Abstract
Background:
Heart failure (HF) is an important complication in adults with congenital heart disease (CHD), but because only a few studies have focused on acute HF hospitalization in adults with CHD, we study aimed to define the clinical characteristics of such patients and examine the differences in acute HF between adults with CHD and acquired heart disease.
Methods and Results:
We retrospectively evaluated 50 adults with CHD admitted for treatment of acute HF and compared their data with those from Japanese HF registries. Patient mean age was 37±15 years and 58% were male. In total, 86% of the patients had complex forms of CHD and 62% had undergone corrective surgery, including the Fontan procedure; 66% of patients showed right heart hemodynamic abnormality. In-hospital mortality was 4%, which was comparable to the Japanese HF registries. Survival rate was 93% at 1 year and 75% at 3 years, which was similarly poor to the rates of HF secondary to acquired heart disease.
Conclusions:
We clarified the clinical characteristics of adults with CHD requiring HF hospitalization. Young adults with complex CHD were hospitalized for management of acute right HF. Short-term and mid-term outcomes were similarly poor compared with acute HF secondary to acquired heart disease.
Congenital heart disease (CHD) is a common birth defect affecting approximately 1% of newborns.1,2
Because of advances in heart surgery and cardiac care for infants and children with CHD, 90% of patients with CHD may survive into adulthood,3
which has led to a growing population of adults with CHD.2
Many of these patients remain at risk of sequelae, including arrhythmia, heart failure (HF), thromboembolism, pulmonary hypertension, endocarditis, and premature death.4,5
A previous report showed increased mortality rates in adults with CHD; the vast majority of whom died from cardiovascular causes, particularly HF.6
The characteristics, clinical presentation, treatment, and outcomes of patients hospitalized with worsening HF have been well-documented based on data from large-scale in-patient hospital registries.7,8
Most cases of HF were secondary to acquired heart disease in almost all registries. Acute HF in adults with CHD may have different characteristics, outcomes, and risk factors for death compared with HF of acquired heart disease etiology. However, only a few studies have focused on acute HF hospitalization in adults with CHD.9
Therefore the objectives of the present study were (1) to clarify the clinical characteristics, management, and outcomes of adults with CHD hospitalized for acute HF; and (2) to evaluate the differences in these factors in acute HF between adults with CHD and those with acquired heart disease.
Methods
The study protocol was approved by the Ethics Committee of the National Cerebral and Cardiovascular Center. We assert that all procedures contributing to this work complied with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Study subjects included 1,363 CHD patients aged 18 years or older hospitalized during a 9-year period from January 2005 to December 2013. We identified 50 patients admitted for treatment of acute HF. The diagnosis was based on clinical presentation of the modified Framingham HF criteria.10,11
Patients diagnosed with protein-losing enteropathy were excluded because those symptoms can resemble HF. Medical records were thoroughly reviewed and provided that data, including demographics, presence of underlying CHD, comorbidities, clinical status, laboratory data, echocardiography, treatment, medication use before hospitalization and at discharge, and in-hospital death. We reviewed post-discharge deaths and major cardiac adverse events (MCAE), which included acute HF symptoms, arrhythmic events, hemostatic events, surgical intervention, and development of protein-losing enteropathy requiring hospitalization.
We also compared these data with those from Japanese HF registries, including the acute decompensated HF syndromes (ATTEND) registry,11
the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD),12
and the Heart Institute of Japan-Department of Cardiology (HIJC)-HF Registry.13
Statistical Analysis
Data are expressed as mean±standard deviation for normally distributed variables, and median and range for non-normally distributed variables. Categorical variables are presented as percentages.
The survival rate was assessed using the Kaplan-Meier method. Cox regression analysis was used to assess event-predictive factors. Significant differences observed in univariate analyses were assessed by multivariate analyses. JMP 10 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses. Differences of P<0.05 were considered statistically significant.
