Images in Cardiovascular Medicine
Lethal Cement Leakage Embolization After Kyphoplasty
2017 Volume 81 Issue 1 Pages 119-120

Details
2017 Volume 81 Issue 1 Pages 119-120
A 49-year-old man, who had a history of stent implantation in the right coronary artery (RCA), was referred for chest pain. Five days before this admission, the patient had undergone percutaneous kyphoplasty of the L5 vertebral body due to compression fracture in other facility. Antiplatelet agents were stopped 1 week before percutaneous kyphoplasty.
Echocardiography showed decreased left ventricular systolic function with regional wall motion abnormalities in the territory of the RCA. There was a hyperechoic linear mass in the right atrium (RA) and right ventricle (RV). The mass seemed to penetrate the RV (Figure 1A). Although the inferior vena cava (IVC) and the opening of the IVC were evaluated, there was no evidence of mass or thrombus in the IVC. The mass origin was uncertain. Coronary angiography showed total occlusion due to thrombosis at the previous stented site. Fluoroscopy showed a radiopaque linear mass in the RV (Figure 1B).
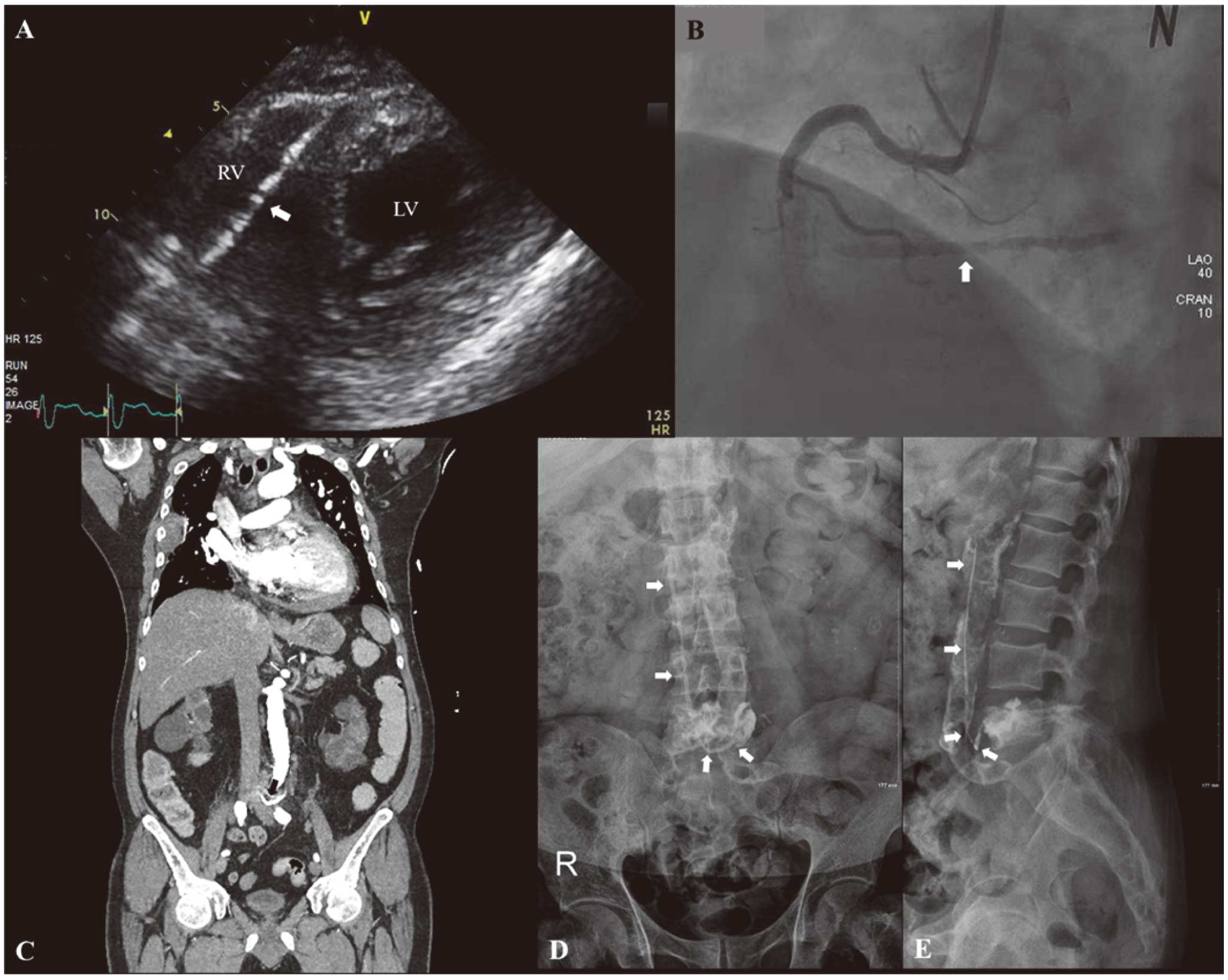
(A) Echocardiography showed a linear hyperechoic mass (arrow) within the right atrium and ventricle (RV). The mass seemed to penetrate the RV. (B) Fluoroscopy during coronary angiography showed a radiopaque linear mass (arrow) in the RV. (C) Computed tomography indicated an approximately 3-cm radiopaque linear mass (arrow) in the lumbar segmental vein, extending from the L5 vertebral body. (D,E) Immediate post-kyphoplasty radiograph showing a radiopaque linear mass (arrow), originating from the lumbar body and extending to the inferior vena cava through the lumbar segmental vein. LV, left ventricle.
Computed tomography indicated an approximately 3-cm radiopaque linear mass in the lumbar segmental vein (Figure 1C). The mass extended from the L5 vertebral body. To confirm the etiology of the intracardiac mass, previous medical records were reviewed. Immediate post-kyphoplasty radiography was reviewed (Figure 1D,E). Anteroposterier and lateral views of the lumbar spine showed a fractured, cement-filled lumbar body. A radiopaque linear mass originated from the lumbar body and extended to the IVC through the lumbar segmental vein. The mass measured approximately 15 cm. The leakage of bone cement from the cement-filled lumbar body seemed to form the linear mass in the IVC. The intracardiac mass was suspected to be fragmented and embolized bone cement from the previous IVC mass.
