Abstract
Background:
Fabry disease is an X-linked lysosomal storage disorder and shows globotriosylceramide (Gb3) accumulation in multiple organs, resulting from a deficiency of α-galactosidase. In patients with Fabry disease, cardiovascular disease occurs at an early age. Previous studies have shown that serum levels of high-density lipoprotein-cholesterol (HDL-C) increase in this disease, yet its clinical significance for cardiovascular disease remains unclear.
Methods and Results:
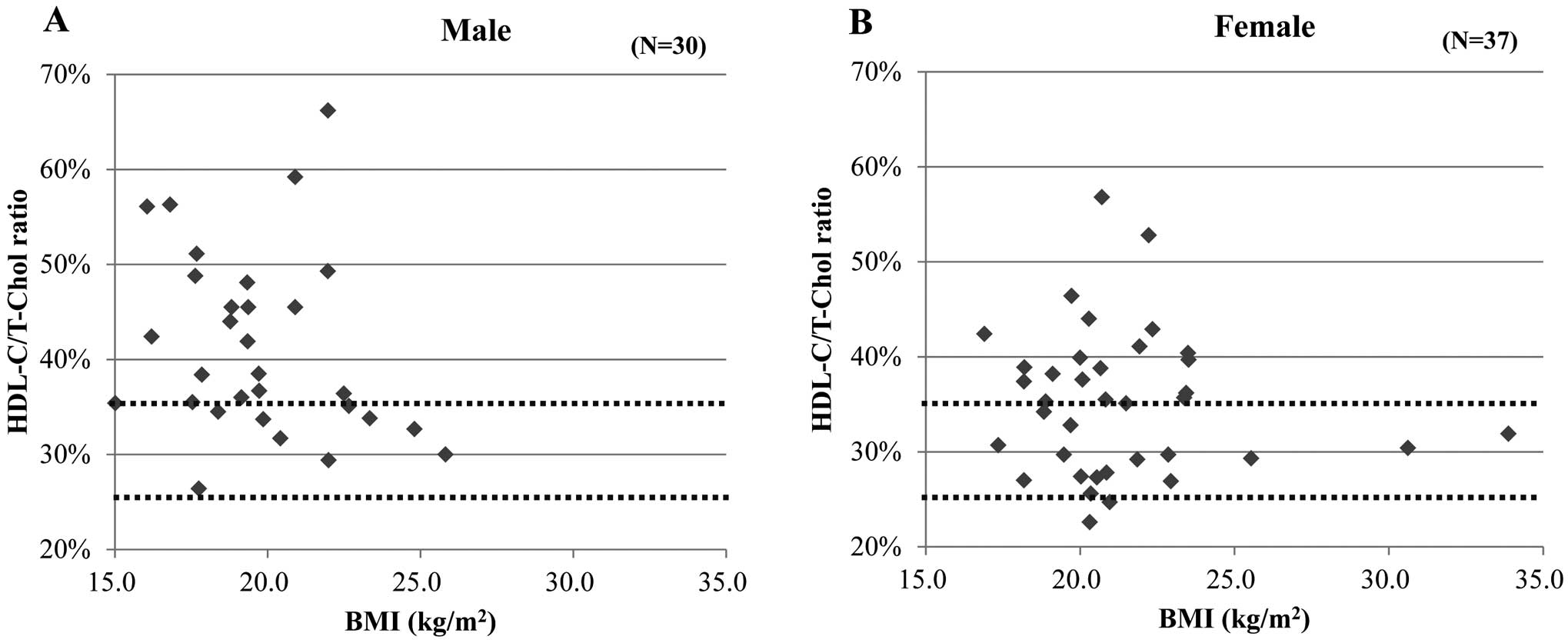
In order to determine why the serum HDL-cholesterol is high in various cardiovascular diseases of Fabry disease patients, we evaluated the serum lipid profiles, ocular vascular lesions, and levels of serum vascular endothelial growth factor (VEGF) and intercellular adhesion molecule-1 in 69 patients with Fabry disease diagnosed by genetic examination. The serum HDL-C/total cholesterol (T-Chol) ratio was significantly high, especially in male patients (41.5±1.7%) regardless of body mass index. Ocular vascular lesions were more likely to occur in female patients with a high HDL-C/T-Chol ratio compared with most male patients. Female patients with a high HDL-C/T-Chol ratio also presented a high serum VEGF level, suggesting that vascular endothelium dysfunction and arteriosclerotic changes progress more severely than in patients with a normal HDL-C/T-Chol ratio. In most patients, enzyme replacement therapy improved serum Gb3 and lyso-Gb3 levels, but these Gb3 and lyso-Gb3 still remained higher than in healthy controls, which appears to result in continuous vascular arteriosclerotic changes.
