Editorials
Rigid Left Ventricle With Attenuated Torsion as the Integrally Deteriorated Form of Dilated Cardiomyopathy
2017 Volume 81 Issue 4 Pages 440-441


Details
2017 Volume 81 Issue 4 Pages 440-441
Analyses of left ventricular (LV) mechanics based on myocardial deformation have provided various insights, even in clinical studies. In particular, speckle-tracking echocardiography (STE) has contributed, with the star parameter “strain”. The number of studies retrieved from the PubMed database using the key word ‘myocardial strain’ has tripled in the past decade, reaching 592 articles in 2016, although various limitations of strain have been pointed out.1 Of the strain components derived from STE, global longitudinal strain (GLS) has been the most reliable and useful parameter, supported by various evidence, and has been standardized by reducing intervendor differences and ambiguities in the strain algorithms.2 Beyond the LV ejection fraction (EF), LS provides additional information on the severity of cardiac function, clinical outcome of heart failure (HF) and valvular diseases. Accordingly, myocardial deformation is more closely related to intrinsic myocardial and chamber function than LVEF. However, the dissociation between LVEF and LS is particularly evident in patients with preserved LVEF. LV longitudinal deformation is a function of the subendomyocardium, and GLS is reduced even in asymptomatic normotensive diabetes patients.3 Thus, GLS undoubtedly has a role as an early marker of subclinical myocardial dysfunction in patients with preserved LVEF. As well, the significance of GLS has been reported even in patients with advanced HF requiring transplantation.4 However, the mechanical disturbances in advanced HF are more complex. In dilated cardiomyopathy (DCM), myocardial fibrosis is present not only in the subendomyocardium but also in the LV mid-wall, which is associated with poor prognosis in DCM.5,6 The mid-wall fibrosis observed in DCM is associated with other LV mechanics, which are reduced circumferential strain and LV torsion of a LV twisting parameter.7 The underlying mechanism may be attributed to the fact that mid-wall fibrosis preferentially affects the mid-wall circumferential fiber function. The terminology of LV twisting mechanism may need to be explained, as it will