Abstract
Background:
Although there have been several reports on the risk factors associated with intima-media thickness (IMT), many questions remain. The purpose of this study was to investigate the association between IMT and cardiovascular risk factors in a Japanese general population.
Methods and Results:
The study group consisted of 1,583 male subjects undergoing routine health checkups. IMT of the common carotid artery was measured by high-resolution ultrasonography. Brachial-ankle pulse wave velocity (baPWV) was measured using an automated device. Univariate analysis demonstrated that carotid IMT significantly associated with age, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), baPWV, fasting glucose, low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C). Multiple logistic regression analysis for carotid atherosclerosis (carotid IMT ≥1.0 mm) was performed using obesity (BMI ≥25.0 kg/m2), high BP (SBP ≥130 mmHg or DBP ≥85 mmHg), dyslipidemia (LDL-C ≥140 mg/dL, TG ≥150 mg/dL, or HDL-C <40 mg/dL), impaired fasting glucose (IFG) (fasting glucose ≥110 g/dL), and high baPWV (≥1,400 cm/s). Carotid atherosclerosis was significantly associated with only high baPWV (OR: 2.22, 95% CI: 1.24–4.17, P<0.01).
Conclusions:
High baPWV was a stronger predictor of early carotid atherosclerosis than high BP, dyslipidemia, or IFG in a Japanese general male population.
Carotid intima-media thickness (IMT) is a commonly used direct assessment of early atherosclerosis, and an increased value has been associated with both the prevalence and incidence of coronary artery disease and stroke.1–3
It has been reported that carotid IMT is associated with several cardiovascular risk factors, including diabetes mellitus, hypertension, hypercholesterolemia, and obesity.4
Although measurement of IMT is a simple and noninvasive examination using high-resolution B-mode ultrasound, a skilled technician is needed to evaluate IMT accurately.
Editorial p 304
On the other hand, pulse wave velocity (PWV) has been conventionally used as an index of arterial stiffness.5,6
Arterial stiffness evaluated by aortic PWV is an independent predictor of cardiovascular death in patients with essential hypertension.7
Although conventional techniques for measuring PWV are noninvasive, the femoral artery transducer must be carefully adjusted to obtain an accurate pulse wave, which increases the psychological stress for patients. Such sophisticated and complex techniques are inconvenient, particularly in large clinical trials.
A simple, noninvasive, and automatic method of measuring the brachial-ankle PWV (baPWV) has been developed, and a strong correlation between it and aortic PWV has been reported.8,9
The baPWV has also been shown to be a predictor of cardiovascular events10
and death.11
Furthermore, a higher baPWV has been independently associated with all-cause death and vascular death in patients with acute stroke.12
In addition, it has been reported that IMT and baPWV, especially when combined, are useful in predicting future vascular events in elderly subjects.13
However, there is no report of the relationship between baPWV and IMT in the general population as far as we know.
The purpose of this study was to investigate the association between carotid IMT and cardiovascular risk factors including baPWV in a Japanese general population.
Methods
Study Population
The study group consisted of 1,583 male subjects undergoing routine health checkups. IMT of the common carotid artery was measured by high-resolution ultrasonography. The baPWV and blood pressure (BP) were measured using automated devices.12
The exclusion criterion of this study was peripheral artery disease or atrial fibrillation. There were no subjects with ankle brachial index <0.9 or >1.4. The protocol used for the study was approved by the institutional review board of Kagoshima University, named the Ethics Committee on Epidemiological Studies, and the approved number of this study was 258. Informed consent was given by all volunteers.
Laboratory Analysis
Blood samples were collected after the subjects had fasted overnight. The serum concentrations of total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), fasting glucose (FG), hemoglobin A1c, uric acid, and creatinine were measured by standard laboratory procedures, while low-density lipoprotein cholesterol (LDL-C) was calculated by Friedewald’s equation. LDL-C was not estimated in 8 subjects whose serum TG concentrations were ≥400 mg/dL, as Friedewald’s equation is unreliable in such cases.