Results
Patients’ Characteristics
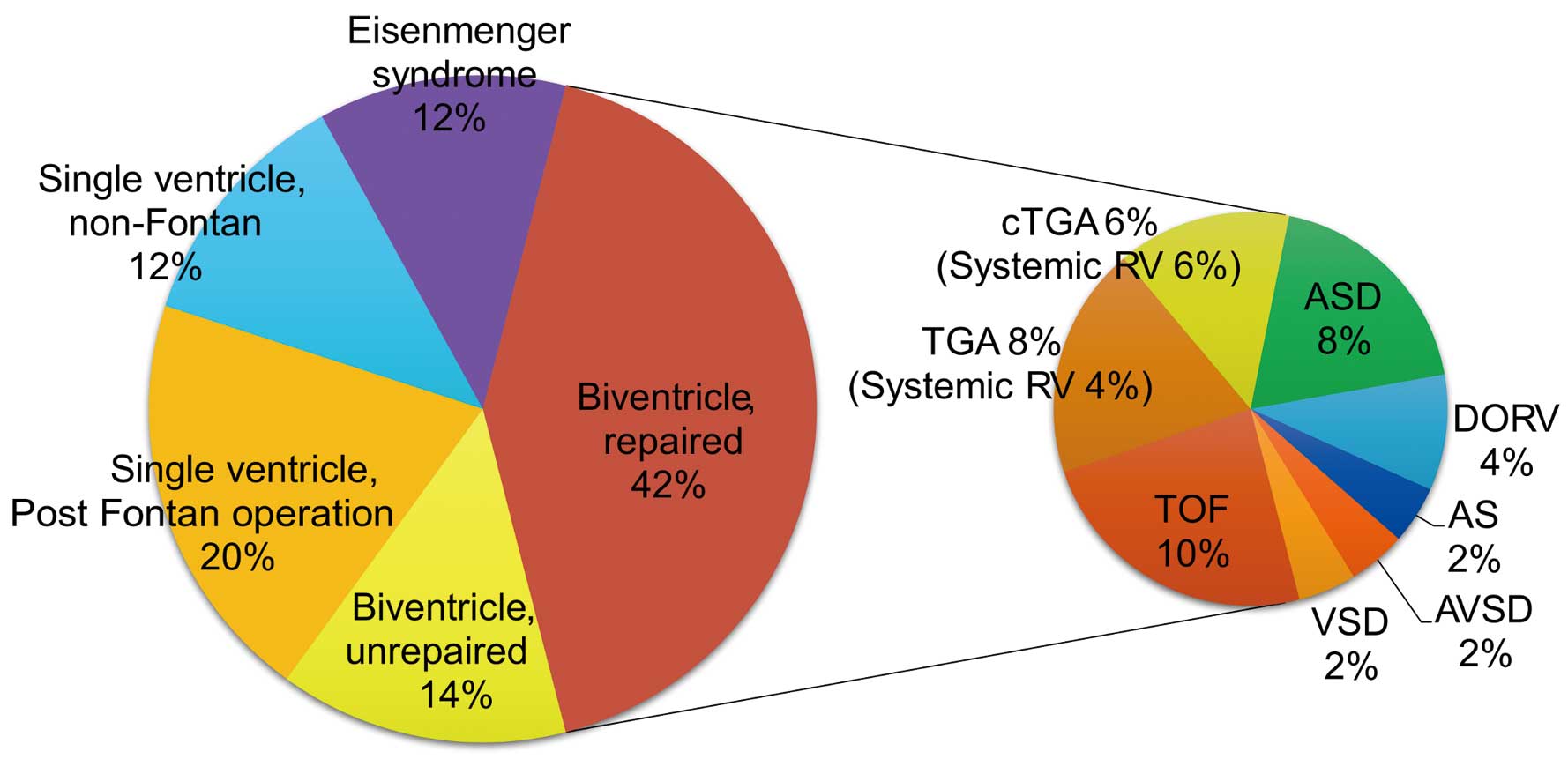
The mean age of the 50 study patients was 37±15 years and 58% were male (Table 1). Data on the prevalence of each underlying CHD in study patients are presented in
Figure 1. Patients with biventricular physiology, single-ventricular physiology, and Eisenmenger syndrome were 56%, 32%, and 12%, respectively. In total, 86% of the patients had complex forms of CHD and 62% of the patients had undergone corrective surgery, including the Fontan procedure. In cases of biventricular physiology with corrective surgery, 4 patients (8%) had transposition of the great arteries, 2 of them had undergone arterial switch operations, and the others had undergone atrial switch operations; 3 patients with congenitally-corrected transposition of the great arteries had undergone functional repair.
Table 1.
Characteristics of the Patients in the Current Study vs. Those in Existing Japanese Registries
| Characteristic |
Current study |
ATTEND |
JCARE-CARD |
HIJC-HF |
| No. of patients, n |
50 |
1,110 |
1,677 |
3,578 |
| Age, years |
37±15*,**,*** |
73±14 |
71±14 |
70±13 |
| Male sex, % |
58 |
59 |
59 |
59 |
| SpO2 <90% |
38 |
NA |
NA |
NA |
| Prior HF hospitalization, % |
28** |
37 |
50 |
34 |
| History of atrial arrhythmia, % |
40 |
40 |
35 |
36 |
| Pacemaker implantation, % |
28 |
NA |
NA |
NA |
| Diabetes mellitus, % |
20* |
34 |
30 |
31 |
| Dyslipidemia, % |
10**,*** |
NA |
26 |
26 |
P<0.05, *vs. ATTEND, **vs. JCARE-CARD, ***vs. HIJC-HF. HF, heart failure; SpO2, oxygen saturation.
