confidence interval, 1.84–7.67; P=0.0003). In patients with estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2, the rate of WRF occurrence was higher in those complicated by hypotension than in those without hypotension (22.6% [7/31 patients] vs. 4.4% [5/113 patients], P=0.0041). In contrast, in patients with eGFR ≥60 ml/min/1.73 m2, hypotension did not influence the occurrence of WRF (0% [0/9 patients] vs. 3.9% [2/51 patients], P=NS).
Conclusions:
Hypotension within 12 h and renal dysfunction on admission are independent predictors of WRF within 24 h in patients with ADHF treated by low-dose carperitide. Hypotension may not cause WRF in patients with eGFR ≥60 ml/min/1.73 m2. (Circ J 2016; 80: 418–425)
Acute decompensated heart failure (ADHF) is the most common cause of hospitalization in many countries. It is associated with high in-hospital and postdischarge mortality and rehospitalization rates. Renal dysfunction after admission for ADHF has been consistently shown to be among the most important prognostic variables.1,2
Worsening renal function (WRF) occurs in approximately 20–30% of patients hospitalized for acute HF.3–6
Thus, WRF represents a significant and common event during acute HF, and its prevention remains an important target.
Since the launch of carperitide in 1995, a low-dose regimen has been widely used for treatment of patients with ADHF in Japan because some previous Japanese studies showed that it has a cardiorenal protective effect and improves prognosis.7–11
However, we sometimes experience WRF occurring in patients with ADHF treated by low-dose carperitide in the real world. The present study was conducted with expectations of selecting more suitable patients and achieving better treatment effects in patients with ADHF by clarifying the predictors of WRF after the initiation of low-dose carperitide therapy.
Methods
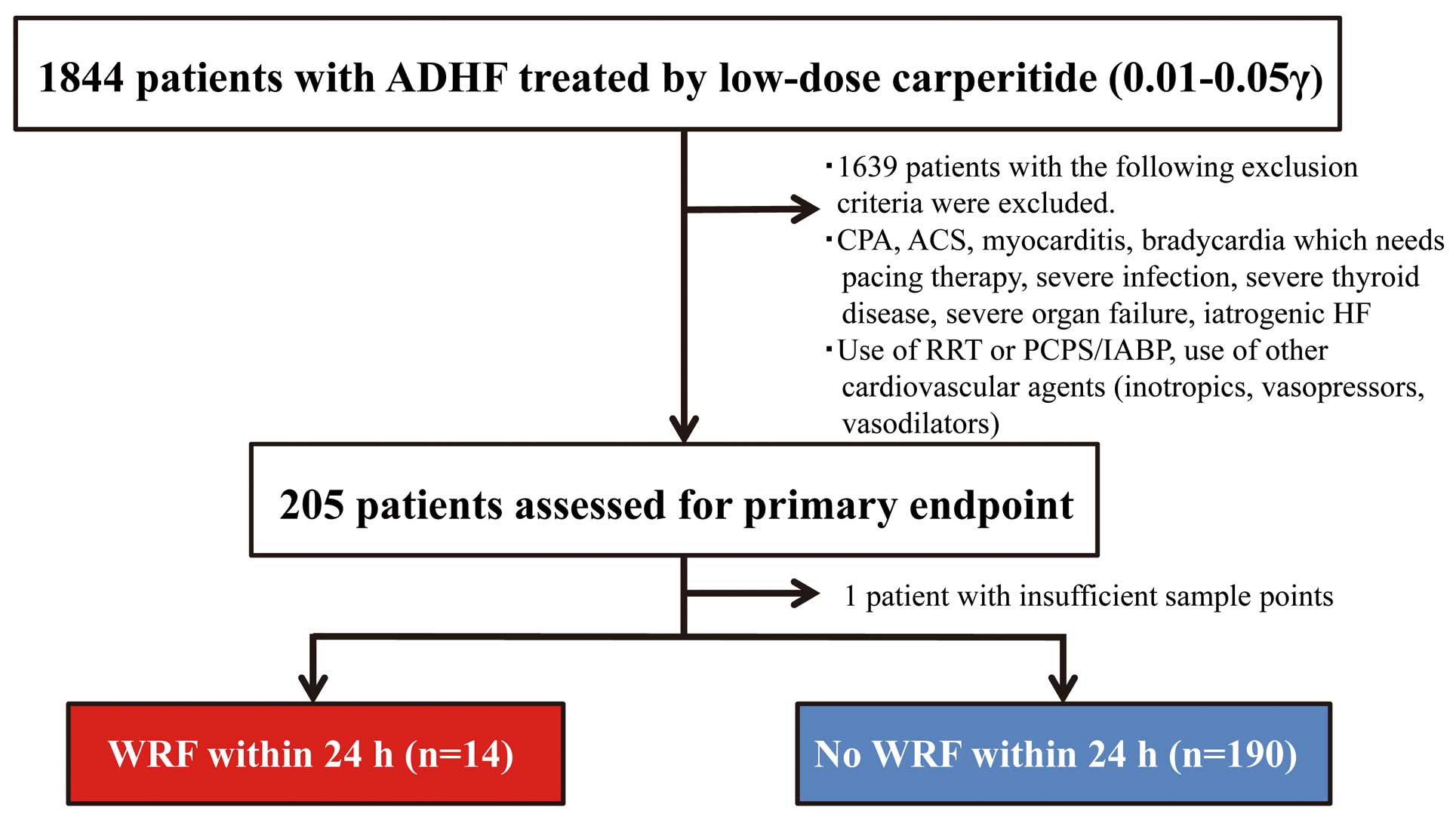
A total of 1,844 consecutive patients were admitted to the coronary care unit of Kurashiki Central Hospital to be treated for ADHF and received low-dose (0.01–0.05 μg/kg/min) carperitide as the initial therapy between January 2006 and April 2014. To clarify the effects of low-dose carperitide therapy by eliminating factors that strongly influence the clinical course, patients with complicated clinical conditions and those who received other types of treatment were excluded on the basis of the following criteria: (1) cardiopulmonary arrest, (2) acute coronary syndrome, (3) myocarditis, (4) severe infection, (5) severe thyroid disease, (6) severe organ failure (excluding HF), (7) iatrogenic HF, (8) use of renal replacement therapy, percutaneous cardiopulmonary support (PCPS), and intra-aortic balloon pumping (IABP), and (9) use of other cardiovascular agents (inotropics, vasopressors and vasodilators). One patient was also excluded because of insufficient sample data, and 204 patients were included in the final analysis (Figure 1). Demographic and clinical data were obtained from medical records. Baseline data included data on age, sex, history of device therapy, use of