Conclusions:
We concluded that increased low-density lipoprotein-cholesterol uptake to the vascular wall caused by endothelial dysfunction is likely to contribute to the high HDL-C/T-Chol ratio observed in Fabry disease patients.
Fabry disease (OMIM no. #301500) is an X-linked lysosomal storage disease caused by loss-of-function mutations of α-galactosidase (GLA).1
In patients with Fabry disease, globotriosylceramide (Gb3) and other glycosphingolipids progressively accumulate in different tissues.1
The specific symptoms of this disease are angiokeratoma, acroparesthesia and hypohydrosis, but other organs, such as the heart, kidneys and blood vessels are also affected, resulting in multiorgan failure and premature death.2,3
For example, in cardiac systems, Gb3 accumulates in heart muscle cells and vascular endothelial and smooth muscle cells, which causes chronic heart failure, left ventricular hypertrophy and arrhythmia.4,5
In vascular, endothelial and smooth muscle cells are affected by Gb3, resulting in vascular endothelial dysfunction and wall thickening.6,7
Previous studies have shown increased carotid intima-media thickness (IMT) and decreased brachial flow-mediated dilation (FMD).8
Although the GLA gene is on the X chromosome, female carriers can be also affected because of lyonization, which results in as many kinds of symptoms as in male patients. The only treatment at present for Fabry disease is enzyme replacement therapy (ERT).9
ERT is effective for acroparesthesia, left ventricular hypertrophy (most common heart lesion in Fabry disease) and renal dysfunction.9–12
However other studies suggest progression of vascular lesions, and autopsies of Fabry disease patients have shown Gb3 accumulation in vascular walls even after ERT.13,14
Previous studies have shown that serum high-density lipoprotein-cholesterol (HDL-C) levels are higher in Fabry disease patients than in healthy controls.15,16
The HDL-C levels remained high even after ERT in those studies. On the other hand, high HDL-C level is related to elimination of the risk of cardiovascular disease.17
It remains unclear why serum HDL-C levels are high in Fabry disease patients and why cardiovascular diseases occur earlier than in other people despite high HDL-C levels. In order to figure out the clinical meaning of serum cholesterol levels in Fabry disease, we analyzed the relationship between serum cholesterol level and vascular lesions. We evaluated vascular lesions by ocular vascular features, and levels of serum vascular endothelial growth factor (VEGF) and intercellular adhesion molecule-1 (ICAM-1), because serum VEGF and ICAM-1 are useful for detecting the early stages of atherosclerotic lesions18–20
and are thought to be related to diabetic microangiopathy.21
In previous studies, these cytokines were higher in this disease than in healthy controls.7,22
We also measured serum Gb3 and lyso-Gb3 levels before and after ERT based on our hypothesis that the cholesterol profile is affected by these factors.
Methods
We carried out an observational study of Fabry disease patients at Nagoya Central Hospital who were confirmed by clinical manifestation and genetic testing. The mutation of E66Q is now thought to be a genetic polymorphism,23,24
so this mutation was excluded. Patients with no test results for HDL-C and low-density lipoprotein-cholesterol (LDL-C) were also excluded. The sex proportions in this study were 30 males and 37 females. The study was conducted in accordance with the Declaration of Helsinki and applicable local laws and regulations. Patients provided written informed consent before inclusion in the study.