Definition of Cardiovascular Risk Factors
Obesity was defined as a body mass index (BMI) ≥25.0 kg/m2.14
High BP was defined as a systolic BP (SBP) ≥130 mmHg, or a diastolic BP (DBP) ≥85 mmHg.15
Dyslipidemia was identified by LDL-C ≥140 mg/dL, TG ≥150 mg/dL, or HDL-C <40 mg/dL.16
Impaired FG (IFG) was defined as FG ≥110 mg/dL.15
Chronic kidney disease (CKD) was evaluated by eGFR using the following equation: eGFR=194×Cr−1.094×age−0.287
(mL/min/1.73 m2).17
CKD was defined as eGFR <60 mL/min/1.73 m2.18
Measurement of PWV and BP
The baPWV was measured as reported previously,8,9
and automatically calculated with the use of a Colin Waveform Analyzer (Colin, Komaki, Japan) according to the following equation: baPWV=(D1−D2)/T1, where
D1 is the distance from the aortic root to the right ankle, and
D2 is the distance from the heart to the right upper arm. These distances were calculated automatically on the basis of the subject’s height.
T1 is the time from the onset of the rise in pulse volume record of the right upper arm to the onset of the rise in pulse volume record of the right ankle. BP of the extremity was measured automatically by the Colin Waveform Analyzer when baPWV was measured, and we used the right brachial BP for statistical analysis. baPWV >14.0 m/s is an independent variable for risk stratification by Framingham score and for the discrimination of patients with atherosclerotic cardiovascular disease.19
Therefore, high baPWV was defined as a baPWV >1,400 cm/s.
Measurement of IMT
IMT imaging of the common carotid artery was performed using high-resolution B-mode ultrasonography (Vivid 7, GE Ultrasound, Solingen, Germany) with a 10-MHz linear array transducer. Bifurcation of the common carotid artery was confirmed, and IMT was measured from the far wall of the distal common carotid arteries over the distance to within 10 mm proximal to the bifurcation. Three points on the bilateral common carotid arteries without plaque were measured, and IMT was defined as the mean IMT value of the left and right common carotid arteries.
Statistical Analysis
Data are expressed as mean±SD. The relationship between continuous variables was analyzed by linear regression analysis. The independence of the association between variables was tested by multiple regression analysis. Statistical analyses were performed with JMP pro 11, while calculation of the partial contribution ratio (partial R2) in multiple regression analysis was performed with SPSS version 23. P<0.05 was considered statistically significant.
Results
The clinical characteristics of the subjects are shown in
Table 1. Mean values for age, BMI, SBP, DBP, baPWV and IMT were 56±10 years, 24±3 kg/cm2, 125±17 mmHg, 80±11 mmHg, 1,531±328 cm/s and 0.78±0.13 mm, respectively.
Table 1.
Characteristics of the Japanese Male Subjects (n=1,583)
| Variables |
|
| Age (years) |
56±10 |
| Height (cm) |
166±6 |
| Weight (kg) |
67±10 |
| BMI (kg/cm2) |
24±3 |
| TG (mg/dL) |
146±136 |
| HDL-C (mg/dL) |
55±14 |
| LDL-C (mg/dL) |
131±33 |
| Fasting blood sugar (mg/dL) |
109±22 |
| Hemoglobin A1c (%) |
5.3±0.7 |
| Creatinine (mg/dL) |
0.8±0.3 |
| eGFR (mL/min/1.73m2) |
78±15 |
| Uric acid (mg/dL) |
6.0±1.2 |
| SBP (mmHg) |
125±17 |
| DBP (mmHg) |
80±11 |
| Smoking history (%) |
29 |
| baPWV (cm/s) |
1,531±328 |
| IMT (mm) |
0.78±0.13 |
baPWV, brachial-ankle pulse wave velocity; BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; IMT, intima-media thickness; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides.