The characteristics of the patients included in this study were compared with those in ATTEND, JCARE-CARD, and HIJC-HF (Table 1). Mean patient age in the present study was lower than in the Japanese HF registries. In all 4 samples (current study and 3 studies from the Japanese registries), approximately 60% of patients were male. The prevalence of atrial arrhythmia was similar among the compared studies (40% in this study vs. 40% in ATTEND, 35% in JCARE-CARD and 36% in HIJC-HF). The prevalence of diabetes mellitus in this study (20%) was significantly lower than in ATTEND registry (34%, P<0.05); however, this was not significant when compared with JCARE-CARD (30%, P>0.05) and HIJC-HF (31%, P>0.05). Additionally, the prevalence of dyslipidemia was significantly lower in this study (10% vs. 26% in JCARE-CARD and 26% in HIJC-HF, P<0.05; dyslipidemia data unavailable for ATTEND).
Clinical Profile on Admission
Major symptoms and clinical data are shown in
Table 2. Most patients were in NYHA functional class III or IV and 60–70% had dyspnea and/or peripheral edema. These findings were similar among studies. Only 16% of patients in the present study had rales, compared with 52–78% of patients in ATTEND and JCARE-CARD. Blood pressure and heart rate were significantly lower in the patients in the present study. On surface ECG, 28% of patients showed atrial tachycardia (AT) or atrial fibrillation (AF), whereas 38% showed this arrhythmia on ATTEND. Laboratory data were also different from those of the patients in ATTEND and JCARE-CARD. Lower levels of B-type natriuretic peptide (BNP), sodium, and serum creatinine, as well as higher estimated glomerular filtration rate and hemoglobin concentration were observed in ACHD with HF.
Table 2.
Clinical Profile of Study Patients on Admission in Current Study vs. Existing Japanese Registries
| |
Current study |
ATTEND |
JCARE-CARD |
| Dyspnea on ordinal exertion, % |
64 |
NA |
67 |
| Rales, % |
16*,** |
78 |
52 |
| Ankle edema, % |
68** |
68 |
53 |
| Clinical scenario 1/2/3/4/5, % |
2/20/8/0/70 |
NA |
NA |
| Body mass index, kg/m2 |
21±4 |
NA |
22±4 |
| Systolic BP, mmHg |
109±16*,** |
147±38 |
134±30 |
| Diastolic BP, mmHg |
65±10** |
NA |
75±18 |
| Heart rate, beats/min |
81±15*,** |
99±30 |
88±24 |
| NYHA functional class (I/II/III/IV), % |
0/16/58/26 |
1/12/39/47 |
1/11/46/43 |
| Electrocardiography |
| AT/AF, % |
28* |
38 |
NA |
| Blood examination |
| BNP, pg/mL |
456±467*,** |
1,063±1,158 |
878±929 |
| Na, mEq/L |
138±4** |
NA |
140±5 |
| Cre, mg/dL |
0.8±0.3*,** |
1.4±1.5 |
1.3±1.0 |
| eGFR, mL/min/1.73 m2 |
88±34** |
NA |
53±25 |
| Hemoglobin, g/dL |
14±3* |
NA |
12±5 |
| Echocardiography |
| Reduced EF, % |
24* |
57 |
NA |
| AVVR ≥moderate, % |
20 |
NA |
NA |
| AR ≥moderate, % |
0 |
NA |
NA |
| TR ≥moderate, % |
41 |
NA |
NA |
| PR ≥moderate, % |
33 |
NA |
NA |
| RA dilation, % |
62 |
NA |
NA |
| RV dilation, % |
51 |
NA |
NA |
P<0.05, *vs. ATTEND, **vs. JCARE-CARD, ***vs. HIJC-HF. AF, atrial fibrillation; AR, aortic regurgitation; AT, atrial tachycardia; AVVR, atrioventricular valve regurgitation; BNP, B-type natriuretic peptide; BP, blood pressure; EF, ejection fraction; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association; PM, pacemaker rhythm; PR, pulmonary regurgitation; RA, right atrium; RV, right ventricle; SR, sinus rhythm; TR, tricuspid regurgitation.
