Editorials
Left Ventricular Fiber Structure and Myocardial Deformation for Assessment of Cardiotoxicity
2018 Volume 82 Issue 3 Pages 648-649


Details
2018 Volume 82 Issue 3 Pages 648-649
LVEF is the most widely used parameter for the determination of LV dysfunction. Because early anthracycline-induced myocardial injury does not necessarily decrease LVEF, most researchers dispute its use as a reliable clinical parameter for the early detection of cardiotoxicity in patients receiving anthracyclines.1–3 Anthracycline-induced myocardial injury can lead to myocardial fibrosis and subsequently alterations of myocardial deformation prior to the occurrence of changes in the LVEF.1,3 Researchers are most concerned with exploring parameters for myocardial deformation that can predict earlier cardiotoxicity during or following therapy. Among the clinically available parameters is echocardiographic strain, which is based on tissue Doppler echocardiography or speckle-tracking technique. It is a novel parameter that represents 2D or 3D myocardial deformation with high spatial and temporal resolution4 and on which a significant amount of research has been conducted to evaluate the usefulness of strain for the early determination of anthracycline-induced cardiotoxicity. Strain has 3D directionality and is classified as radial, longitudinal, and circumferential. Previous studies report that longitudinal strain is predominantly impaired earlier than the other strain values2–4 and that myocardial damage starts from the endocardium and extends to the epicardium, which can be detected earlier by assessing the longitudinal rather than the circumferential strain.5 Because the superiority of longitudinal strain in the early detection of cardiotoxicity has been emphasized by several studies, those findings may require further investigation. In this issue of the Journal, Yazaki et al explain that a detailed understanding of the myocardial fiber structure and its arrangement in the developing heart may provide definitive insights to explain such issues.5
Article p 715
LV Myocardial Fiber Structure and FunctionTheir study used high spatial and temporal resolution 2D strain imaging with the aim of elucidating the mechanism of LV dysfunction caused by chemotherapy and to provide new insights into the myocardial layer-specific deformation following anthracycline treatment in patients with childhood cancers. A valuable finding from their study was that myocardial damage started in the endocardium at the base and extended towards the epicardium and apex with age.5 The 2D strain echocardiography enabled analysis of layer-specific myocardial deformation. Previously, Uematsu et al reported that a myocardial velocity gradient existed in the LV wall, which was related to its function.6 To the best of our knowledge, this is the first to assess layer-specific myocardial function. However, the measurement of myocardial velocity was performed using tissue Doppler. Accordingly, it was Doppler angle-dependent and therefore difficult to track the fixed position set as the region of interest. The development of the speckle-tracking technique brought about a revolutionary change in the assessment of cardiac wall motion with high spatial and temporal resolution and allowed the measurement of contractions in specific layers of the myocardium. In our previous animal study, we reported a myocardial strain rate gradient in the wall, which decreased from the endocardium towards the epicardium (Figure).7 Furthermore, they appeared in isovolumic contraction and relaxation cycles and correlated with hemodynamic changes. In regard to the structure of the myocardial fibers, it is reasonable to analyze endomyocardial strain for early detection of LV dysfunction. As the authors discuss, the LV myocardial fibers have a helical and triple-layered structure that distributes each fiber at an angle of approximately 60 degrees.8 Novel magnetic resonance imaging technology enables visualization of the structure of the myocardial fibers in real time.9 The distribution of myocardial fibers is different within the ventricular wall, with longitudinally oriented fibers predominantly in the endocardial region. However, the present authors speculate the reason why longitudinal strain remains stable during the early stage of anthracycline-induced cardiotoxicity is the dependency of endomyocardial deformation on the active and passive motion of the other adjacent layers. Similar to other reports, we have concluded that impairment of longitudinal LV contractions occurs earlier than that of global LV contractions.10,11 In the present authors’ study, the circumferential endomyocardial strain at the base, which decreased during the earlier stages following anthracycline treatment, was a more sensitive indicator than the other strains. Histologically, the myocardial fibers in the endocardial region that are closer to the base are arranged in a direction similar to that of the circumferential strain.12 This may explain their lower susceptibility to contractions of adjacent longitudinal fibers.