In previous studies, serum cholesterol levels have shown no obvious changes before and after ERT, so we used the blood test results from the first visit to hospital regardless of ERT. The serum lipid profile was determined by enzymatic method. The reference ranges were: 120–219 mg/dL for total cholesterol (T-Chol); 40–85 mg/dL in men and 40–95 mg/dL in women for HDL-C; 65–139 mg/dL for LDL-C; 30–149 mg/dL for triglycerides (TG); and 25–35% for the T-Chol/HDL-Chol (T-Chol/LDL) ratio. Serum VEGF and ICAM-1 levels were measured by enzyme immunoassay (EIA). The normal range of serum VEGF is <38.3 pg/mL, and for serum ICAM-1 is 82.5–276 ng/mL. Gb3 and lyso-Gb3 levels were measured by liquid chromatography–tandem mass spectrometry (LC-MS/MS). Ocular vascular lesions were evaluated by ophthalmologists. The Scheie classification was used for hypertensive and arteriosclerotic lesion assessments.25
All data are described as mean±SD or median (95% CI). Fisher’s exact test, paired t-test and Mann-Whitney U-test were us in the statistical analysis. We defined P<0.05 as statistically significant.
Results
Patients’ Characteristics
The age of patients included in this study ranged from 6 to 55 years (median 33) in the males and from 14 to 64 years (median 43) in the females. None of the male patients had dyslipidemia, but 2 female patients did and were treated with statins. Average body mass index (BMI) was 20.1±0.6 kg/m2
in the males and 21.5±0.5 kg/m2
in the females.
Serum Lipid Profiles (Table 1)
In male and female patients, respectively, the serum lipid profiles were as follows: T-Chol, 166.8±5.2 mg/dL (4.32±0.13 mmol/L) and 203.8±5.4 mg/dL (5.28±0.14 mmol/L), which was almost the same as in previous studies of Fabry disease patients;15,16
TG, 77.1±6.4 mg/dL (0.87±0.07 mmol/L) and 105.4±10.4 mg/dL (1.19±0.12 mmol/L); LDL-C, 87.5±4.8 mg/dL (2.27±0.12 mmol/L) and 119.0±4.4 mg/dL (3.08±0.11 mmol/L); HDL-C, 67.2±4.7 mg/dL (1.74±0.12 mmol/L) and 68.7±4.5 mg/dL (1.78±0.11 mmol/L). A total of10 female patients had dyslipidemia; all showed only high LDL-C.
Table 1.
Serum Lipid Profiles of Fabry Disease Patients
| |
Laboratory
reference range |
Male
(n=30) |
Female
(n=37) |
| Age (years) |
|
31.4±4.1 (6–55) |
45.67±4.8 (14–64) |
| BMI (kg/m2) |
|
20.1±1.2 |
21.5±1.0 |
| T-Chol (mg/dL) |
130–220 |
166.8±5.2 |
203.8±5.4 |
| LDL-C (mg/dL) |
65–139 |
87.5±4.8 |
119.0±4.4 |
| Triglycerides (mg/dL) |
40–150 |
77.1±6.4 |
105.4±10.4 |
| HDL-C (mg/dL) |
40–85 (M)/40–95 (F) |
67.8±2.3 |
70.2±2.0 |
| HDL/Total (%) |
25–35 |
41.5±1.7* |
35.2±1.2 |
*P<0.05. BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; T-Chol, total cholesterol.
The HDL-C/T-Chol ratio was higher than the reference range in 22 of the 30 male patients and in 20 of the 37 female patients. The HDL-C/T-Chol ratio was 41.5±1.7% in males and 35.2±1.2% in females. We also analyzed whether this cholesterol profile correlated with age (Figure S1), but did not find a clear correlation in either sex. Male patients aged >50 years were also included in the high HDL-C/T-Chol ratio group, but they had significant heart atrophy and renal dysfunction, which suggested that a high HDL-C/T-Chol ratio does not contribute to cardiovascular protection.
We also analyzed the relationship between BMI and the HDL-C/T-Chol ratio. As shown in
Figure 1
the correlation coefficient was −0.097 in males and −0.231 in females, which is not a clear correlation.