In this study, only 24% of patients showed reduced systemic ventricular contraction compared with 57% in ATTEND. Moreover, as much as 66% of patients showed right heart hemodynamic abnormalities, such as Fontan circulation, Eisenmenger syndrome, at least moderate pulmonary regurgitation, and at least moderate tricuspid regurgitation, on echocardiography.
In-Hospital Management
In-hospital management and outcomes are summarized in
Table 3; 44% of patients were treated with intravenous loop diuretics and the remainder took loop diuretics orally. Carperitide was less frequently administered in the present study (22%) compared with ATTEND (69%) and JCARE-CARD (34%). Use of inotropes was similar among the databases compared. Of the patients with AT or AF (28%), 8% had an acute onset; they underwent direct cardioversion and recovered to sinus rhythm or atrial pacing rhythm. The remaining 20% of patients with chronic AT or AF continued with heart rate control and anticoagulation therapy. None of the patients underwent surgical intervention during the same admission. However, 5 of the 48 discharged patients were planned for surgical intervention after discharge.
Table 3.
In-Hospital Management and Outcomes in the Current Study vs. Existing Japanese Registries
| |
Current study |
ATTEND |
JCARE-CARD |
| In-hospital management |
| Diuretics IV, % |
44*,** |
80 |
96 |
| Carperitide, % |
22* |
69 |
34 |
| Dobutamine, % |
12 |
13 |
13 |
| Dopamine, % |
4** |
11 |
20 |
| PDE3 inhibitor, % |
4 |
4 |
5 |
| DCCV, % |
8 |
NA |
NA |
| Surgical intervention, % |
0*,** |
4† |
9‡ |
| Outcome |
| Hospital stay (median), days |
28*,** |
21 |
15 |
| Hospital death, % |
4 |
8 |
6 |
P<0.05, *vs. ATTEND, **vs. JCARE-CARD. †Coronary artery bypass grafting, valve replacement, percutaneous cardiopulmonary support and left ventricular assist system; ‡coronary artery bypass. DCCV, direct current cardioversion; PDE3, phosphodiesterase 3.
