Images in Cardiovascular Medicine
Clinical Utility of Fractional Flow Reserve on Computed Tomography in Left Main Trunk Disease
2018 Volume 82 Issue 3 Pages 930-931

Details
2018 Volume 82 Issue 3 Pages 930-931
Hemodynamic assessment of coronary artery disease (CAD) is important for performing appropriate percutaneous coronary intervention (PCI).
Fractional flow reserve on computed tomography (FFRCT) is a new technology provided by HeartFlow. This is an epoch-making analytical method that allows the data from standard coronary computed tomography angiography (CCTA) to yield hemodynamic assessment of CAD without invasive procedures.1
A 58-year-old woman with risk factors of type 2 diabetes mellitus and dyslipidemia developed chest discomfort on mild effort. Electrocardiography showed complete right bundle block, and ultrasound cardiography showed a normal left ventricular wall motion, while CCTA using a 320-row CT (Aquillion ONE, Toshiba Medical Systems, Ohtawara, Japan) showed severe stenosis in the distal left main trunk (LMT) bifurcation (Figure 1). In this case, adenosine 201Tl-myocardial perfusion imaging (MPI) showed no apparent perfusion defects in the left coronary area on MPI/CT fusion image (Figure 1) with summed stress score 2, summed rest score 0, and no transient ischemic dilatation. The washout rate of the present patient for adenosine 201Tl-myocardial perfusion image was 44.68% which was slightly lower than the normal washout rate of the present institution (Figure S1). This indicated no myocardial ischemia. On FFRCT analysis, however, FFR of the left descending artery (LAD), left circumflex artery (LCx) and right coronary artery (RCA) was 0.58, 0.75 and 0.92, respectively, indicating 2-vessel disease. Moreover, FFRCT clearly showed the most hemodynamically significant point as the distal LMT bifurcation on color mapping image (Figure 2). In this case, invasive coronary angiography (ICA) also showed a severe stenosis in the distal LMT bifurcation (MEDINA 1, 1, 1) similar to CCTA. Invasive FFR measured with pressure wire (Aeris PressureWire; St. Jude Medical, St. Paul, MN, USA) of the LAD and LCx was 0.72 and 0.71, respectively (Figure 2). Moreover, both FFR values were jumped up at the LMT bifurcation, and hence hemodynamically significant LMT disease (LMTD) was diagnosed. Finally, LMTD was treated with a 3.5×23-mm everolimus-eluting stent cross-over LCx.