Ocular Vascular Lesions and Relationship to Serum Cholesterol
Abnormal findings in the ocular vessels were identified in 23 of the 27 male patients and in 17 of 34 female patients. Common vascular lesions were arteriolar tortuosity, arteriolar narrowing, broadening of the light reflex with minimal arteriolovenous compression in fundic vessels. Conjunctival microaneurysms, vessel overswelling or irregularities of the vessel’s caliber were found in 4 patients. The ocular vascular lesions of the patients in this study are shown in
Table 2. A previous study reported tortuosity of retinal vessels, venous vascular aneurysmal dilatation and caliber irregularities.26
However, aneurysms of the conjunctival vessels were much fewer (4 of 61 patients) compared with previous studies reporting that aneurysms were observed in 68–97% patients.26–28
Table 2.
Ocular Vascular Lesions in Fabry Disease Patients
| Vascular lesion |
Male (%) |
Female (%) |
| Fundic vascular tortuosity |
20 (74) |
8 (24) |
| Scheie classification |
| H0 |
11 (41) |
21 (62) |
| H1 |
13 (48) |
11 (32) |
| H2 |
3 (11) |
2 (6) |
| H3 |
0 (0) |
0 (0) |
| S0 |
10 (37) |
21 (62) |
| S1 |
15 (56) |
12 (35) |
| S2 |
1 (4) |
1 (3) |
| S3 |
1 (4) |
0 (0) |
In addition to these vascular lesions, conjunctiva microaneurysms (1 patient), vessel overswelling (1 patient) and irregularities of the vessel caliber (2 patients) were observed.
In this study, only 3 male and 4 female patients showed hypertension and only 10 female patients showed dyslipidemia; hypertensive and arteriosclerotic changes occurred in most of the male patients and half of the female patients, suggesting that Fabry disease, but not the more common diseases such as hypertension and dyslipidemia, causes arteriolar lesions.
We also analyzed the correlation between the HDL-C/T-Chol ratio and ocular vascular lesions (Table 3). We divided our patients into 2 groups according to the HDL-C/T-Chol ratio (≤35% vs. >35%). In male patients, ocular vascular lesions were found at almost the same rate in both groups. However, female patients with a high HDL-C/T-Chol ratio (>35%) were more likely to have ocular vascular lesions, although not statistically significant in Fisher’s exact test. Our results suggested that a high HDL-C level does not play a vascular protective role in Fabry disease patients.
Table 3.
Relationship Between Ocular Vascular Lesions and HDL-C/T-Chol Level
| |
HDL-C/T-Chol
>35% (%) |
HDL-C/T-Chol
≤35% (%) |
| Male |
| Ocular vascular lesions (+) |
17 (85) |
7 (100) |
| Ocular vascular lesions (−) |
3 (15) |
0 (0) |
| Total |
20 |
7 |
| Female |
| Ocular vascular lesions (+) |
12 (71) |
7 (41) |
| Ocular vascular lesions (−) |
5 (29) |
10 (59) |
| Total |
17 |
17 |
The results of Fisher’s exact test were P=0.55 in males and P=0.17 in females. HDL-C, high-density lipoprotein-cholesterol; T-Chol, total cholesterol.
In order to determine whether serum VEGF and ICAM-1 levels change after ERT, we compared 14 patients with serum VEGF and ICAM-1 data before and after ERT using the Wilcoxon rank sum test. Neither VEGF nor ICAM-showed a decrease after ERT, so we used the serum VEGF and ICAM-1 data from the first hospital visit regardless of administration of ERT. The serum VEGF level was >38.3 pg/mL in 12 of 18 male patients and in 12 of 22 female patients. ICAM-1 was higher than the reference range in 16 of 18 male patients and in 13 of 22 female patients. We analyzed the correlation between these cytokines and the HDL-C/T-Chol ratio. Serum VEGF was significantly higher in patients with a high HDL-C/T-Chol ratio, especially in female patients (P=0.138 in males; P=0.047 in females) (Figure 2). Serum ICAM-1 did not show a clear correlation with the HDL-C/T-Chol ratio. Previous studies have shown that serum VEGF and ICAM-1 levels increase from an early stage of atherosclerosis. So it is likely that a high HDL-C/T-Chol ratio reflects some vascular lesions in Fabry disease. In addition, patients with ocular vascular lesions had more tendency towards a high serum VEGF level. Our results suggested that a high HDL-C/T-Chol ratio and high serum VEGF indicate vascular damage in Fabry disease patients.

