Editorials
Assessment of Atherosclerosis ― Vascular Imaging Tests and Vascular Function Tests ―
2017 Volume 81 Issue 3 Pages 304-305


Details
2017 Volume 81 Issue 3 Pages 304-305
It is well known that atherosclerotic lesions that cause primary cardiovascular disease comprise 2 aspects: plaque and vascular dysfunction. Therefore, it is clinically important to accurately assess atherosclerosis. Because of the recent development of devices for the diagnosis of plaque (e.g., coronary angiography, intravascular ultrasound, optical coherence tomography and coronary computerized tomography), plaque per se can be accurately assessed (Figure 1). The vascular function tests include tests for endothelial function (e.g., endothelium-dependent vasodilation induced by intra-arterial infusion of a vasoactive agent using coronary angiography, Doppler flow guide wire, and mercury-filled Silastic strain-gauge plethysmography, flow-mediated vasodilation, reactive hyperemia-peripheral arterial tonometry and enclosed-zone flow-mediated vasodilation), vascular response to nitroglycerine as an index of vascular smooth muscle function, pulse wave velocity (PWV), cardio-ankle vascular index, ankle-brachial pressure index, central blood pressure, augmentation index and stiffness ß (Figure 1).1–5 There are several guidelines for management of vascular function tests6,7 and although they are widely used, these tests unfortunately lack fixed opinions concerning standard measurement methods, interpretation of results, clinical significance and clinical applications. To reach consensus on a common biomarker for the management of cardiovascular diseases using vascular function tests, it is necessary to know the degree of vascular dysfunction, predict cardiovascular events, assess the effects of interventions on events, and certify the relationship between improvements in vascular function tests and therapeutic efficacy and prevention of cardiovascular events. In addition, application of vascular function tests in the clinical setting requires non-invasive and safe measurement methods, low cost for measurement of vascular function, high levels of accuracy and reproducibility, and standardization of measurement methods.
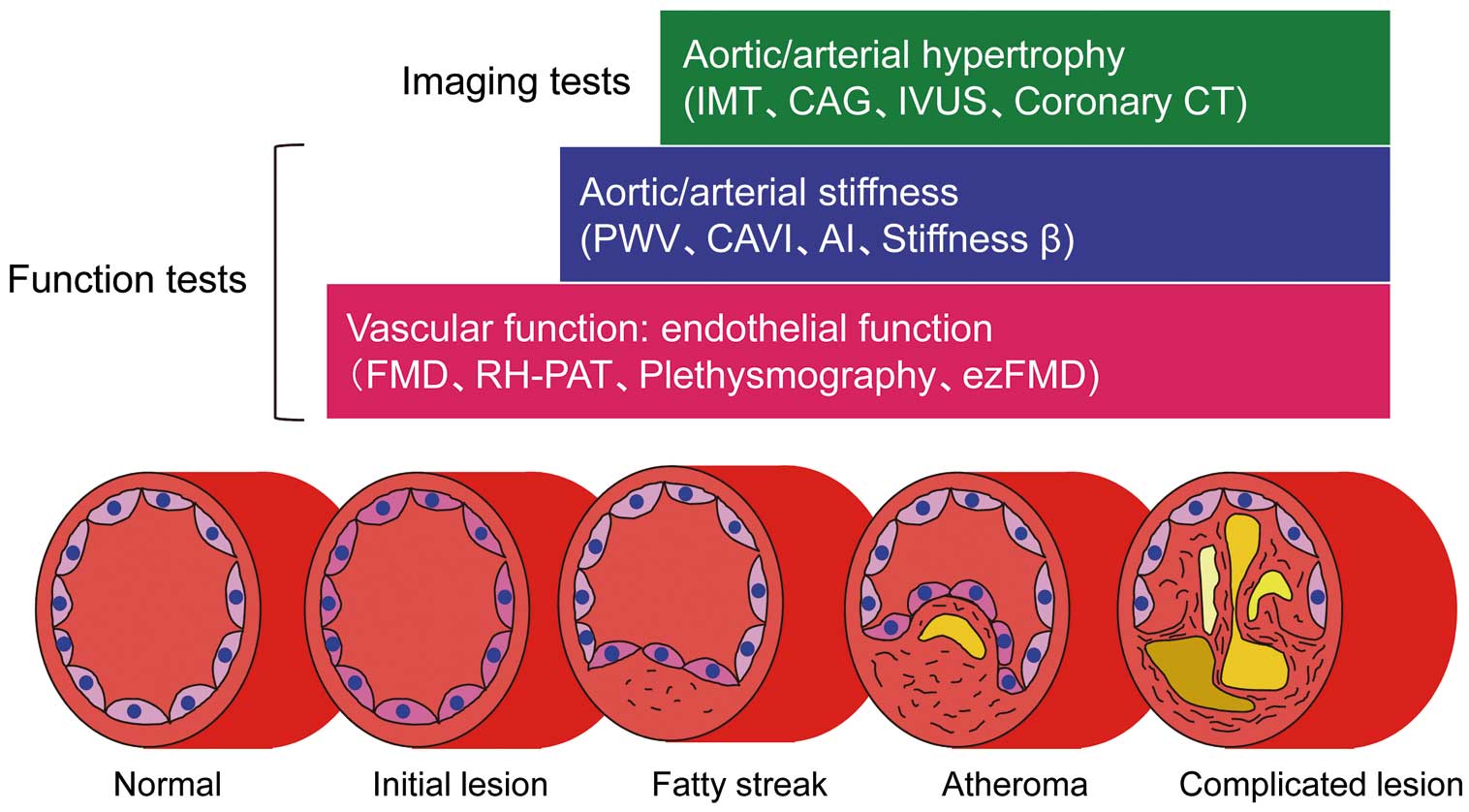
Assessment of vascular function and vascular structure: vascular function tests and vascular imaging tests (modified with permission from Higashi Y, et al1). AI, augmentation index; CAG, coronary angiography; CAVI, cardio-ankle vascular index; CT, computed tomography; ezFMD, enclosed-zone flow-mediated vasodilation; IMT, intima-media thickness; IVUS, intravascular ultrasound; PWV, pulse wave velocity; RH-PAT, reactive hyperemia-peripheral arterial tonometry.
Article p 310
