Essential thrombocythemia (ET) is one of the severe clonal hematologic stem cells disorders belonging to myeloproliferative syndrome.1
ET has been shown to be associated with arterial thrombosis,1
and the discovery of the
V617FJAK2
mutation enabled elucidation of the prothrombotic state of this hematological malignancy.1
Transcutaneous oxygen pressure (tcpO2) measurement at rest is mainly used to assess critical limb ischemia. This technique is also used during exercise (exercise-tcpO2). Exercise-tcpO2 is a promising technique for the diagnosis of lower limb tissue ischemia during walking. We have already shown its usefulness in the diagnosis and monitoring of peripheral arterial disease (PAD) and exercise claudication.2
The aim of this study was therefore to determine whether exercise-tcpO2 could be used to identify exercise ischemia induced by non-atheromatous PAD in young adults, such as ET.
A 47-year-old man, former smoker, with a history of arterial hypertension and transient ischemic attack was referred for investigation of severe left foot claudication and Raynaud’s phenomenon of the toes in December 2015. He was on medical treatment for secondary cardiovascular prevention.
Feet examination at rest was normal, but after exercise pallor and coldness and Raynaud’s phenomenon were noted on the left side (Figure, Left panel). Ankle brachial index (ABI) was measured as recommended by current guidelines. Doppler ultrasonography (US) was performed, followed by exercise-tcpO2 to assess the vascular origin of exercise-induced pain.2
A reference probe (chest probe) was placed between the scapulae to measure systemic changes in tcpO2 during exercise.2
One probe was positioned on each buttock and one probe on each calf. Once the probes were in position, the patient then waited for 10 min in the standing position, in order to stabilize the probes to obtain baseline values. Finally, one probe was positioned on the left foot. During exercise-tcpO2, chest tcpO2 changes are subtracted from limb tcpO2 changes and expressed as decrease from rest of oxygen pressure (DROP; mmHg). DROP is zero at rest and returns to zero after recovery. Minimum DROP (DROPmin) is the lowest observed. Calculations are automatically performed during the test using dedicated software (OxyMonitor®). The treadmill test uses a constant load procedure (10% slope and 3.2 km/h speed) up to 20 min (1,800 s). The maximum walking time (MWT) and the maximum walking distance (MWD) were measured.
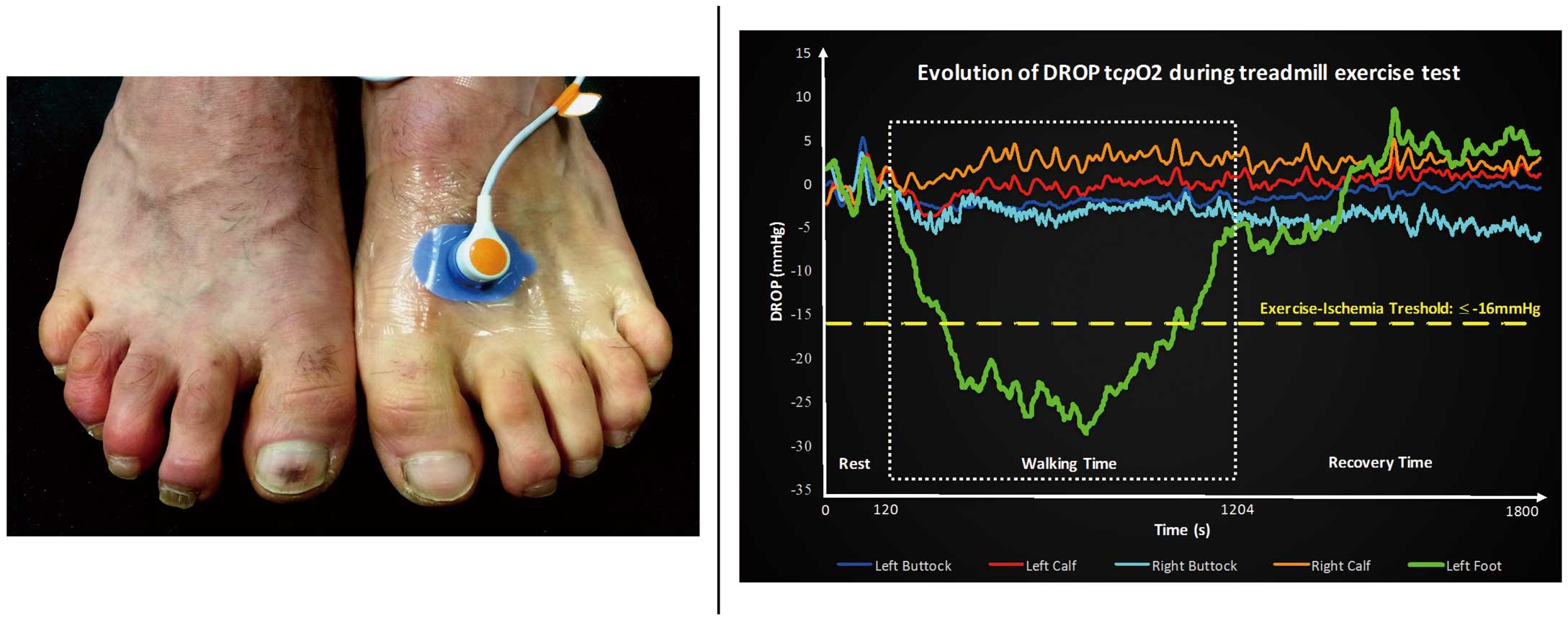
ABI was 1.13 on the right side and 0.97 on the left side. Lower limb US was normal. During the test, DROPmin was −33 mmHg in the left foot (Figure, Right panel). In the right and left calves, DROPmin was always above −16 mmHg; in the right and left buttocks it was always above −15 mmHg.2
The MWT was 1,204 s, corresponding to an MWD of 1,053 m, and walking was stopped at the end of the treadmill test. Exercise-tcpO2 confirmed exercise-induced left foot ischemia. Relevant diagnostic procedures were performed following the diagnosis, including multiple blood tests, which indicated thrombocythemia (platelet count, 850×109/L) without iron deficiency or inflammatory syndrome. Differential diagnoses such as connective disease, vasculitis, or primary/secondary coagulopathy were negative.