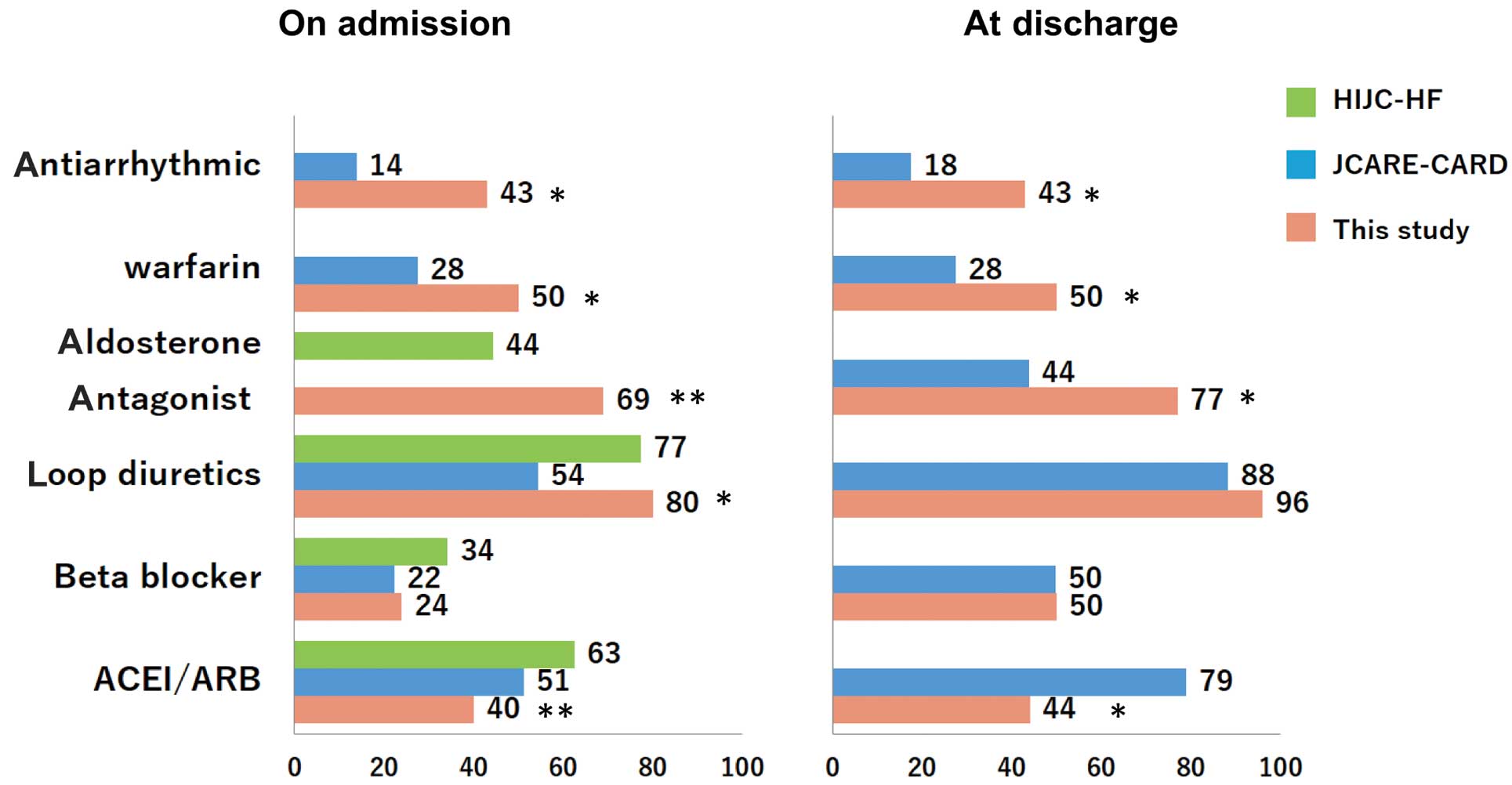
Rates of prescribed medications before hospitalization and at discharge are shown in
Figure 2. At both time points, the prescription rates of diuretics and β-blockers were similar to those in JCARE-CARD and HIJC-HF. The use of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers was lower in the present study.
Length of Stay and In-Hospital Mortality
Median length of hospital stay was 28 days in the present study (Table 3), which was significantly longer than in ATTEND (21 days) or JCARE-CARD (15 days (P<0.05, respectively). In-hospital mortality rates were comparable (present study (4.0%), ATTEND (7.7%), and JCARE-CARD (5.6%)).
Long-Term Morbidity and Mortality
During the median follow-up period of 2.8 years, 79% of patients experienced MCAE and 29% of patients died; 71% of MCAE patients were re-hospitalized because of HF and 57% died from progressive HF. The MCAE-free survival rate calculated by the Kaplan-Meier method was 58% at 1 year and 31% at 3 years (Figure 3A); the survival rate was 93% at 1 year and 75% at 3 years (Figure 3B). This was similarly poor to HF secondary to acquired heart disease (HIJC-HF registry, 1 year; 93.7%, 3 years; 70.8%). No significant predictors of MCAE were identified (Table 4). At least moderate atrioventricular valve regurgitation and non-use of angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers were independent predictors of death (Table 5).
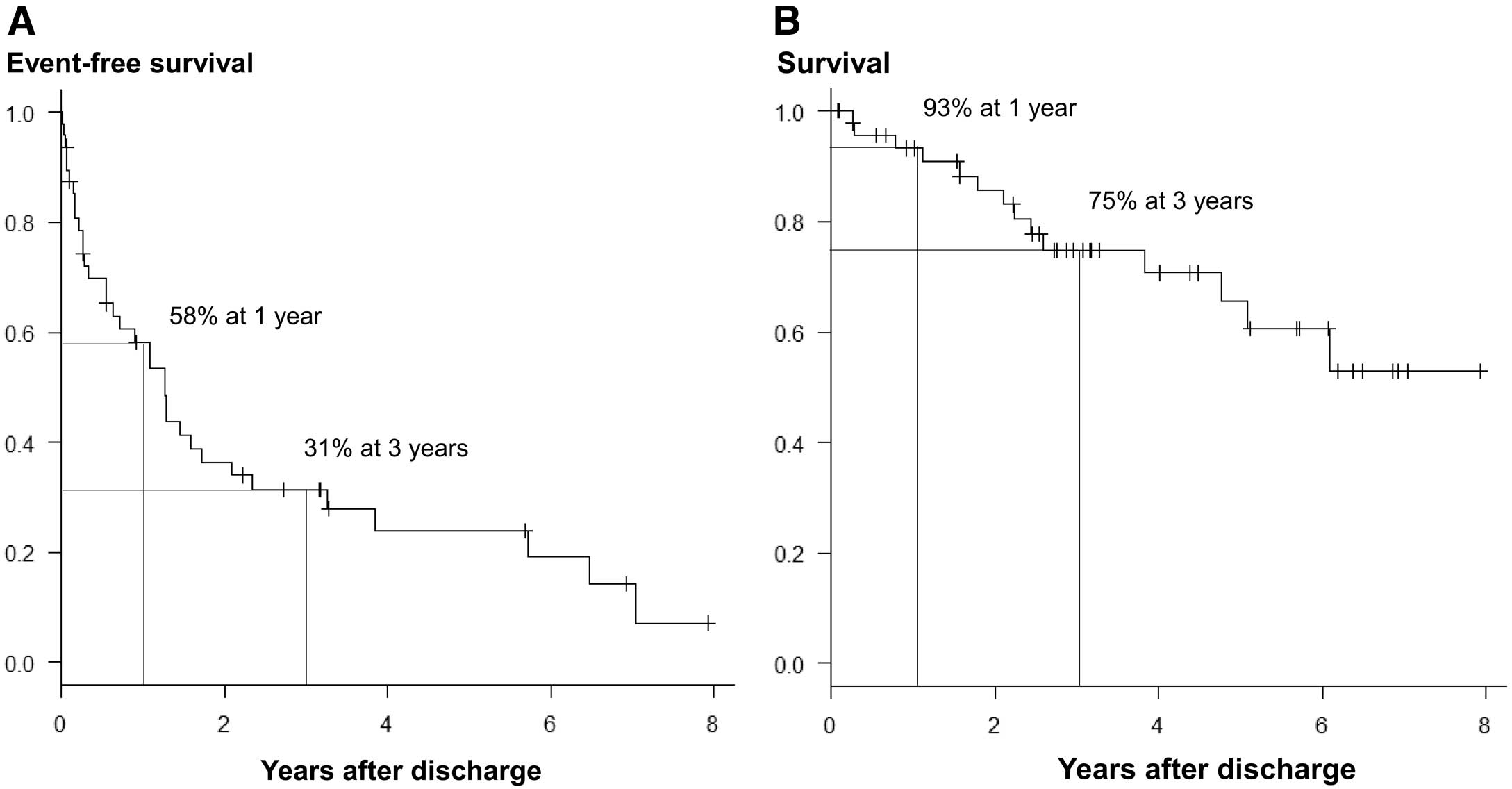
Table 4.
Univariate Predictors of Event-Free Survival After Discharge
| |
HR |
95% CI |
P value |
| Age |
1.00 |
0.98–1.02 |
NS |
| SV physiology |
1.33 |
0.65–2.66 |
NS |
| Systemic right ventricle |
1.34 |
0.53–3.03 |
NS |
| Pulmonary hypertension |
1.02 |
0.43–2.16 |
NS |
| SpO2 <90% |
1.15 |
0.57–2.27 |