Both the measurement of PWV, one of the vascular function tests, and measurement of the intima-media thickness (IMT), one of the vascular imaging tests, are established methods and have been shown to be predictors of cardiovascular events.8–11 Carotid IMT has been used as a surrogate marker of hard endpoints such as myocardial infarction, stroke and cardiac death in large clinical trials.9–11 Several lines of evidence have shown a significant positive correlation between PWV and IMT in patients with atherosclerosis.12,13 These findings suggest that IMT increases in relation to increases in PWV, that PWV increases in relation to increases in IMT or that both IMT and PWV simultaneously increase. However, it remains unclear whether the relationship between increases in PWV and in IMT in patients with atherosclerosis is a cause or a consequence. When anatomically considering the process of development of atherosclerosis, it is thought that arterial stiffness precedes arterial or aortic hypertrophy. If this is in fact true, an increase in PWV would precede an increase in IMT. Is this concept really correct?
In this issue of the Journal, Kubozono et al14 show that high brachial-ankle PWV was a stronger predictor of early carotid atherosclerosis assessed by measurement of carotid IMT than were traditional cardiovascular risk factors in a Japanese general male population. Their results indicated that vascular dysfunction leads to vascular hypertrophy from a methodological aspect as well as anatomical aspect, resulting in cardiovascular complications. An increase in PWV should overlap an increase in IMT in the process of atherosclerosis (Figure 1). It is also well known that PWV is underestimated in the presence of stenosis of an artery and/or aorta, suggesting that measurement of PWV may enable detection of an early stage of atherosclerosis but not advanced atherosclerosis. As the next step for evaluation of the relationship between measurements of PWV and IMT, we should more accurately determine whether any level of PWV reflects any stage of atherosclerosis with the absence of stenosis of an artery and/or aorta.
Vascular function tests have a relatively short history, and there is not sufficient evidence from clinical perspectives. It is expected that vascular function tests will become popular and will be appropriately used in the clinical setting. Further studies are needed to confirm the relationships among vascular function, arterial/aortic stiffness and arterial/aortic hypertrophy in the early to advanced stages of atherosclerosis in a large clinical trial. Which measurement parameters in vascular imaging tests and vascular function tests are sensitive and useful as biomarkers for degree of atherosclerosis, target for treatment of atherosclerosis and predictor of cardiovascular events? Which combination of measurement parameters is most useful? In any case, assessment of atherosclerosis should be made from every possible angle. In the future, atherosclerosis will be assessed by a combination of vascular imaging tests, vascular function tests, chemical biomarkers and genetic tests (Figure 2).2,4

Assessment of atherosclerosis performed in an integrated way (modified with permission from Soga J, et al2 and Higashi Y4). ABI, ankle-brachial pressure index; FMD, flow-mediated vasodilation; LDPI, laser Doppler perfusion imaging; TBI, toe brachial pressure index. Other abbreviations as in Figure 1.