In order to determine why the HDL-C/T-Chol ratio and VEGF levels remain high, we analyzed the serum Gb3 and lyso-Gb3 levels before and after ERT (Table 4). For the data from “after ERT”, we used the latest blood test results from all patients who underwent this treatment for at least 3 months. In male patients, Gb3 decreased from 15.7 ng/mL to 6.49 ng/mL and lyso-Gb3 decreased from 83.4 pg/mL to 32.3 pg/mL on average. In female patients, Gb3 decreased from 9.00 ng/mL to 5.61 ng/mL and lyso-Gb3 decreased from 10.5 pg/mL to 6.84 pg/mL on average. These results suggested that ERT can decrease Gb3 and lyso-Gb3 levels. However, the reference range for Gb3 is 4.6±2.0 ng/mL and that of lyso-Gb3 is <1.2±0.1 pg/mL, so the serum levels were still higher in the present study patients than in healthy people, even after ERT. Based on our results, it is possible that high Gb3 and lyso-Gb3 levels may affect the continually high HDL-C/T-Chol ratio, and thus vascular lesions, even after ERT.
Table 4.
Comparison of Serum Gb3 and Lyso-Gb3 Levels Before ERT and in the Latest Blood Test Results
| |
Threshold |
Before ERT
(n=16) |
Latest
(n=21) |
| Male |
| Gb3 concentration (ng/mL) |
4.6±2.0 |
15.7 (8.6–25.6) |
6.5 (6.0–11.0) |
| Lyso-Gb3 concentration (pg/mL) |
<1.2±0.1 |
83.4 (21.3–156.0) |
32.3 (26.7–40.3) |
| Female |
| Gb3 concentration (ng/mL) |
4.6±2.0 |
9.0 (5.5–11.3) |
5.6 (4.5–10.2) |
| Lyso-Gb3 concentration (pg/mL) |
<1.2±0.1 |
10.5 (6.7–14.2) |
6.8 (4.9–9.5) |
ERT, enzyme replacement therapy; Gb3, globotriosylceramide.
Discussion
In this study, we analyzed the correlations between serum cholesterol levels and vascular lesions in Fabry disease patients. Our results showed that these patients had a high HDL-C/T-Chol ratio, vascular hypertensive and arteriosclerotic changes of the fundus and high serum VEGF and ICAM-1 levels. In the study by Cartwright et al, the average of serum HDL-C concentration in male patients was 1.46 mmol/L and 1.93 mmol/L in female patients.15
Stepien et al also reported almost the same cholesterol levels.16
In our results, the male HDL-C level was 1.74 mmol/L, which was higher than in the 2 previous studies. So the high HDL-C level in our study is consistent and unlikely to be affected by ethnic differences.
Ocular vascular lesions and increased VEGF levels were observed more frequently in patients with a high HDL-C/T-Chol ratio, especially female patients, suggesting that the HDL-C/T-Chol ratio is related to vascular lesions. This high HDL-C/T-Chol ratio was observed from an early age and did not change even after ERT, which is consistent with previous research.15,16
Other studies have shown that accumulated Gb3 in vascular endothelial cells induces oxidative stress,29
reduces NO production29
and upregulates adhesion molecules and LDL-receptor expression.30,31
Moreover, KCa3.1, expressed in vascular endothelial cells, is downregulated by Gb3 accumulation, resulting in endothelial dysfunction.32
Based on these results, it is possible that a high HDL-C/T-Chol ratio is caused by increased endocytosis of LDL-C to the endothelial cells. Our results indicated that this endothelial dysfunction can start when young, even in heterozygote female patients. Considering that female patients with a high HDL-C/T-Chol ratio were more likely to show a high serum VEGF level, a high HDL-C/T-Chol ratio might reflect vascular endothelium dysfunction and arteriosclerotic changes, resulting in a more severe disease process.