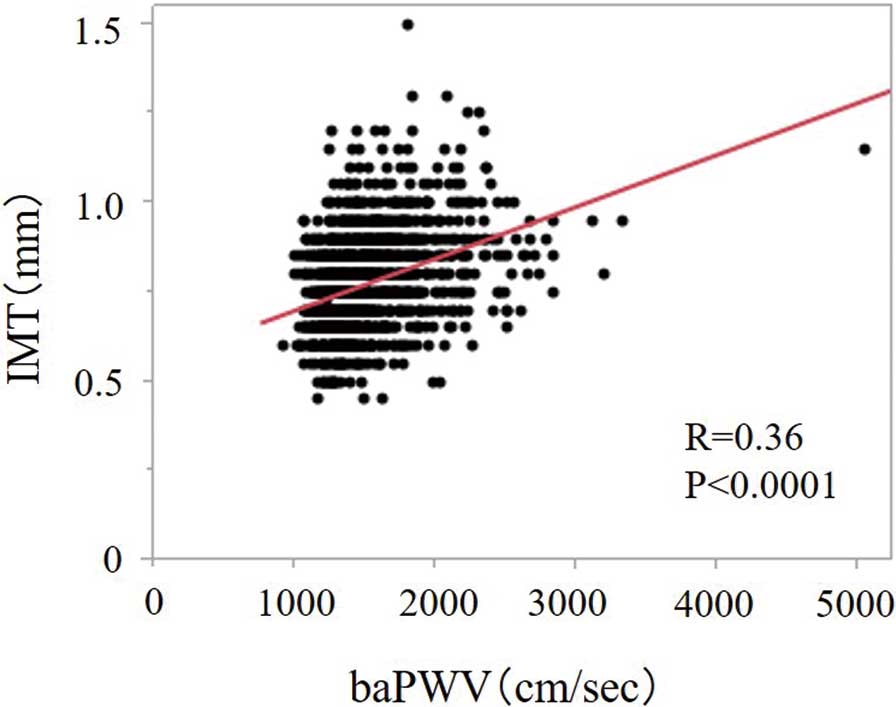
Univariate analysis demonstrated that carotid IMT was significantly associated with age, BMI, SBP, DBP, baPWV, FG, LDL-C, TG, eGFR, and smoking history (Table 2). Age and baPWV showed stronger correlations with carotid IMT than did the other variables (Figure 1). Multiple regression analysis was performed using IMT as the dependent variable, and conventional atherosclerotic risk factors, such as age, BMI, TG, HDL-C, LDL-C, fasting blood sugar, SBP, DBP, eGFR, smoking history and baPWV as independent variables. This revealed that IMT was independently related to age, BMI, TG, LDL-C, FBS, SBP, smoking history and baPWV (Table 3).
Table 2.
Univariate Linear Regression Analysis of IMT With Risk Factors
| |
r |
P value |
| Age |
0.427 |
<0.0001 |
| BMI |
0.137 |
<0.0001 |
| TG |
−0.080 |
<0.005 |
| HDL-C |
−0.038 |
NS |
| LDL-C |
0.063 |
<0.05 |
| Fasting blood sugar |
0.117 |
<0.0001 |
| SBP |
0.286 |
<0.0001 |
| DBP |
0.093 |
<0.0005 |
| eGFR |
−0.133 |
<0.0001 |
| Smoking history |
−0.070 |
<0.01 |
| baPWV |
0.360 |
<0.0001 |
BMI, body mass index; NS, not significant. Other abbreviations as in Table 1.
Table 3.
Multiple Regression Analysis of IMT and Risk Factors
| |
R2 |
β |
P value |
| Age |
0.295 |
0.360 |
<0.0001 |
| BMI |
0.158 |
0.156 |
<0.0001 |
| TG |
−0.051 |
−0.050 |
<0.05 |
| HDL-C |
−0.038 |
−0.037 |
NS |
| LDL-C |
0.088 |
0.077 |
<0.005 |
| Fasting blood sugar |
0.084 |
0.075 |
<0.005 |
| SBP |
0.070 |
0.097 |
<0.01 |
| DBP |
0.001 |
0.001 |
NS |
| eGFR |
−0.003 |
−0.003 |
NS |
| Smoking history |
0.080 |
0.072 |
<0.005 |
| baPWV |
0.109 |
0.133 |
<0.0001 |
Abbreviations as in Tables 1,2.
In addition, multiple logistic regression analysis for carotid atherosclerosis, defined as carotid IMT ≥1.0 mm was performed using obesity, high BP, dyslipidemia, IFG, CKD, smoking history, and high baPWV (≥1,400 cm/s). After adjustment for age, carotid atherosclerosis was significantly associated with only high baPWV (odds ratio (OR): 2.22, 95% confidence interval (CI): 1.24–4.17, P<0.01) (Table 4).
Table 4.
Multiple Logistic Regression Analysis for Carotid Atherosclerosis After Adjustment for Age
| Variables |
OR |
95% CI |
P value |
| Obesity |
1.29 |
0.84–1.97 |
NS |
| Dyslipidemia |
0.77 |
0.48–1.19 |
NS |
| IFG |
1.39 |
0.92–2.08 |
NS |
| High blood pressure |
1.51 |
0.97–2.38 |
NS |
| Smoking history |
1.49 |
0.91–2.38 |
NS |
| CKD |
1.00 |
0.99–1.01 |
NS |
| High baPWV |
2.22 |
1.24–4.17 |
<0.01 |
CI, confidence interval; CKD, chronic kidney disease; IFG, impaired fasting glucose; OR, odds ratio. Other abbreviations as in Tables 1,2.