noninvasive positive pressure ventilation and/or invasive positive pressure ventilation, baseline cardiovascular diseases (ischemic heart disease [IHD], cardiomyopathy [CM], hypertensive heart disease, valvular heart disease [VHD], and others), concomitant diseases (hypertension [blood pressure (BP) ≥140/90 mmHg or a history of hypertension and being on antihypertensive medications], dyslipidemia, diabetes mellitus [DM], atrial fibrillation/flutter, and chronic obstructive pulmonary disease), history of admission for HF, admission laboratory values (hemoglobin/hematocrit levels, serum creatinine level, blood urea nitrogen [BUN] level, serum sodium level, and B-type natriuretic peptide [BNP] level), echocardiographic parameters, admission vital signs (heart rate [HR], systolic BP [SBP], diastolic BP [DBP], and mean BP [MBP]), and medications on admission. For chronic kidney disease, the estimated glomerular filtration rate (eGFR) was calculated on the basis of serum creatinine on admission, age, and sex using the simplified Modification of Diet in Renal Disease equation.12
The clinical characteristics and concomitant diseases were assessed on the basis of independent physician assessment. SBP, DBP, MBP, and HR were measured at baseline and at 1, 3, 6, and 12 h after starting administration of carperitide. For SBP, DBP, and MBP, the lowest values were also measured. Hypotension was defined as SBP <90 mmHg.13
∆BUN/creatinine and ∆hematocrit for 24 h were measured as indexes of hemoconcentration. The primary endpoint of this study was the occurrence of WRF (defined as an increase in serum creatinine ≥0.3 mg/dl from the value on admission) within the first 24 h of low-dose carperitide therapy.4,6,14
The primary endpoint was set within 24 h from the initiation of carperitide therapy because the early phase seemed to be less influenced by other factors and to be suitable for clarifying the effects of low-dose carperitide as the initial therapy. The rates of occurrence of WRF within 24 h classified by hypotension within 12 h and eGFR (cut-off value being 60 ml/min/1.73 m2) were also compared.
Categorical variables are presented as numbers or percentages, and they were compared by using the χ2
test or Fisher’s exact test as appropriate. Continuous variables are presented as mean±standard deviation. Comparisons between groups of continuous variables were made on the basis of the distribution using the t test or Wilcoxon’s rank-sum test. To determine the independent predictors of WRF within 24 h, a logistic regression model was used to estimate the risks associated with the following variables: male sex, history of permanent pacemaker implantation therapy, serum creatinine, BUN, eGFR and occurrence of hypotension within 12 h. Variables with probability values <0.10 in the univariate analysis and for which proportional assumptions were generally fair were included in the multivariate analysis. Differences were considered statistically significant at P<0.05. All analyses were performed using a statistical software package (JMP 9, SAS Institute, Cary, NC, USA).
