Images in Cardiovascular Medicine
Ventricular Fibrillation Triggered by Earthquake During the Accumoli-Amatrice Disaster in Italy
2017 Volume 81 Issue 5 Pages 759-760

Details
2017 Volume 81 Issue 5 Pages 759-760
A51-year-old woman, treated in 2006 with mastectomy for breast cancer and subsequently with chemotherapy in 2013 for bone and lung metastases, was rescued from ventricular fibrillation (VF) in July 2015. Cardiovascular evaluation showed a mildly dilated left ventricle (LV) with an ejection fraction (EF) of 46%, consistent with moderate cardiac toxicity of the chemotherapy, known since 2013, and normal coronary arteries. No ion channel disease was detectable. A subcutaneous implantable cardioverter defibrillator (S-ICD) was implanted, and the patient received education to cope with arrhythmia-related symptoms and with shock delivery, as per the center’s protocol. The patient was discharged on bisoprolol, and follow-up was uneventful for 12 months.
On 24 August 2016, while on holiday in her native area in the Marche region in Italy, she was abruptly awakened at 03:34 hours by the earthquake occurring in the Accumoli-Amatrice area. While realizing that an earthquake with long-lasting shaking waves was ongoing, she began to feel pounding in her chest, then in a short time dizziness ensued, and she dropped to the floor, as she had been taught to do in that specific circumstance. Then she felt faint, and full consciousness was suddenly resumed. On telephone contact at mid-morning, we advised the patient to leave the area as soon as feasible; on ambulatory follow-up at hospital on 5 September, a VF episode was noted to have occurred at 03:35 hours on 24 August (Figure), within the very first 2 min of the Accumoli-Amatrice earthquake.
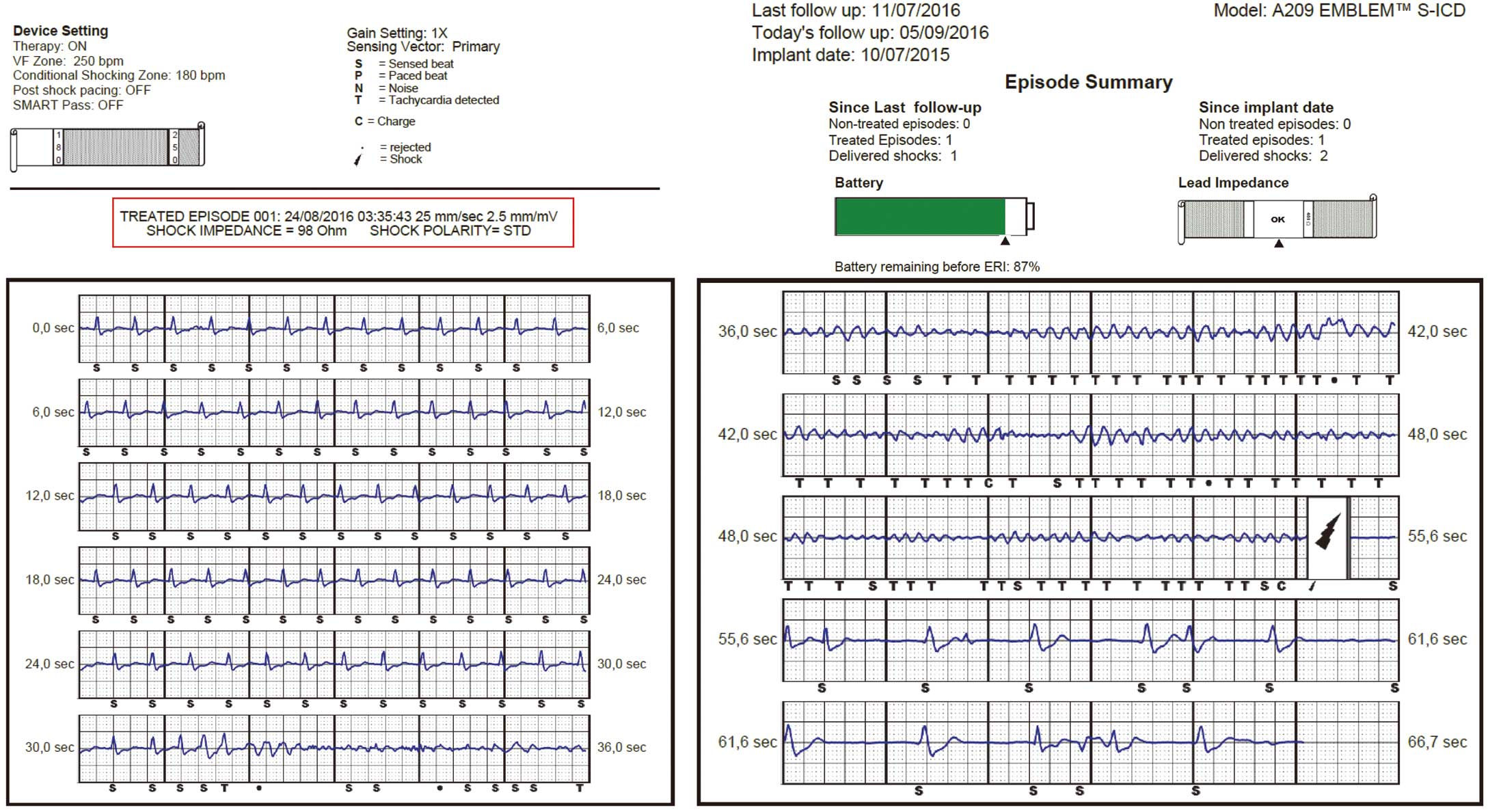
Sinus Tachycardia in the range 110–130 beats/min, giving abruptly rise to VF. Detection and VF termination with a single shock occur 21s after arrrhythmia onset. ·, rejected;  , shock; C, charge; N, noise; P, paced beat; S, sensed beat; T, tachycardia detected.
, shock; C, charge; N, noise; P, paced beat; S, sensed beat; T, tachycardia detected.
No change in disease status or in LVEF was detected. The patient was psychologically confident in S-ICD functioning. On counselling, she did not return to the earthquake area, where huge shaking waves have been ongoing as of the end of October 2016. As at the time of writing, follow-up has confirmed the absence of arrhythmias and other cardiovascular events (CVE).
Abrupt stress, as in the acute and subacute phases of a great earthquake, has been reported to precipitate major CVE such as cardiopulmonary arrest (CPA), acute coronary syndrome (ACS), heart failure (HF), and stroke.1 The present patient had VF in the first to second minute after the first earthquake shake, possibly mediated by huge adrenergic arousal, as reflected by the rate increase up to 120–130 beats/min preceding VF onset (Figure), despite bisoprolol treatment. This has been observed during the Great East Japan Earthquake that hit the Miyagi prefecture in March 2011: the time course of CVE shows that CPA increased immediately compared with the period preceding the earthquake, then rapidly decreased in the following days, to recur only in the event of further earthquake shakes,1,2 either in the general population2 or in ICD recipients.3 In contrast, ACS, HF and stroke tended to increase in the 2 weeks following the earthquake, and gradually decreased during the following 6 weeks.1 CPA were more likely to occur in the elderly, in women, and in residents close to the earthquake epicenter owing to repeated shakes,2 hence we asked the patient not to return to her native area until earthquake termination. We believe that the East Japan Earthquake experience was helpful in counseling the patient, in order to prevent further arrhythmic events or a true electrical storm.