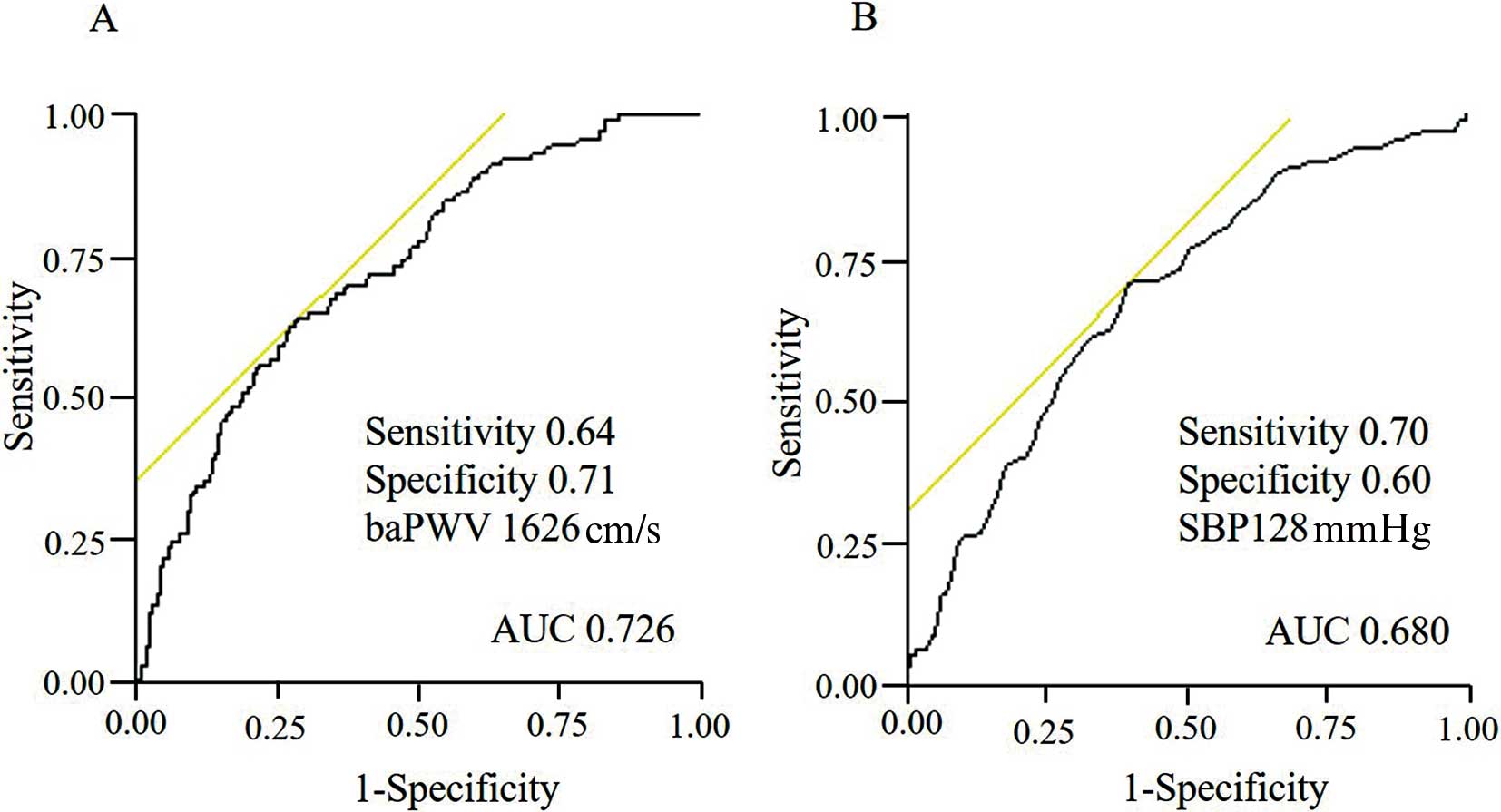
Figure 2
shows the receiver-operator characteristics curve between baPWV or SBP and carotid atherosclerosis (carotid IMT ≥1.0 mm). The area under the curve was 0.73, and the sensitivity and specificity were 0.64 and 0.73, respectively, at baPWV=1,626 cm/s. When SBP was 128 mmHg, the area under the curve was 0.68, and the respective sensitivity and specificity were 0.70 and 0.60.