The patient was taken urgently to the operating room for foreign body removal and coronary bypass graft. After median sternotomy, a pointed mass was identified. The tip of the mass penetrated the RV apex and had torn the pericardium and pleura (Figure 2A). Another tip, located in the RA, had abraded the RA wall and tricuspid leaflet without rupture (Figure 2B). A 10-cm rigid pointed mass was extracted (Figure 2C). The mass was confirmed to be fragmented and embolized methyl methacrylate used in percutaneous kyphoplasty.

(A) After median sternotomy, the tip of a mass, penetrating the apex of the right ventricle (RV) and tearing the pericardium and pleura, was found. (B) The mass was located in the right atrium (RA) and RV, causing RV perforation and RA wall and tricuspid leaflet abrasion without rupture. (C) A 10-cm rigid pointed mass was extracted.
Percutaneous kyphoplasty has been widely used for treatment of compression fracture.1,2 Although methyl methacrylate is injected into the vertebral body, and solidifies within a short time, there is always a risk of vascular leakage into the systemic circulation before solidification.2,3 In the present case, unsolidified methyl methacrylate had leaked into the venous system and formed the rigid rod-like bone cement in the IVC. After solidification, it had fragmented and embolized to the right heart, resulting in cardiac perforation. Fortunately, embolized methyl methacrylate had obstructed the penetrated hole and delayed cardiac rupture. Cardiac perforation due to embolized methyl methacrylate is an extremely rare complication of percutaneous kyphoplasty, but a possible emergency case.
In the present case, immediate post-kyphoplasty radiography clearly showed the migration route of the methyl methacrylate. Post-kyphoplasty radiography might provide information for predicting high-risk vascular or cardiac complications. The present case suggests that close observation is needed and that risk of cardiac complications should be considered in the case of suspected vascular leakage of methyl methacrylate into the systemic circulation after percutaneous kyphoplasty.
None.