Results
Baseline Patient Characteristics and In-Hospital Clinical Course
The mean age of the 205 patients was 75.6±12.1 years, and men accounted for 56% of the patients (114 patients). All patients were in NYHA functional class III (15 patients) or IV (190 patients). Baseline characteristics are presented in
Table 1. The mean carperitide dose was 0.03±0.009 μg/kg/min. Baseline cardiovascular diseases were IHD (93 patients, 45%), CM (42 patients, 20%), and VHD (46 patients, 22%); 81 (40%) of the patients had a history of admission for HF. The most common concomitant disease was hypertension (144 patients, 70%). The mean admission BNP level was 997.4±692.7 pg/ml, mean admission serum creatinine level was 1.28±0.72 mg/dl, and mean admission eGFR level was 48.5±22.8 ml/min/1.73 m2. The mean baseline left ventricular ejection fraction was 41.9±15.9%. Mean admission values of SBP, DBP, MBP, and HR were 129.4±18.9 mmHg, 61.8±13.1 mmHg, 84.3±12.6 mmHg, and 87.1±17.8 beats/min, respectively. Among the 205 patients, percutaneous coronary intervention was performed in 24 patients (12%) and cardiac surgery in 14 patients (7%), neither of which were performed within 24 h, and 2 patients (1%) died during hospitalization.
Table 1.
Baseline Characteristics and Demographic Data of All Patients With ADHF
| Variable |
All patients (n=205) |
| Age, years |
75.6±12.1 |
| Men, n (%) |
114 (56) |
| Body mass index* |
22.2±3.8 |
| Baseline cardiovascular diseases |
| Ischemic heart disease, n (%) |
93 (45) |
| Cardiomyopathy, n (%) |
42 (20) |
| Hypertensive heart disease, n (%) |
21 (10) |
| Valvular heart disease, n (%) |
46 (22) |
| Other, n (%) |
3 (1) |
| Concomitant diseases |
| Hypertension, n (%) |
144 (70) |
| Dyslipidemia, n (%) |
80 (39) |
| Diabetes mellitus, n (%) |
76 (37) |
| Atrial fibrillation/flutter, n (%) |
64 (31) |
| Chronic obstructive pulmonary disease, n (%) |
11 (5) |
| Previous admission for heart failure, n (%) |
81 (40) |
| Cardiac devices |
| Permanent pacemaker, n (%) |
8 (4) |
| Implantable cardioverter defibrillator, n (%) |
4 (2) |
| Cardiac resynchronization therapy pacemaker, n (%) |
3 (1) |
| Cardiac resynchronization therapy defibrillator, n (%) |
6 (3) |
| Initial therapy |
| Noninvasive positive pressure ventilation, n (%) |
75 (37) |
| Invasive positive pressure ventilation, n (%) |
10 (5) |
| Carperitide dose, μg/kg/min |
0.03±0.009 |
| Laboratory values on admission |
| Hemoglobin, mg/dl |
11.8±2.8 |
| Hematocrit, % |
36.2±7.8 |
| Cre, mg/dl |
1.28±0.72 |
| BUN, mg/dl |
29.2±18.3 |
| BUN/Cre |
23.3±8.4 |
| eGFR, ml/min/1.73 m2 |
48.5±22.8 |
| eGFR <60 ml/min/1.73 m2, n (%) |
144 (70) |
| Serum sodium, mmol/L |
138.8±3.8 |
| B-type natriuretic peptide, pg/ml |
997.4±692.7 |
| Echocardiographic parameters |
| Left ventricular ejection fraction, % |
41.9±15.9 |
| MR moderate-severe, n (%) |
70 (34) |
| AR moderate-severe, n (%) |
6 (3) |
| AS moderate-severe, n (%) |
16 (8) |
| Baseline hemodynamic data |
| Heart rate, beats/min |
87.1±17.8 |
| Systolic blood pressure, mmHg |
129.4±18.9 |
| Diastolic blood pressure, mmHg |
61.8±13.1 |
| Mean blood pressure, mmHg |
84.3±12.6 |
| Medications on admission |
| Angiotensin-converting enzyme inhibitors, n (%) |
40 (20) |
| Angiotensin-receptor blockers, n (%) |
52 (26) |
| Aldosterone antagonists, n (%) |
37 (18) |
| β-blockers, n (%) |
48 (24) |
| Calcium-channel blockers, n (%) |
83 (41) |
| Nitrates, n (%) |
56 (28) |
| Digoxin, n (%) |
22 (11) |
| Loop diuretics, n (%) |
99 (49) |
*Calculated as weight in kilograms divided by height in meters squared. ADHF, acute decompensated heart failure; AR, aortic regurgitation; AS, aortic stenosis; BUN, blood urea nitrogen; Cre, creatinine; eGFR, estimated glomerular filtration rate; MR, mitral regurgitation.
Changes in SBP, DBP, MBP, and HR over a period of 12 h after starting the administration of carperitide are shown in
Figure 2. Carperitide therapy significantly decreased the mean levels of SBP, DBP, MBP, and HR from baseline for 1 h after administration, and significant decreases continued until 12 h. The mean lowest levels of SBP, DBP, and MBP were 100.7±13.7 mmHg, 47.1±10.5 mmHg, and 65±9.3 mmHg. Hypotension occurred in 40 (20%) of the patients.