Discussion
We found that carotid IMT was significantly associated with age, BMI, SBP, DBP, baPWV, FG, LDL-C, TG, eGFR and smoking history in the univariate analysis. Multiple regression analysis demonstrated that IMT was independently correlated with age, BMI, LDL-C, TG, fasting blood sugar, SBP, smoking history and baPWV. In addition, after adjustment for age and sex, carotid atherosclerosis was significantly associated with high baPWV, but not with obesity, dyslipidemia, IFG, smoking history, presence of CKD or high BP. Furthermore, baPWV is a more useful index for predicting IMT than high BP because the OR of a high baPWV was high compared with that of a high BP, and the area under the curve of baPWV had a high value compared with that of SBP.
The associations between IMT and risk factors for atherosclerosis, such as hypertension, metabolic syndrome and diabetes mellitus, have been reported previously. With regard to hypertension, it is clear that BP is an independent risk factor for carotid atherosclerosis.20,21
Matsui et al reported that the maximum home SBP was significantly associated with left ventricular mass index and IMT, and assessment of the maximum home SBP may increase the predictive value of hypertensive target organ damage in the heart and arteries.22
It has been reported that the metabolic syndrome is associated with progression of early carotid atherosclerosis in the general population23
and with subclinical atherosclerosis.24
However, the association between IMT and the HbA1c value or the severity of diabetes mellitus is controversial. Although Selvin et al showed a significant association between HbA1c and IMT in 2,060 diabetic patients,25
Temelkova-Kurktschiev et al reported no significant correlation between HbA1c and IMT after adjustment for sex and age in newly detected type 2 diabetic subjects.26
In the present study, carotid atherosclerosis was significantly associated with high baPWV and high BP, but not with obesity, dyslipidemia or IFG, and high baPWV strongly related with carotid atherosclerosis in comparison with high BP. In addition, baPWV is a simple and noninvasive examination that could be useful to detect early atherosclerosis in the clinical setting and in general populations.
Although carotid-femoral PWV (cfPWV) is widely considered to be the most established index of arterial stiffness, the baPWV is a simple, noninvasive, and automatic method that can evaluate arterial stiffness, and closely correlates with aortic PWV.8,9
cfPWV showed a positive association with IMT in elderly patients, with a correlation coefficient of 0.322.27
In our study, baPWV had a significant association with carotid IMT, with a similar correlation coefficient (r=0.353). Therefore, it is suggested that baPWV, like cfPWV, is a useful index of early-stage atherosclerosis.
We reported that baPWV was more dependent on BP compared with CAVI.28
However, in the present study, we adjusted the BP, including SBP and DBP, and revealed that baPWV was a predictor of carotid atherosclerosis, which was independent of BP. These results suggested high baPWV as an independent predictor of carotid atherosclerosis.
IMT is considered to be a parameter of structural change in atherosclerosis whereas baPWV can be evaluated as an arterial functional distensibility. There are several studies that report the mechanism of how PWV affects atherosclerosis. Dao et al reported that increased arterial stiffness leads to increased SBP and decreased DBP,29
and promotes vascular remodeling. Furthermore, increased luminal pressure stimulates excessive collagen production, and these molecular changes lead to a doubling or tripling of the IMT.30
On the other hand, we demonstrated that baPWV correlated with IMT independent of classical risk factors such as high BP. There may be a new mechanism for baPWV accelerating worsening of the IMT.
In a meta-analysis, it was found that an increase in baPWV of 1 m/s corresponds to increases of 12% in total cardiovascular events, 13% in cardiovascular deaths, and 6% in all-cause deaths.31
Several studies have reported the cutoff value of baPWV for cardiovascular disease. In patients with acute coronary syndrome, the cutoff value for predicting a post-hospitalization cardiovascular event was 1,700 cm/s, and that for predicting a major cardiovascular event was 1,800 cm/s.32
In hypertensive patients, a value of 1,750 cm/s is an appropriate cutoff value for predicting the onset of stroke, cardiovascular disease, stroke and cardiovascular disease, and total death.33
Elevated baPWV is a risk factor for re-admission or cardiac death of heart failure patients and the cutoff value is 1,750 cm/s.34
In addition, Lee et al demonstrated that baPWV was useful for estimating the risk of cardiovascular events in patients with suspected or known coronary artery disease, and the cutoff value was 1,790 cm/s.35
On the other hand, the present study demonstrated that the cutoff value of baPWV to predict carotid atherosclerosis in a general male population was 1,626 cm/s. In addition, when the cutoff value of baPWV was >1,600 cm/s, the sensitivity and specificity were 0.65 and 0.68, respectively. These results are similar to those with a baPWV=1,626 cm/s. Therefore, we propose that baPWV >1,600 cm/s is the screening value for early atherosclerosis in the general population. If baPWV is >1,600 cm/s in the general male population, we recommend further examinations including carotid ultrasonography.