Although the majority of patients in this study did not show hypertension, S1 and H1 in the Scheie classification and vascular tortuosity were commonly found, even in some young patients. Previous in vivo study using GLA knockout mice showed that lyso-Gb3 is a strong proliferation factor for vascular smooth muscle cells.33
Ocular vascular changes appear to reflect vascular wall thickening and narrowed vessel caliber. Other studies report increased basilar artery diameter in Fabry disease patients.34,35
In our study, serum lyso-Gb3 showed a significant decrease after ERT, but remained much higher than in healthy people, suggesting that present ERT protocols are still not effective enough because of high lyso-Gb3 levels. In fact, other ways of evaluating vascular lesions and endothelial functions, such as IMT and FMD, have not shown outstanding improvement after ERT.8
Recent in vitro studies suggested other mechanisms of vascular damage caused by this disease. In GLA-silencing cells, lipid raft domains show a significant increase.36
Because LDL-C is essential for lipid raft formation,37
LDL utilization might be increased in Fabry disease patients, which is likely to result in a relative increase of serum HDL-C. Moreover, the vascular tortuosity observed in this disease is likely to cause turbulent blood flow, which may contribute to the formation of focally distributed incipient atherosclerotic lesions.38
It is known that other lysosomal storage disorders are associated with HDL-C decrease. In Gaucher disease, this low HDL-C improves with ERT towards the normal range.39
In Niemann-Pick A, B and C disease, the HDL-C level is also low.40,41
One possible reason is the contribution of liver function. HDL-C is not only produced in peripheral tissues but also re-secreted by the liver. As with many other organs, liver function is affected in most lysosomal storage diseases, but not in Fabry disease,42
which may contribute to the high serum HDL-C level in this disease. However, further study is necessary to clarify more why HDL-C increases only in Fabry disease.
The limitation of this study is that the number of patients was small, especially those who had serum VEGF, ICAM-1, Gb3 and lyso-Gb3 levels measured. In addition, the relationships between the serum cholesterol profile and the risk of stroke, acute coronary syndrome etc. need to be further studied. By evaluating ocular vascular lesions or the serum VEGF level, we may be able to follow-up vascular damage. Despite these limitations, we believe our study sheds new light on Fabry disease, especially in relation to vascular damage.
Grants
No grants are provided in this study, but Kazuya Tsuboi receives consulting fee from Sumitomo Dainippon Pharma Co., Ltd.
Supplementary Files
Supplementary File 1
Figure S1.
Correlation between age and HDL/T-Chol ratio in Fabry disease patients.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-18-0378
References
- 1.
Zarate YA, Hopkin RJ. Fabry’s disease. Lancet 2017; 372: 1427–1435.
- 2.
Orssaud C, Dufier JL, Germain DP. Ocular manifestations in Fabry disease: A survey of 32 hemizygous male patients. Ophthalmic Genet 2003; 24: 129–139.
- 3.
MacDermot K, Holmes A, Miners A. Anderson-Fabry disease: Clinical manifestations and impact of disease in a cohort of 60 obligate carrier females. J Med Genet 2001; 38: 769–775.
- 4.
Hůlková H, Ledvinová J, Poupĕtová H, Bultas J, Zeman J, Elleder M. Postmortem diagnosis of Fabry disease in a female heterozygote leading to the detection of undiagnosed manifest disease in the family. Cas Lek Cesk 1999; 138: 660–664.
- 5.
Uchino M, Uyama E, Kawano H, Hokamaki J, Kugiyama K, Murakami Y, et al. A histochemical and electron microscopic study of skeletal and cardiac muscle from a Fabry disease patient and carrier. Acta Neuropathol 1995; 90: 334–338.
- 6.
Satoh K. Globotriaosylceramide induces endothelial dysfunction in Fabry disease. Arterioscler Thromb Vasc Biol 2013; 34: 2–4.
- 7.
Shen JS, Meng XL, Moore DF, Quirk JM, Shayman JA, Schiffmann R, et al. Globotriaosylceramide induces oxidative stress and up-regulates cell adhesion molecule expression in Fabry disease endothelial cells. Mol Genet Metab 2008; 95: 163–168.
- 8.
Rombach SM, van den Bogaard B, de Groot E, Groener JEM, Poorthuis BJ, Linthorst GE, et al. Vascular aspects of Fabry disease in relation to clinical manifestations and elevations in plasma globotriaosylsphingosine: Novelty and significance. Hypertension 2012; 60: 998–1005.
- 9.