NS |
| BNP at discharge, per 10 pg/mL |
1.01 |
1.00–1.02 |
NS |
| Na at discharge |
0.95 |
0.86–1.05 |
NS |
| Cre at discharge |
1.66 |
0.66–3.40 |
NS |
| Reduced EF |
1.01 |
0.42–2.15 |
NS |
| AVVR ≥moderate |
1.35 |
0.30–4.61 |
NS |
| TR ≥moderate |
1.27 |
0.58–2.58 |
NS |
| PR ≥moderate |
1.08 |
0.45–2.31 |
NS |
| ACEI/ARB use at discharge |
0.84 |
0.42–1.63 |
NS |
| β-blocker use at discharge |
1.22 |
0.62–2.41 |
NS |
| Loop diuretic use at discharge |
0.81 |
0.24–5.01 |
NS |
| Male sex |
1.39 |
0.69–2.81 |
NS |
| Pacemaker implantation |
1.94 |
0.91–3.98 |
NS |
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; CI, confidence interval; HR, hazard ratio. Other abbreviations as in Tables 1,2.
Table 5.
Univariate and Multivariate Predictors of Survival After Discharge
| |
Univariate analysis |
Multivariate analysis |
| HR |
95% CI |
P value |
HR |
95% CI |
P value |
| Age |
1.01 |
0.99–1.05 |
NS |
|
|
|
| SV physiology |
1.67 |
0.55–4.80 |
NS |
|
|
|
| Systemic RV |
0.36 |
0.02–1.79 |
NS |
|
|
|
| Pulmonary hypertension |
1.59 |
0.49–4.64 |
NS |
|
|
|
| SpO2 <90% |
1.95 |
0.66–5.72 |
NS |
|
|
|
| BNP at discharge, per 10 pg/mL |
1.01 |
1.00–1.02 |
0.06 |
|
|
|
| Na at discharge |
1.01 |
0.86–1.28 |
NS |
|
|
|
| Cre at discharge |
3.96 |
1.06–12.4 |
<0.05 |
2.63 |
0.78–10.2 |
NS |
| Reduced EF |
1.04 |
0.23–3.33 |
NS |
|
|
|
| AVVR ≥moderate |
3.51 |
1.13–10.6 |
<0.05 |
4.52 |
1.22–15.8 |
<0.05 |
| TR ≥moderate |
1.05 |
0.29–3.16 |
NS |
|
|
|
| PR ≥moderate |
0.54 |
0.12–1.78 |
NS |
|
|
|
| ACEI/ARB use at discharge |
0.29 |
0.07–0.94 |
<0.05 |
0.14 |
0.03–0.52 |
<0.05 |
| β-blocker use at discharge |
0.52 |
0.14–1.57 |
NS |
|
|
|
| Loop diuretic use at discharge |
0.17 |
0.04–1.18 |
NS |
|
|
|
| Male sex |
1.61 |
0.54–4.83 |
NS |
|
|
|
| Pacemaker implantation |
1.48 |
0.40–4.46 |
NS |
|
|
|
Abbreviations as in Tables 1,2,4.