Study Limitations
First, it was a cross-sectional study. Therefore, a prospective longitudinal study is needed to confirm the relation between baPWV and IMT in the general population. Second, baPWV cannot be measured accurately in patients with aortic valve stenosis, peripheral arterial disease, or atrial fibrillation. Therefore, subjects with peripheral artery disease or atrial fibrillation were excluded. Third, we did not have detailed data on alcohol intake and medication because detailed declaration was lacking in the questionnaire used in this study.
Conclusions
For the first time, a high baPWV value has been revealed as a stronger predictor of early carotid atherosclerosis than high BP, dyslipidemia, or IFG in a Japanese general male population.
Disclosures
The authors have no conflicts of interest to declare.
References
- 1.
Nambi V, Chambless L, Folsom AR, He M, Hu Y, Mosley T, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: The ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol 2010; 55: 1600–1607.
- 2.
Nichols WW, Pepine CJ, O’Rourke MF. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke. N Engl J Med 1999; 340: 1762–1763.
- 3.
Ikeda N, Kogame N, Iijima R, Nakamura M, Sugi K. Impact of carotid artery ultrasound and ankle-brachial index on prediction of severity of SYNTAX score. Circ J 2013; 77: 712–716.
- 4.
Cheng KS, Mikhailidis DP, Hamilton G, Seifalian AM. A review of the carotid and femoral intima-media thickness as an indicator of the presence of peripheral vascular disease and cardiovascular risk factors. Cardiovasc Res 2002; 54: 528–538.
- 5.
Kawada H, Sumimoto T, Okayama H, Hiwada K. Structure and function of the left ventricle and carotid artery in hemodialysis patients. Hypertens Res 2001; 24: 221–227.
- 6.
Rahn KH, Barenbrock M, Hausberg M, Kosch M, Suwelack B, Witta J. Vessel wall alterations in patients with renal failure. Hypertens Res 2000; 23: 3–6.
- 7.
Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001; 37: 1236–1241.
- 8.
Yamashina A, Tomiyama H, Takeda K, Tsuda H, Arai T, Hirose K, et al. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens Res 2002; 25: 359–364.
- 9.
Kubo T, Miyata M, Minagoe S, Setoyama S, Maruyama I, Tei C. A simple oscillometric technique for determining new indices of arterial distensibility. Hypertens Res 2002; 25: 351–358.
- 10.
Kusunose K, Sato M, Yamada H, Saijo Y, Bando M, Hirata Y, et al. Prognostic implications of non-invasive vascular function tests in high-risk atherosclerosis patients. Circ J 2016; 80: 1034–1040.
- 11.
Sheng CS, Li Y, Li LH, Huang QF, Zeng WF, Kang YY, et al. Brachial-ankle pulse wave velocity as a predictor of mortality in elderly Chinese. Hypertension 2014; 64: 1124–1130.
- 12.
Kim J, Song TJ, Song D, Lee KJ, Kim EH, Lee HS, et al. Brachial-ankle pulse wave velocity is a strong predictor for mortality in patients with acute stroke. Hypertension 2014; 64: 240–246.
- 13.
Nagai K, Shibata S, Akishita M, Sudoh N, Obara T, Toba K, et al. Efficacy of combined use of three non-invasive atherosclerosis tests to predict vascular events in the elderly: Carotid intima-media thickness, flow-mediated dilation of brachial artery and pulse wave velocity. Atherosclerosis 2013; 231: 365–370.
- 14.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004; 363: 157–163.
- 15.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486–2497.
- 16.
Teramoto T, Sasaki J, Ishibashi S, Birou S, Daida H, Dohi S, et al. Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan: 2012 version. J Atheroscler Thromb 2013; 20: 517–523.