Comparison of Groups Based on Occurrence of WRF Within 24 h
WRF within the first 24 h of low-dose carperitide therapy occurred in 14 patients (7%).
Table 2
shows the results of a comparison of patients with and without WRF within 24 h. Univariate analysis showed significant differences between patients with and without WRF within 24 h in admission serum creatinine (2.01±1.13 mg/dl vs. 1.23±0.65 mg/dl, P<0.0001), admission eGFR (33.7±19.3 ml/min/1.73 m2
vs. 49.5±22.7 ml/min/1.73 m2, P=0.0115), and hypotension within 12 h (50% [7/14 patients] vs. 17% [33/190 patients], P=0.008). There were no significant differences between patients with and without WRF within 24 h in baseline cardiovascular diseases, concomitant diseases, indexes of hemoconcentration, echocardiographic parameters, admission SBP (132.6±24.5 mmHg vs. 129.2±18.6 mmHg, P=0.52), urinary output for 12 h (1,464±895 ml vs. 1,820±900 ml P=0.15), or medications on admission. Multivariate adjustment analysis showed that admission serum creatinine (odds ratio [OR], 3.64; 95% confidence interval [CI]: 1.84–7.67, P=0.0003) and hypotension within 12 h (OR, 8.7; 95% CI: 2.38–35.88, P=0.0012) were independent predictors of WRF within the first 24 h of low-dose carperitide therapy in patients hospitalized for ADHF (Table 3).
Table 2.
Demographic Characteristics of ADHF Patients Based on the Occurrence of WRF* Within 24 h
| Variable |
WRF within 24 h (n=14) |
No WRF within 24 h (n=190) |
P value |
| Age, years |
76.2±13.6 |
75.6±12 |
0.85 |
| Men, n (%) |
11 (79) |
103 (54) |
0.097 |
| Body mass index** |
22.5±3.6 |
22.2±3.9 |
0.78 |
| Baseline cardiovascular diseases |
| Ischemic heart disease, n (%) |
7 (50) |
68 (36) |
0.39 |
| Cardiomyopathy, n (%) |
1 (7) |
41 (22) |
0.31 |
| Hypertensive heart disease, n (%) |
3 (21) |
18 (9) |
0.16 |
| Valvular heart disease, n (%) |
3 (21) |
42 (22) |
1.0 |
| Other, n (%) |
0 |
3 (2) |
1.0 |
| Concomitant diseases |
| Hypertension, n (%) |
12 (86) |
131 (69) |
0.24 |
| Dyslipidemia, n (%) |
6 (43) |
74 (39) |
0.78 |
| Diabetes mellitus, n (%) |
7 (50) |
69 (36) |
0.39 |
| Atrial fibrillation/flutter, n (%) |
4 (29) |
59 (31) |
1.0 |
| Chronic obstructive pulmonary disease, n (%) |
2 (14) |
9 (5) |
0.17 |
| Previous admission for heart failure, n (%) |
8 (57) |
72 (38) |
0.17 |
| Cardiac devices |
| Permanent pacemaker, n (%) |
2 (14) |
6 (3) |
0.097 |
| Implantable cardioverter defibrillator, n (%) |
0 |
4 (2) |
1.0 |
| Cardiac resynchronization therapy pacemaker, n (%) |
0 |
3 (2) |
1.0 |
| Cardiac resynchronization therapy defibrillator, n (%) |
0 |
6 (3) |
1.0 |
| Initial therapy |
| Noninvasive positive pressure ventilation, n (%) |
7 (50) |
68 (36) |
0.39 |
| Invasive positive pressure ventilation, n (%) |
2 (14) |
8 (4) |
0.14 |
| Carperitide dose, μg/kg/min |
0.03±0.002 |
0.03±0.001 |
0.94 |
| Laboratory values on admission |
| Hemoglobin, mg/dl |
11.3±2.4 |
11.8±2.8 |
0.52 |
| Hematocrit, % |
35.3±6.8 |
36.3±7.9 |
0.63 |
| Cre, mg/dl |
2.01±1.13 |
1.23±0.65 |
<0.0001 |
| BUN, mg/dl |
38.1±21 |
28.6±18 |
0.059 |
| BUN/Cre |
19.9±4.7 |
23.6±8.5 |
0.11 |
| eGFR, ml/min/1.73 m2 |
33.7±19.3 |
49.5±22.7 |
0.0115 |
| Serum sodium, mmol/L |
139.2±4.0 |
138.7±3.8 |
0.65 |
| ΔBUN/Cre for 24 h |
−0.7±2.4 |
−0.5±4.3 |
0.84 |
| ΔHematocrit for 24 h |
−2.2±3.3 |
−1.5±3.6 |
0.51 |
| B-type natriuretic peptide, pg/ml |
1,039±896.6 |
994±682.6 |
0.83 |
| Echocardiographic parameters |
| Left ventricular ejection fraction, % |
39.5±14.1 |
42±16 |
0.62 |
| MR moderate-severe, n (%) |
3 (21) |
67 (36) |
0.39 |
| AR moderate-severe, n (%) |
0 |
6 (3) |
1.0 |
| AS moderate-severe, n (%) |
0 |
15 (8) |
0.61 |
| Baseline hemodynamic data |
| Heart rate, beats/min |
84.6±23.1 |