Schiffmann R, Kopp JB, Austin III HA, Sabnis S, Moore DF, Weibel T, et al. Enzyme replacement therapy in Fabry disease. JAMA 2001; 285: 2743.
- 10.
Eng CM, Guffon N, Wilcox WR, Germain DP, Lee P, Waldek S, et al. Safety and efficacy of recombinant human α-galactosidase: A replacement therapy in Fabry’s disease. N Engl J Med 2001; 345: 9–16.
- 11.
Weidemann F, Niemann M, Breunig F, Herrmann S, Beer M, Störk S, et al. Long-term effects of enzyme replacement therapy on Fabry cardiomyopathy. Circulation 2009; 119: 524–529.
- 12.
Hughes DA, Elliott PM, Shah J, Zuckerman J, Coghlan G, Brookes J, et al. Effects of enzyme replacement therapy on the cardiomyopathy of Anderson-Fabry disease: A randomised, double-blind, placebo-controlled clinical trial of agalsidase alfa. Heart 2008; 94: 153.
- 13.
Elliott PM, Kindler H, Shah JS, Sachdev B, Rimoldi OE, Thaman R, et al. Coronary microvascular dysfunction in male patients with Anderson-Fabry disease and the effect of treatment with α galactosidase A. Heart 2006; 92: 357.
- 14.
Schiffmann R, Rapkiewicz A, Abu-Asab M, Ries M, Askari H, Tsokos M, et al. Pathological findings in a patient with Fabry disease who died after 2.5 years of enzyme replacement. Virchows Arch 2006; 448: 337–343.
- 15.
Cartwright DJ, Cole AL, Cousins AJ, Lee PJ. Raised HDL cholesterol in Fabry disease: Response to enzyme replacement therapy. J Inherit Metab Dis 2004; 27: 791–793.
- 16.
Stepien KM, Hendriksz CJ. Lipid profile in adult patients with Fabry disease: Ten-year follow up. Mol Genet Metab Rep 2017; 13: 3–6.
- 17.
Sacks FM. The role of high-density lipoprotein (HDL) cholesterol in the prevention and treatment of coronary heart disease: Expert group recommendations. Am J Cardiol 2017; 90: 139–143.
- 18.
Tsai WC, Li YH, Huang YY, Lin CC, Chao TH, Chen JH. Plasma vascular endothelial growth factor as a marker for early vascular damage in hypertension. Clin Sci 2005; 109: 39.
- 19.
Kitagawa K, Matsumoto M, Sasaki T, Hashimoto H, Kuwabara K, Ohtsuki T, et al. Involvement of ICAM-1 in the progression of atherosclerosis in APOE-knockout mice. Atherosclerosis 2002; 160: 305–310.
- 20.
Davies MJ, Gordon JL, Gearing AJH, Pigott R, Woolf N, Katz D, et al. The expression of the adhesion molecules ICAM-1, VCAM-1, PECAM, and E-selectin in human atherosclerosis. J Pathol 1993; 171: 223–229.
- 21.
Stehouwer C, Lambert J, Donker AJ, van Hinsbergh VW. Endothelial dysfunction and pathogenesis of diabetic angiopathy. Cardiovasc Res 1997; 34: 55–68.
- 22.
Zampetti A, Gnarra M, Borsini W, Giurdanella F, Antuzzi D, Piras A, et al. Vascular endothelial growth factor (VEGF-a) in Fabry disease: Association with cutaneous and systemic manifestations with vascular involvement. Cytokine 2013; 61: 933–939.
- 23.
Peng H, Xu X, Zhang L, Zhang X, Peng H, Zheng Y, et al. GLA variation p.E66Q identified as the genetic etiology of Fabry disease using exome sequencing. Gene 2016; 575: 363–367.
- 24.
Lee BH, Heo SH, Kim GH, Park JY, Kim WS, Kang DH, et al. Mutations of the GLA gene in Korean patients with Fabry disease and frequency of the E66Q allele as a functional variant in Korean newborns. J Hum Genet 2010; 55: 512–517.
- 25.
Scheie HG. Evaluation of ophthalmoscopic changes of hypertension and arteriolar sclerosis. AMA Arch Ophthalmol 1953; 49: 117–138.
- 26.