- 17.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 2009; 53: 982–992.
- 18.
Collins AJ, Roberts TL, St Peter WL, Chen SC, Ebben J, Constantini E. United States Renal Data System assessment of the impact of the National Kidney Foundation-Dialysis Outcomes Quality Initiative guidelines. Am J Kidney Dis 2002; 39: 784–795.
- 19.
Yamashina A, Tomiyama H, Arai T, Hirose K, Koji Y, Hirayama Y, et al. Brachial-ankle pulse wave velocity as a marker of atherosclerotic vascular damage and cardiovascular risk. Hypertens Res 2003; 26: 615–622.
- 20.
Shimabukuro M, Hasegawa Y, Higa M, Amano R, Yamada H, Mizushima S, et al. Subclinical carotid atherosclerosis burden in the Japanese: Comparison between Okinawa and Nagano residents. J Atheroscler Thromb 2015; 22: 854–868.
- 21.
Su TC, Chien KL, Jeng JS, Chen MF, Hsu HC, Torng PL, et al. Age- and gender-associated determinants of carotid intima-media thickness: A community-based study. J Atheroscler Thromb 2012; 19: 872–880.
- 22.
Matsui Y, Ishikawa J, Eguchi K, Shibasaki S, Shimada K, Kario K. Maximum value of home blood pressure: A novel indicator of target organ damage in hypertension. Hypertension 2011; 57: 1087–1093.
- 23.
Jung JM, Young Kwon D, Han C, Park MH. Metabolic syndrome and early carotid atherosclerosis in the elderly. J Atheroscler Thromb 2014; 21: 435–444.
- 24.
Park GM, An H, Lee SW, Cho YR, Gil EH, Her SH, et al. Impact of metabolic syndrome on subclinical atherosclerosis in asymptomatic individuals. Circ J 2015; 79: 1799–1806.
- 25.
Selvin E, Coresh J, Golden SH, Boland LL, Brancati FL, Steffes MW. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: The atherosclerosis risk in communities study. Diabetes Care 2005; 28: 1965–1973.
- 26.
Temelkova-Kurktschiev TS, Koehler C, Leonhardt W, Schaper F, Henkel E, Siegert G, et al. Increased intimal-medial thickness in newly detected type 2 diabetes: Risk factors. Diabetes Care 1999; 22: 333–338.
- 27.
Shen L, Wu W, You B, Gao H, Wang C, Liu Y. Relationship between pulse wave velocity and carotid atherosclerosis in geriatric people. Cerebrovasc Dis 2011; 32(Suppl 1): 16–20.
- 28.
Kubozono T, Miyata M, Ueyama K, Nagaki A, Otsuji Y, Kusano K, et al. Clinical significance and reproducibility of new arterial distensibility index. Circ J 2007; 71: 89–94.
- 29.
Dao HH, Essalihi R, Bouvet C, Moreau P. Evolution and modulation of age-related medial elastocalcinosis: Impact on large artery stiffness and isolated systolic hypertension. Cardiovasc Res 2005; 66: 307–317.
- 30.
Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol 2005; 25: 932–943.
- 31.
Vlachopoulos C, Aznaouridis K, Terentes-Printzios D, Ioakeimidis N, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: A systematic review and meta-analysis. Hypertension 2012; 60: 556–562.
- 32.
Tomiyama H, Koji Y, Yambe M, Shiina K, Motobe K, Yamada J, et al. Brachial-ankle pulse wave velocity is a simple and independent predictor of prognosis in patients with acute coronary syndrome. Circ J 2005; 69: 815–822.
- 33.
Kawai T, Ohishi M, Takeya Y, Onishi M, Ito N, Oguro R, et al. Carotid plaque score and intima media thickness as predictors of stroke and mortality in hypertensive patients. Hypertens Res 2013; 36: 902–909.
- 34.
Meguro T, Nagatomo Y, Nagae A, Seki C, Kondou N, Shibata M, et al. Elevated arterial stiffness evaluated by brachial-ankle pulse wave velocity is deleterious for the prognosis of patients with heart failure. Circ J 2009; 73: 673–680.
- 35.
Lee HS, Kim HL, Kim H, Hwang D, Choi HM, Oh SW, et al. Incremental prognostic value of brachial-ankle pulse wave velocity to single-photon emission computed tomography in patients with suspected coronary artery disease. J Atheroscler Thromb 2015; 22: 1040–1050.