87.4±17.4 |
0.58 |
| Systolic blood pressure, mmHg |
132.6±24.5 |
129.2±18.6 |
0.52 |
| Diastolic blood pressure, mmHg |
62.5±16.9 |
61.9±12.7 |
0.87 |
| Mean blood pressure, mmHg |
85.8±17.1 |
84.3±12.3 |
0.68 |
| Lowest systolic blood pressure within 12 h, mmHg |
94.9±21.4 |
101.1±12.9 |
0.104 |
| Occurrence of hypotension*** within 12 h, n (%) |
7 (50) |
33 (17) |
0.008 |
| Urinary output for 12 h, ml |
1,464±895 |
1,820±900 |
0.15 |
| Medications on admission |
| Angiotensin-converting enzyme inhibitors, n (%) |
4 (29) |
36 (19) |
0.49 |
| Angiotensin-receptor blockers, n (%) |
2 (14) |
49 (26) |
0.53 |
| Aldosterone antagonists, n (%) |
1 (7) |
36 (19) |
0.47 |
| β-blockers, n (%) |
6 (43) |
42 (23) |
0.11 |
| Calcium-channel blockers, n (%) |
7 (50) |
75 (40) |
0.58 |
| Nitrates, n (%) |
5 (36) |
51 (27) |
0.54 |
| Digoxin, n (%) |
3 (21) |
19 (10) |
0.19 |
| Loop diuretics, n (%) |
9 (64) |
89 (48) |
0.28 |
*Defined as an increase in Cre ≥0.3 mg/dl. **Calculated as weight in kilograms divided by height in meters squared. ***Defined as systolic blood pressure <90 mmHg. WRF, worsening renal function. Other abbreviations as in Table 1.
Table 3.
Univariate and Multivariate Analyses of Predictors of WRF* Within 24 h After Starting Low-Dose Carperitide
| Variable |
Univariate OR
(95% CI) |
P value |
Multivariate OR
(95% CI) |
P value |
| Men |
3.10 (0.84–11.5) |
0.097 |
2.50 (0.67–12.2) |
0.18 |
| Permanent pacemaker |
5.11 (0.93–28.1) |
0.097 |
5.39 (0.63–35.6) |
0.11 |
| Cre |
2.73 (1.54–4.94) |
0.0009 |
3.64 (1.84–7.67) |
0.0003 |
| BUN |
1.02 (1.00–1.05) |
0.085 |
|
|
| eGFR |
0.96 (0.93–0.99) |
0.006 |
|
|
| Occurrence of hypotension** within 12 h |
4.76 (1.56–14.5) |
0.008 |
8.70 (2.38–35.9) |
0.0012 |
*Defined as an increase in Cre ≥0.3 mg/dl. **Defined as systolic blood pressure <90 mmHg. CI, confidence interval; OR, odds ratio. Other abbreviations as in Tables 1,2.
As shown in
Figure 3, in patients with eGFR <60 ml/min/1.73 m2, the rate of WRF occurrence was significantly higher in those complicated by hypotension than in those without hypotension (22.6% [7/31 patients] vs. 4.4% [5/113 patients], P=0.0041). In contrast, in patients with eGFR ≥60 ml/min/1.73 m2, hypotension did not influence the occurrence of WRF (0% [0/9 patients] vs. 3.9% [2/51 patients], P=NS). There was no difference in the rate of WRF occurrence between patients with eGFR ≥60 ml/min/1.73 m2
with or without hypotension and patients with eGFR <60 ml/min/1.73 m2
without hypotension (3.3% [2/60 patients] vs. 4.4% [5/113 patients], P=NS).
Predictors of the Occurrence of Hypotension Within 12 h After Starting Administration of Low-Dose Carperitide
Table 4
shows the results of a comparison of patients with and without the occurrence of hypotension within 12 h after starting administration of carperitide. Univariate analysis showed significant differences between patients with and without the occurrence of hypotension within 12 h in the use of invasive positive pressure ventilation (13% [5/40 patients] vs. 3% [5/164 patients], P=0.027), moderate to severe mitral regurgitation (20% [8/40 patients] vs. 38% [62/164 patients], P=0.04), and baseline SBP (115.4±19.5 mmHg vs. 132.9±17.3 mmHg, P<0.0001). Multivariate adjustment analysis showed that moderate to severe mitral regurgitation (OR, 0.38; 95% CI: 0.14–0.90, P=0.026) and baseline SBP ≤110 mmHg (the cut-off value of baseline SBP calculated using receiver-operating characteristic curve [area under the curve=0.76] was 112 mmHg; OR, 7.61; 95% CI: 3.34–17.83, P<0.0001) were independent predictors of the occurrence of hypotension within 12 h after starting administration of low-dose carperitide in patients hospitalized for ADHF (Table 5).