Discussion
In this study, we clarified the clinical characteristics of adults with CHD requiring HF admission. Young adults with complex CHD were hospitalized for management of acute right HF. Short-term and mid-term outcomes were similarly poor compared with acute HF secondary to acquired heart disease.
Adults with CHD are a young, growing population. Aging is a risk factor for developing HF.14
The prevalence of adult CHD patients with HF is expected to increase and this influences the care of these patients. A report from the CONCOR registry showed that univentricular hearts, congenitally- and surgically-corrected transposition of the great arteries, multiple defects, surgical interventions, and pacemaker implants were risk factors for HF admission.9
Similarly, we found that single-ventricular physiologies and systemic right ventricles were the most common underlying causes of heart disease; we also found a high frequency of pacemaker implantation. More aggressive treatment against HF development (including cases of ventricular dyssynchrony, arrhythmia, or valve dysfunction) may be needed to prevent HF admission in these patients.
Compared with non-CHD HF patients, the adult CHD patients with HF had different hemodynamics and mechanisms underlying the development of HF. Our data clearly showed a predominance of right-sided HF in adults with CHD, whereas the incidence of non-CHD HF mainly consisted of left-sided HF. However, diuretic therapy was the main type of in-hospital management similar to that in cases of HF in patients with acquired heart disease and oral medication use at discharge was also similar to that of HF patients with acquired heart disease, with the exception of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. Lower rates of prescribing renin-angiotensin-aldosterone system (RAAS) inhibitors might be related to the considerably lower blood pressure in adult patients with CHD. Similar to HF patients with acquired heart disease, neurohormonal activation has been well demonstrated in patients with CHD.15
However, efficacy of neurohormonal blockage in patients with CHD remains unclear16
and must be elucidated.
Short-term and mid-term outcomes were similarly poor for acute HF secondary to acquired heart disease. Zomer et al reported a 3-year mortality rate of adult CHD patients with HF of 35%.9
In the current study, the 3-year mortality rate was considerably lower (25%), which may be because of the younger patient population (37 vs. 47 years) and differences in the medical care system between Japan and Western countries. Indeed, a Japanese registry of non-CHD HF patients also showed a lower mortality rate compared with European and US registries.13
In this study, atrioventricular valve regurgitation and non-use of RAAS inhibitors were related to death. Zomer et al reported the following to be independent predictors of 3-year mortality in adult CHD patients hospitalized for HF: male sex, pacemaker implantation, length of hospital stay, use of non-cardiac medications, and high serum creatinine concentrations.9
In addition, analysis of large-scale in-patient hospital registries has identified several risk factors for death in HF patients with acquired heart disease etiology, including elevated BNP,17
anemia,18
diuretic use at discharge,19
and hyponatremia.20
Further studies are needed to elucidate the prognostic effect of these risk factors in adult CHD patients to ensure better long-term outcomes for these patients.
Study Limitations
To begin with, it was a retrospective study, conducted at a single institution with a small patient population. Also, with advances in medical treatments, the therapeutic strategy may have varied over the study period. Furthermore, we used a classical definition of HF to identify the study patients. Adults with CHD have different hemodynamics and mechanisms underlying the development of HF compared with non-CHD patients. A definition of HF that is applicable to patients with CHD is needed for further comparison of these populations.
Conclusions
We clarified the clinical characteristics of adults with CHD requiring HF admission. Young adults with complex CHD were hospitalized for management of acute right HF. Both the short-term and mid-term outcomes were similarly poor in patients with CHD compared with those for patients with acute HF secondary to acquired heart disease. Though adults with CHD are an anatomically heterogeneous group and account for a small percentage of HF patients, they are a young and ever-growing population that is beginning to age. As such, their medical care also continues to increase. Prevention, early diagnosis, and establishment of a treatment strategy for HF in adults with CHD should be emphasized.