not be familiar to general cardiologists. First, rotation is the angular displacement of the LV in each short-axis slice (Figure 1). Second, LV twist is the systolic peak of the instantaneous difference between the basal and apical levels. Finally, LV torsion is the twist per level distance (degree/cm), which is obtained by dividing twist by the distance between the base and apex.
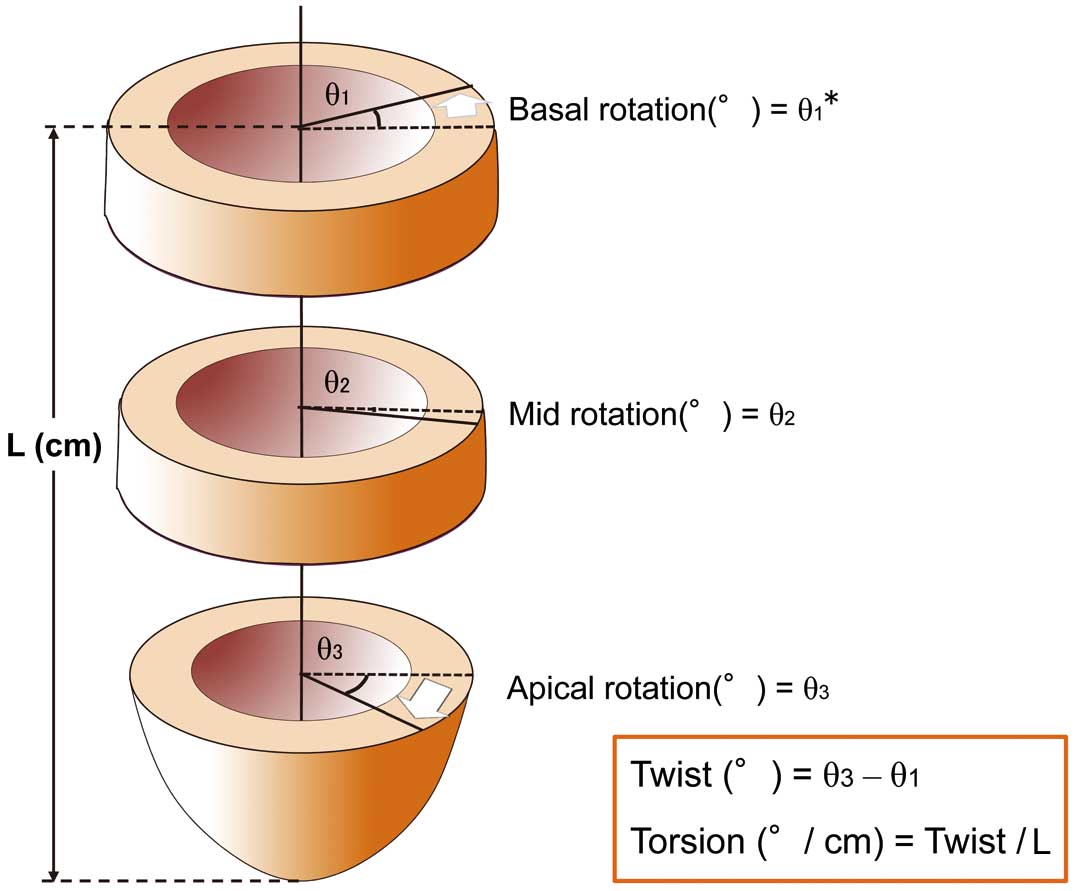
Parameters of left ventricular twisting mechanism. *Basal rotation has a negative value because the basal segments rotate in the counter direction to the apex in a normal heart. L, distance between base and apex.
Article p 529
LV torsion is produced by shortening of obliquely oriented myocardial fibers. However, mid-wall circumferential fiber dysfunction inhibits LV rotation, because the mid-wall fibers create horizontal counterforces. In addition, LV torsion is affected by LV remodeling and disturbance of the LV conduction system. In particular, LV dyssynchrony attenuates LV torsion, which cannot be improved even after cardiac resynchronization therapy.8,9 Therefore, the LV twisting mechanism has been featured in the assessment of myocardial and chamber dysfunction in patients with DCM. Notomi et al elegantly demonstrated the significant relationship of LV torsion with LV reverse remodeling and clinical outcomes after mitral valve surgery in severely symptomatic DCM patients with severe secondary mitral regurgitation.8 These reports on DCM or nonischemic cardiomyopathy show that a reduced twisting mechanism relates to the more advanced features of HF, including significant LV remodeling, presence of LV dyssynchrony, and severe LV diastolic dysfunction. Therefore, the LV twisting mechanism may be an integrated surrogate marker of disease severity in DCM (Figure 2).
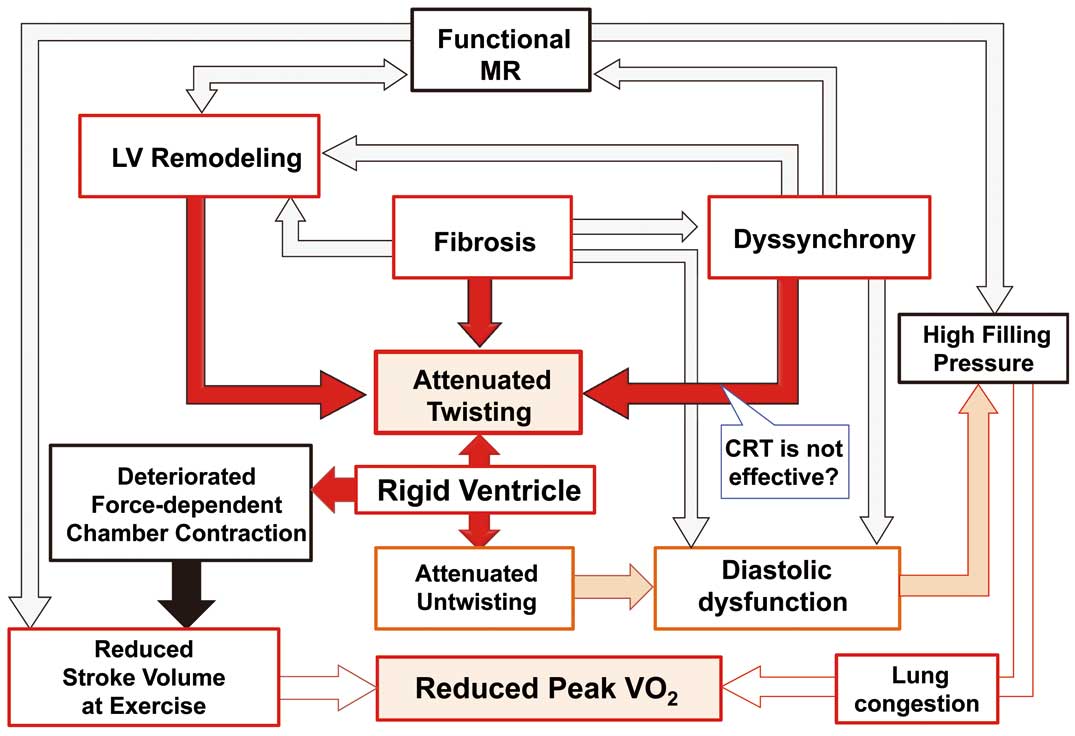
Pathophysiological relation of rigid ventricle with associated factors. The black arrow means a suggestive pathophysiology. CRT, cardiac resynchronization therapy; LV, left ventricle; MR, mitral regurgitation.