Table 4.
Demographic Characteristics of ADHF Patients Based on the Occurrence of Hypotension* Within 12 h After Starting Low-Dose Carperitide
| Variable |
Hypotension within
12 h (n=40) |
No hypotension within
12 h (n=164) |
P value |
| Age, years |
76.6±13.8 |
75.4±11.7 |
0.58 |
| Men, n (%) |
20 (50) |
94 (57) |
0.48 |
| Body mass index** |
21.8±4.2 |
22.3±3.7 |
0.45 |
| Baseline cardiovascular diseases |
| Ischemic heart disease, n (%) |
19 (48) |
74 (45) |
0.86 |
| Cardiomyopathy, n (%) |
6 (15) |
36 (22) |
0.39 |
| Hypertensive heart disease, n (%) |
3 (8) |
18 (11) |
0.77 |
| Valvular heart disease, n (%) |
12 (30) |
33 (20) |
0.20 |
| Other, n (%) |
0 |
3 (2) |
1.0 |
| Concomitant diseases |
| Hypertension, n (%) |
26 (65) |
117 (71) |
0.45 |
| Dyslipidemia, n (%) |
20 (50) |
60 (37) |
0.15 |
| Diabetes mellitus, n (%) |
12 (30) |
64 (39) |
0.36 |
| Atrial fibrillation/flutter, n (%) |
8 (20) |
55 (34) |
0.13 |
| Chronic obstructive pulmonary disease, n (%) |
3 (8) |
8 (5) |
0.45 |
| Previous admission for heart failure, n (%) |
15 (38) |
65 (40) |
0.86 |
| Cardiac devices |
| Permanent pacemaker, n (%) |
2 (5) |
6 (4) |
0.66 |
| Implantable cardioverter defibrillator, n (%) |
0 |
4 (2) |
1.0 |
| Cardiac resynchronization therapy pacemaker, n (%) |
1 (3) |
2 (1) |
0.48 |
| Cardiac resynchronization therapy defibrillator, n (%) |
0 |
6 (4) |
0.60 |
| Initial therapy |
| Noninvasive positive pressure ventilation, n (%) |
15 (38) |
60 (37) |
1.0 |
| Invasive positive pressure ventilation, n (%) |
5 (13) |
5 (3) |
0.027 |
| Carperitide dose, μg/kg/min |
0.03±0.009 |
0.03±0.009 |
0.88 |
| Laboratory values on admission |
| Hemoglobin, mg/dl |
12.0±2.4 |
11.7±2.8 |
0.57 |
| Hematocrit, % |
36.9±7.0 |
36.1±8.0 |
0.58 |
| Cre, mg/dl |
1.23±0.54 |
1.30±0.76 |
0.56 |
| BUN, mg/dl |
27.1±13.6 |
29.8±19.2 |
0.40 |
| BUN/Cre |
22.7±7.5 |
23.5±8.6 |
0.61 |
| eGFR, ml/min/1.73 m2 |
48.3±26.3 |
48.5±22.0 |
0.95 |
| Serum sodium, mmol/L |
138.3±3.2 |
138.9±4.0 |
0.34 |
| B-type natriuretic peptide, pg/ml |
949.8±643.2 |
1007.9±707.5 |
0.64 |
| Echocardiographic parameters |
| Left ventricular ejection fraction, % |
40.3±14.1 |
42.2±16.3 |
0.52 |
| MR moderate-severe, n (%) |
8 (20) |
62 (38) |
0.04 |
| AR moderate-severe, n (%) |
0 |
6 (4) |
0.60 |
| AS moderate-severe, n (%) |
5 (13) |
10 (6) |
0.18 |
| Baseline hemodynamic data |
| Heart rate, beats/min |
88.8±17.0 |
86.8±18.0 |
0.52 |
| Systolic blood pressure, mmHg |
115.4±19.5 |
132.9±17.3 |
<0.0001 |
| Diastolic blood pressure, mmHg |
61.0±12.8 |
62.2±13.1 |
0.59 |
| Mean blood pressure, mmHg |
79.0±13.8 |
85.7±12.0 |
0.0023 |
| Medications on admission |
| Angiotensin-converting enzyme inhibitors, n (%) |
9 (23) |
31 (19) |
0.66 |
| Angiotensin-receptor blockers, n (%) |
8 (20) |
43 (27) |
0.42 |
| Aldosterone antagonists, n (%) |
8 (20) |
29 (18) |
0.82 |
| β-blockers, n (%) |
9 (23) |
39 (24) |
1.0 |
| Calcium-channel blockers, n (%) |
12 (30) |
70 (44) |
0.15 |
| Nitrates, n (%) |
12 (30) |
44 (28) |
0.84 |
| Digoxin, n (%) |
6 (15) |
16 (10) |
0.40 |
| Loop diuretics, n (%) |
21 (53) |
77 (48) |
0.72 |
*Defined as systolic blood pressure <90 mmHg. **Calculated as weight in kilograms divided by height in meters squared. Abbreviations as in Table 1.