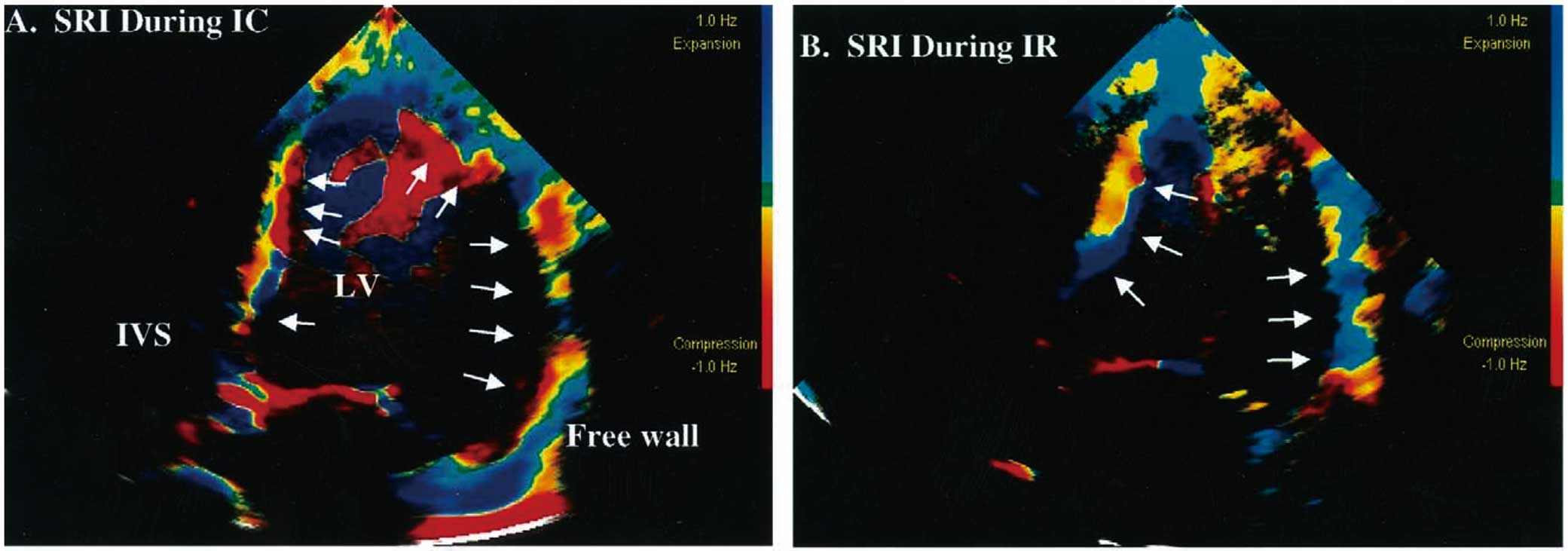
Strain rate imaging during isovolumic contraction time (A) and isovolumic relaxation time (B). Left ventricular (LV) tissue is inhomogeneously colored on strain rate imaging (SRI). The solid arrows indicate the subendocardium, which is deeply colored. IVS, interventricular septum.
The high spatial and temporal resolution of the echocardiographic speckle-tracking technique enables layer-specific analysis of myocardial deformation. However, the lack of sufficiently validated reference values for myocardial strain is a challenge that needs to be resolved. Furthermore, there are several issues that can impede an accurate strain measurement, including poor echocardiographic image quality and rotation of the heart.13 However, echocardiographic strain can provide patients with a non-invasive and robust assessment of myocardial deformation for early detection of cardiotoxicity during or following chemotherapy.
None.