References
- 1.
Sissman NJ. Incidence of congenital heart disease. JAMA 2001; 285: 2579–2580.
- 2.
Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation 2014; 130: 749–756.
- 3.
Moons P, Bovijn L, Budts W, Belmans A, Gewillig M. Temporal trends in survival to adulthood among patients born with congenital heart disease from 1970 to 1992 in Belgium. Circulation 2010; 122: 2264–2272.
- 4.
Engelfriet P, Boersma E, Oechslin E, Tijssen J, Gatzoulis MA, Thilen U, et al. The spectrum of adult congenital heart disease in Europe: Morbidity and mortality in a 5 year follow-up period: The Euro Heart Survey on adult congenital heart disease. Eur Heart J 2005; 26: 2325–2333.
- 5.
Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Circulation 2008; 118: e714–e833.
- 6.
Verheugt CL, Uiterwaal CS, van der Velde ET, Meijboom FJ, Pieper PG, van Dijk AP, et al. Mortality in adult congenital heart disease. Eur Heart J 2010; 31: 1220–1229.
- 7.
Adams KF Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 2005; 149: 209–216.
- 8.
Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur Heart J 2006; 27: 2725–2736.
- 9.
Zomer AC, Vaartjes I, van der Velde ET, de Jong HM, Konings TC, Wagenaar LJ, et al. Heart failure admissions in adults with congenital heart disease; risk factors and prognosis. Int J Cardiol 2013; 168: 2487–2493.
- 10.
McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: The Framingham study. N Engl J Med 1971; 285: 1441–1446.
- 11.
Sato N, Kajimoto K, Asai K, Mizuno M, Minami Y, Nagashima M, et al. Acute decompensated heart failure syndromes (ATTEND) registry. A prospective observational multicenter cohort study: Rationale, design, and preliminary data. Am Heart J 2010; 159: 949–955.
- 12.
Hamaguchi S, Kinugawa S, Tsuchihashi-Makaya M, Goto D, Yamada S, Yokoshiki H, et al. Characteristics, management, and outcomes for patients during hospitalization due to worsening heart failure: A report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD). J Cardiol 2013; 62: 95–101.
- 13.
Kawashiro N, Kasanuki H, Ogawa H, Matsuda N, Hagiwara N. Clinical characteristics and outcome of hospitalized patients with congestive heart failure: Results of the HIJC-HF registry. Circ J 2008; 72: 2015–2020.
- 14.
Rodriguez FH 3rd, Moodie DS, Parekh DR, Franklin WJ, Morales DL, Zafar F, et al. Outcomes of heart failure-related hospitalization in adults with congenital heart disease in the United States. Congenit Heart Dis 2013; 8: 513–519.
- 15.
Bolger AP, Sharma R, Li W, Leenarts M, Kalra PR, Kemp M, et al. Neurohormonal activation and the chronic heart failure syndrome in adults with congenital heart disease. Circulation 2002; 106: 92–99.
- 16.
van der Bom T, Winter MM, Bouma BJ, Groenink M, Vliegen HW, Pieper PG, et al. Effect of valsartan on systemic right ventricular function: A double-blind, randomized, placebo-controlled pilot trial. Circulation 2013; 127: 322–330.
- 17.
Fonarow GC, Peacock WF, Horwich TB, Phillips CO, Givertz MM, Lopatin M, et al. Usefulness of B-type natriuretic peptide and cardiac troponin levels to predict in-hospital mortality from ADHERE. Am J Cardiol 2008; 101: 231–237.
- 18.
Hamaguchi S, Tsuchihashi-Makaya M, Kinugawa S, Yokota T, Takeshita A, Yokoshiki H, et al. Anemia is an independent predictor of long-term adverse outcomes in patients hospitalized with heart failure in Japan. A report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD). Circ J 2009; 73: 1901–1908.
- 19.
Hamaguchi S, Kinugawa S, Tsuchihashi-Makaya M, Goto D, Yamada S, Yokoshiki H, et al. Loop diuretic use at discharge is associated with adverse outcomes in hospitalized patients with heart failure: A report from the Japanese cardiac registry of heart failure in cardiology (JCARE-CARD). Circ J 2012; 76: 1920–1927.
- 20.
Hamaguchi S, Kinugawa S, Tsuchihashi-Makaya M, Matsushima S, Sakakibara M, Ishimori N, et al. Hyponatremia is an independent predictor of adverse clinical outcomes in hospitalized patients due to worsening heart failure. J Cardiol 2014; 63: 182–188.