Table 5.
Univariate and Multivariate Analyses of Predictors of the Occurrence of Hypotension* Within 12 h After Starting Low-Dose Carperitide
| Variable |
Univariate OR
(95% CI) |
P value |
Multivariate OR
(95% CI) |
P value |
| Invasive positive pressure ventilation |
4.54 (1.25–16.5) |
0.027 |
2.09 (0.44–9.90) |
0.35 |
| MR moderate-severe |
0.40 (0.17–0.93) |
0.04 |
0.38 (0.14–0.90) |
0.026 |
| Baseline SBP ≤110 mmHg |
7.63 (3.49–16.7) |
0.008 |
7.61 (3.34–17.8) |
<0.0001 |
*Defined as systolic blood pressure <90 mmHg. Abbreviations as in Tables 1,3.
Discussion
In the present study, WRF within the first 24 h of low-dose carperitide therapy occurred in 14 patients (7%). Possible reasons for the low incidence of WRF in this study are the short observation period from the start of treatment and the study population with relatively low severities, which might have been related to the exclusion of patients with complicated pathological conditions and those requiring cardiotonic agents or IABP/PCPS.
We found that the serum creatinine level on admission (OR, 3.64; 95% CI: 1.84–7.67, P=0.0003) and hypotension within 12 h (OR, 8.7; 95% CI: 2.38–35.88, P=0.0012) were independent predictors of WRF within the first 24 h of low-dose carperitide therapy in patients hospitalized for ADHF. The ASCEND-HF was a study conducted on the basis of several contradictory reports on the effects of nesiritide on renal function in patients with ADHF.15
The effects of nesiritide are similar to those of carperitide. However, in the ASCEND-HF, nesiritide did not affect renal function in patients with ADHF and, furthermore, a multivariable-adjusted subanalysis showed no significant relationship between hypotension in the first 48 h of randomization and serum creatinine level at discharge or day 10.13,15
The results of the present study differed from those of the ASCEND-HF and might be related to differences in the pharmacological properties of carperitide and nesiritide, effects of concomitant drugs such as the cardiotonic agents used in the ASCEND-HF, or the definition of WRF. In the present study, WRF was defined as an increase in serum creatinine ≥3 mg/dl from the value on admission and it was measured within 24 h from the initiation of carperitide therapy, whereas in the ASCEND-HF, it was defined as a >25% decrease in eGFR and was measured from study-drug initiation through to day 30. The difference in results might also be related to differences in baseline renal function of the study population. The mean admission eGFR was 48.5±22.8 ml/min/1.73 m2
in the present study but approximately 60 ml/min/1.73 m2
in the ASCEND-HF. In the present study, hypotension influenced the occurrence of WRF in patients with eGFR <60 ml/min/1.73 m2
but not in those with eGFR ≥60 ml/min/1.73 m2. On the other hand, it is noteworthy that the occurrence of WRF showed no significant difference between patients with eGFR ≥60 ml/min/1.73 m2
(with or without hypotension) and those with eGFR <60 ml/min/1.73 m2
without hypotension. Thus, when treating ADHF with carperitide, hypotension should be carefully avoided in patients with eGFR <60 ml/min/1.73 m2. DM is widely considered as a risk factor of renal injury, but in the present study, it had no effect on the outcomes, possibly because of the small number of patients.
Independent predictors of the occurrence of hypotension within 12 h after starting administration of low-dose carperitide in patients hospitalized for ADHF were moderate to severe mitral regurgitation (OR, 0.38; 95% CI: 0.14–0.90, P=0.026) and baseline SBP ≤110 mmHg (OR, 7.61; 95% CI: 3.34–17.83, P<0.0001). BNP, ejection fraction, and renal function on admission had no effect on the outcomes, indicating that low-dose carperitide can be used safely regardless of the severities of cardiac and renal function because it is not likely to increase the risk of hypotension. The reason why hypotension was rare in patients with moderate to severe mitral regurgitation may be because cardiac output increased after the regurgitant volume decreased due to the effect of carperitide on cardiac afterload reduction.