Nguyen TT, Gin T, Nicholls K, Low M, Galanos J, Crawford A. Ophthalmological manifestations of Fabry disease: A survey of patients at the Royal Melbourne Fabry Disease Treatment Centre. Clin Exp Ophthalmol 2005; 33: 164–168.
- 27.
Sher NA, Letson RD, Desnick RJ. The ocular manifestations in Fabry’s disease. Arch Ophthalmol 1979; 97: 671–676.
- 28.
Orssaud C, Dufier J, Germain D. Ocular manifestations in Fabry disease: A survey of 32 hemizygous male patients. Ophthalmic Genet 2003; 24: 129–139.
- 29.
Shu L, Park JL, Byun J, Pennathur S, Kollmeyer J, Shayman JA. Decreased nitric oxide bioavailability in a mouse model of Fabry disease. J Am Soc Nephrol 2009; 20: 1975–1985.
- 30.
Altarescu G, Moore DF, Pursley R, Campia U, Goldstein S, Bryant M, et al. Enhanced endothelium-dependent vasodilation in Fabry disease. Stroke 2001; 32: 1559–1562.
- 31.
Puri V, Jefferson JR, Singh RD, Wheatley CL, Marks DL, Pagano RE. Sphingolipid storage induces accumulation of intracellular cholesterol by stimulating SREBP-1 cleavage. J Biol Chem 2003; 278: 20961–20970.
- 32.
Park S, Kim JA, Joo KY, Choi S, Choi EN, Shin JA, et al. Globotriaosylceramide leads to KCa3.1 channel dysfunction: A new insight into endothelial dysfunction in Fabry disease. Cardiovasc Res 2011; 89: 290–299.
- 33.
Aerts JM, Groener JE, Kuiper S, Donker-Koopman WE, Strijland A, Ottenhoff R, et al. Elevated globotriaosylsphingosine is a hallmark of Fabry disease. Proc Natl Acad Sci USA 2008; 105: 2812–2817.
- 34.
Üçeyler N, Homola GA, Guerrero González H, Kramer D, Wanner C, Weidemann F, et al. Increased arterial diameters in the posterior cerebral circulation in men with Fabry disease. PLoS One 2014; 9: e87054.
- 35.
Fellgiebel A, Keller I, Martus P, Ropele S, Yakushev I, Böttcher T, et al. Basilar artery diameter is a potential screening tool for Fabry disease in young stroke patients. Cerebrovasc Dis 2011; 31: 294–299.
- 36.
Labilloy A, Youker RT, Bruns JR, Kukic I, Kiselyov K, Halfter W, et al. Altered dynamics of a lipid raft associated protein in a kidney model of Fabry disease. Mol Genet Metab 2014; 111: 184–192.
- 37.
Song J, Ping LY, Duong DM, Gao XY, He CY, Wei L, et al. Native low density lipoprotein promotes lipid raft formation in macrophages. Mol Med Rep 2016; 13: 2087–2093.
- 38.
Prado CM, Ramos SG, Elias J, Rossi MA, Rossi MA. Turbulent blood flow plays an essential localizing role in the development of atherosclerotic lesions in experimentally induced hypercholesterolaemia in rats. Int J Exp Pathol 2008; 89: 72–80.
- 39.
Cenarro A, Pocovi M, Giraldo P, Garcia-Otin AL, Ordovas JM. Plasma lipoprotein responses to enzyme-replacement in Gaucher’s disease. Lancet 1999; 353: 642–643.
- 40.
Choi HY, Karten B, Chan T, Vance JE, Greer WL, Heidenreich RA, et al. Impaired ABCA1-dependent lipid efflux and hypoalphalipoproteinemia in human Niemann-Pick type C disease. J Biol Chem 2003; 278: 32569–32577.
- 41.
McGovern MM, Pohl-Worgall T, Deckelbaum RJ, Simpson W, Mendelson D, Desnick RJ, et al. Lipid abnormalities in children with types A and B Niemann Pick disease. J Pediatr 2004; 145: 77–81.
- 42.
Meuwissen SGM, Dingemans KP, Strijland A, Tager JM, Ooms BCM. Ultrastructural and biochemical liver analyses in Fabry’s disease. Hepatology 2007; 2: 263S–268S.