Coronary computed tomography (CT) angiography showing severe stenosis in the distal left main trunk bifurcation. Adenosine 201Tl-myocardial perfusion imaging (MPI) shows no apparent perfusion defects in the left coronary area on MPI/CT fusion image.
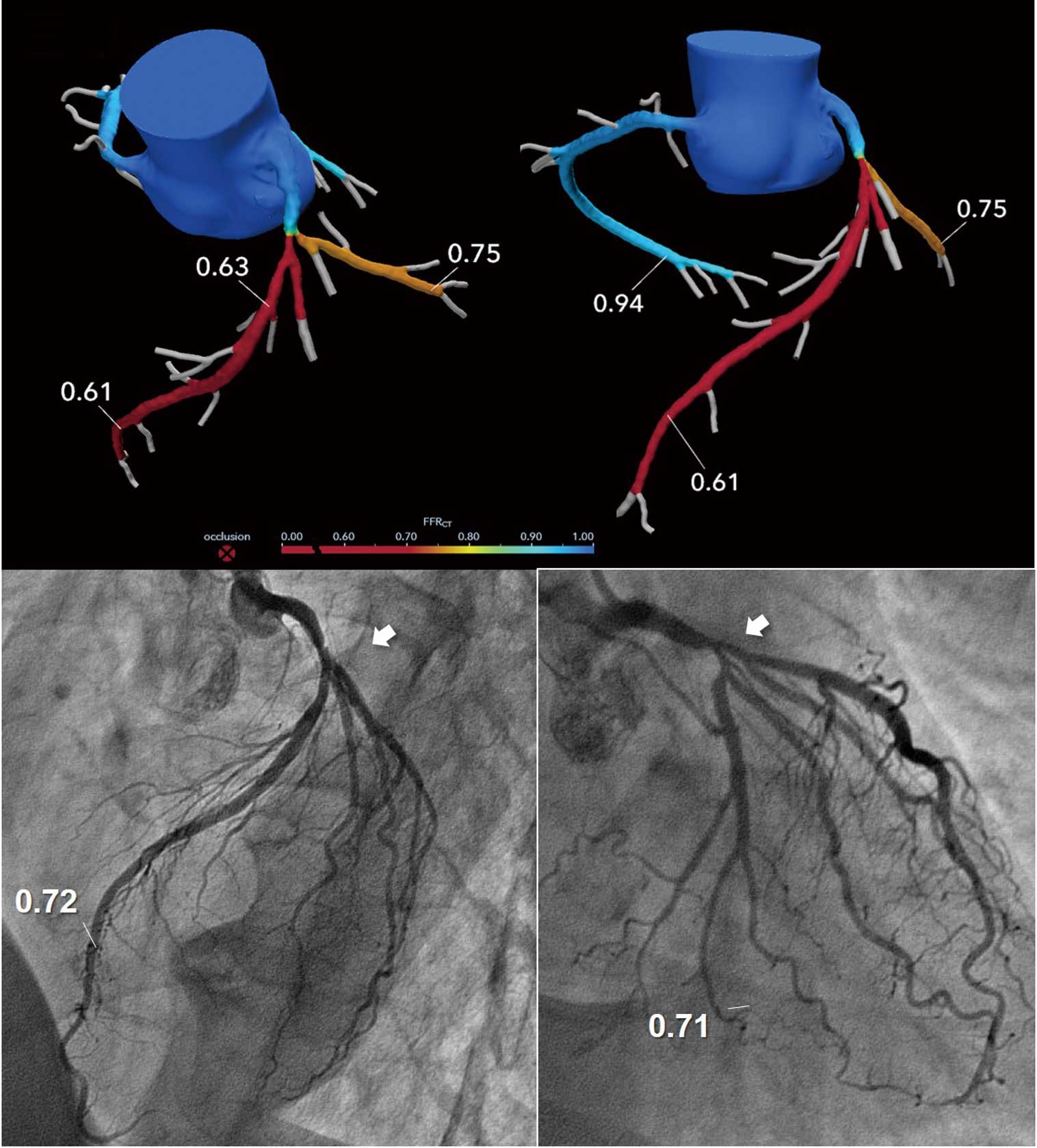
Fractional flow reserves (FFR) of the left descending artery (LAD), left circumflex artery (LCx) and right coronary artery (RCA) of 0.58, 0.75 and 0.92, respectively, on FFR computed tomography (FFRCT). The color mapping image clearly shows the most hemodynamically significant point as the distal left main trunk (LMT) bifurcation. Coronary angiography shows severe stenosis in the distal LM trunk bifurcation (white arrow). The invasive FFR of the LAD and LCx are 0.72 and 0.71, respectively.
Traditionally, stress MPI has been used to evaluate myocardial ischemia, but there is a limitation due to false negative results caused by balance ischemia2 in patients with multi-vessel disease including LMTD. Therefore, even if stress MPI was used to examine myocardial ischemia in patients with LMTD, ischemia would have been missed in 88%.3
Recently, FFR analysis using pressure wire has been widely recognized and used in the clinical field of interventional cardiology.4,5 FFR analysis can evaluate the hemodynamic significance of each diseased vessel without the influence of balance ischemia, but it requires an invasive procedure and drug stress test. In contrast, FFRCT analysis can be performed non-invasively without drug stress test, and both morphological and functional evaluation can be carried out simultaneously in the one modality. Moreover, it is not influenced by balance ischemia, similar to invasive FFR. Interestingly, in the present case the invasive FFR of the LAD and LCx were similar, suggesting the presence of balanced ischemia, and this may have been responsible for the negative stress MPI. This case suggests that FFRCT analysis will become a feasible and useful functional evaluation method compared with stress MPI in patients with LMTD.
The authors received no financial support from the manufacturer.
Supplementary File 1
Figure S1. The result of stress myocardial perfusion image.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-16-1183