Study Limitations
The main limitation of the present study is its retrospective design, which is prone to inherent bias. In addition, the number of patients was small. Strict exclusion criteria to clarify the effects of low-dose carperitide therapy resulted in a small study population by eliminating patients with factors that could strongly influence the clinical course, such as complicated clinical conditions and intervention with other types of treatment, and its appropriateness was not elucidated. The primary endpoint of the present study was WRF within 24 h after starting the administration of carperitide, because the early phase seemed to be less influenced by other factors and to be suitable for clarifying the effects of low-dose carperitide as the initial therapy; however, whether it was an appropriate endpoint or not was not elucidated. As in a number of preceding studies, WRF was defined as a change in serum creatinine level. Evaluation including a change in eGFR might be more accurate. We did not evaluate risk factors for renal dysfunction, such as hypoxia and low cardiac output, because of insufficient data. Ejection fraction did not affect the occurrence of hypotension; however, its effect on cardiac output was not evaluated. Survival analysis was not conducted, because of the small number of patients and the low follow-up rate after discharge. Further prospective studies with a larger study population including survival analysis are needed to reveal the relationship between low-dose carperitide and WRF in patients with ADHF.
Conclusions
Hypotension within 12 h after starting administration of carperitide and renal dysfunction on admission are independent predictors of WRF within 24 h in patients with ADHF treated by low-dose carperitide. Hypotension may not cause WRF in patients with eGFR ≥60 ml/min/1.73 m2.
Acknowledgments
We are grateful to Miho Kobayashi for writing assistance.
References
- 1.
Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, et al. Renal impairment and outcomes in heart failure: Systematic review and meta-analysis. J Am Coll Cardiol 2006; 47: 1987–1996.
- 2.
Neves FM, Meneses GC, Sousa NE, Menezes RR, Parahyba MC, Martins AM, et al. Syndecan-1 in acute decompensated heart failure: Association with renal function and mortality. Circ J 2015; 79: 1511–1519.
- 3.
Damman K, Valente MA, Voors AA, O’Connor CM, van Veldhuisen DJ, Hillege HL. Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur Heart J 2014; 35: 455–469.
- 4.
Kociol RD, Greiner MA, Hammill BG, Phatak H, Fonarow GC, Curtis LH, et al. Long-term outcomes of medicare beneficiaries with worsening renal function during hospitalization for heart failure. Am J Cardiol 2010; 105: 1786–1793.
- 5.
Metra M, Nodari S, Parrinello G, Bordonali T, Bugatti S, Danesi R, et al. Worsening renal function in patients hospitalised for acute heart failure: Clinical implications and prognostic significance. Eur J Heart Fail 2008; 10: 188–195.
- 6.
Voors AA, Davison BA, Felker GM, Ponikowski P, Unemori E, Cotter G, et al; Pre-RELAX-AHF study group. Early drop in systolic blood pressure and worsening renal function in acute heart failure: Renal results of Pre-RELAX-AHF. Eur J Heart Fail 2011; 13: 961–967.
- 7.
Hata N, Seino Y, Tsutamoto T, Hiramitsu S, Kaneko N, Yoshikawa T, et al. Effects of carperitide on the long-term prognosis of patients with acute decompensated chronic heart failure: The PROTECT multicenter randomized controlled study. Circ J 2008; 72: 1787–1793.
- 8.
Sezai A, Nakata K, Iida M, Yoshitake I, Wakui S, Hata H, et al. Results of low-dose carperitide infusion in high-risk patients undergoing coronary artery bypass grafting. Ann Thorac Surg 2013; 96: 119–126.
- 9.
Kitakaze M, Asakura M, Kim J, Shintani Y, Asanuma H, Hamasaki T, et al; J-WIND investigators. Human atrial natriuretic peptide and nicorandil as adjuncts to reperfusion treatment for acute myocardial infarction (J-WIND): Two randomised trials. Lancet 2007; 370: 1483–1493.
- 10.
Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, et al; ATTEND Investigators. Clinical features and outcome in hospitalized heart failure in Japan (from the ATTEND Registry). Circ J 2013; 77: 944–951.
- 11.
Dohi K, Ito M. Novel diuretic strategies for the treatment of heart failure in Japan. Circ J 2014; 78: 1816–1823.
- 12.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999; 130: 461–470.
- 13.
Patel PA, Heizer G, O’Connor CM, Schulte PJ, Dickstein K, Ezekowitz JA, et al. Hypotension during hospitalization for acute heart failure is independently associated with 30-day mortality: Findings from ASCEND-HF. Circ Heart Fail 2014; 7: 918–925.
- 14.
Yamazoe M, Mizuno A, Nishi Y, Niwa K, Isobe M. Serum alkaline phosphatase as a predictor of worsening renal function in patients with acute decompensated heart failure. J Cardiol
2015 September 9, doi:10.1016/j.jjcc.2015.08.004.
- 15.
van Deursen VM, Hernandez AF, Stebbins A, Hasselblad V, Ezekowitz JA, Califf RM, et al. Nesiritide, renal function, and associated outcomes during hospitalization for acute decompensated heart failure: Results from the Acute Study of Clinical Effectiveness of Nesiritide and Decompensated Heart Failure (ASCEND-HF). Circulation 2014; 130: 958–965.