In this issue of the Journal, Sveric et al10 show the relationship of LV torsion with functional capacity using cardiopulmonary exercise testing of patients with DCM. This prospective study was well designed, and consisted of subjects with relatively uniform characteristics (short history after HF onset, sinus rhythm, no left bundle branch block and significant mitral regurgitation) but a wide range of peak oxygen uptake (peak V̇O2: 11.9–33.4 mL/kg/min). The advantage of this study was that LV torsion was analyzed by 3D echocardiography. As compared with 2D echocardiography, 3D echocardiography can provide more accurate LV twist and the distance between base and apex because full LV segmental data are obtained in the same cardiac cycles, and is unaffected by the whole heart moving through the 2D plane of interest, which is well known as the “through-plane” or “out-of-plane” phenomenon.11
Why Does the Twisting Mechanism Obtained at Rest Determine the Exercise Tolerance?The point of this study is that the peak V̇O2 in patients with DCM depended on the magnitude of LV torsion at rest.10 In the reduced peak V̇O2 group, baseline characteristics, including age, sex, vital signs, NYHA class and NT-pro BNP level, did not differ from those in the preserved peak V̇O2 groups. As the authors discuss, peak V̇O2 represents an adaptive LV stroke volume at peak exercise. A previous study suggested LV torsion is a force-dependent parameter rather than volume dependent.12 Therefore, torsion might be augmented during exercise, and associated with the exercise capacity parameter at peak exercise. In addition, LV torsion correlated with LV diastolic dysfunction as the key parameter of exercise capacity in HF patients. Untwisting coupled with twisting might be helpful to preserve LV diastolic function, even in patients with reduced EF. Conversely, in the rigid LV with attenuated LV torsion, higher filling pressure will be needed.
Recent studies has reported that decreased ventilatory efficiency (elevated V̇E /V̇CO2 ratio or steeper V̇E/V̇CO2 slope) and an oscillatory breathing pattern are more significant prognostic markers than peak V̇O2;13,14 however, Sveric et al did not assess the parameters or oscillatory breathing.10 In addition, they could not provide information about the clinical outcomes of the patients with DCM.
Nevertheless, we look forward to LV torsion on 3D echocardiography becoming a reliable marker of clinical outcome in HF patients, and hope that multicenter prospective studies will be performed to validate its significance in the near future.
None.