V617FJAK2
mutation was positive and the diagnosis of ET was retained. Coronarography showed long chronic occlusion of the right middle coronary artery. Cytoreductive treatment with hydroxyurea (Hydrea®; 500 mg b.i.d.) was introduced and the last platelet count after 3 months of treatment was 457×109/L. No thrombotic event has occurred since the initiation of treatment.
ET is a hematologic disorder characterized by a markedly elevated platelet count caused by excessive megakaryocyte proliferation with an annual incidence rate in the USA of approximately 1.5/100,000 persons.3
The activating
V617FJAK2
mutation can be a strong predictor for thromboembolic events in ET patients.3
In ET patients, the main cause of morbi-mortality is associated with its prothrombotic state, including vascular thrombosis. Thrombotic complications are present at diagnosis in approximately 9–22% of patients.3
Claudication is a common clinical expression of PAD, and atherosclerosis is the main etiology. Smoking is one of the most potent risk factors for PAD,4
and it is associated with an increased rate of mutagenesis and cancer.5
Occurrence of
V617FJAK2
mutation is increased (3.1%) in PAD patients compared with healthy subjects.6
Exercise-tcpO2 can identify a vascular origin of walking-induced pain especially in the case of proximal claudication, but this technique does not allow prediction of the etiology of exercise ischemia. In the present case, US did not show any arterial lesion or pathological Doppler waveform.7
Therefore, computed tomography angiography was not performed because revascularization was not considered in the present case. This is in agreement with PAD guidelines.8
While US and the other non-invasive vascular imaging techniques did not indicate macrovascular involvement due to very distal and microcirculatory lesions, exercise-tcpO2 showed the functional impact of this ischemia. We have previously shown that exercise-tcpO2 using a distal DROPmin ≤−16 mmHg is accurate to diagnose arterial stenosis, especially stenosis ≥60% in the lower limbs.
In conclusion, in this case of suspected vascular impairment during exercise and when non-invasive vascular imaging is normal, exercise-tcpO2 can be used to confirm or exclude the vascular origin of symptomatology.
Acknowledgment
Written consent for publication was obtained from the patient.
Disclosures
The authors declare no conflict of interest.
Author contributions
L.O. contributed to literature search, data collection, data analysis, data interpretation, and writing of the report. O.S. contributed to literature search, data analysis, data interpretation, and revising of the intellectual content. G.M. and V.J. carried out patient management, and contributed to literature search, data collection, data analysis, data interpretation, and revising of the intellectual content. All authors read approved the final version of the manuscript.
References
- 1.
Sivakumaran Y, Freeman A. Refractory arterial insufficiency associated with Janus kinase 2 positive essential thrombocythaemia. Ann Vasc Surg 2017; 38: 317.e13–e16.
- 2.
Koch C, Chauve E, Chaudru S, Le Faucheur A, Jaquinandi V, Mahé G. Exercise transcutaneous oxygen pressure measurement has good sensitivity and specificity to detect lower extremity arterial stenosis assessed by computed tomography angiography. Medicine (Baltimore) 2016; 95: e4522.
- 3.
Tefferi A, Barbui T. Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management: TEFFERI and BARBUI. Am J Hematol 2017; 92: 94–108.
- 4.
Lu L, Mackay DF, Pell JP. Meta-analysis of the association between cigarette smoking and peripheral arterial disease. Heart 2014; 100: 414–423.
- 5.
Pfeifer GP, Denissenko MF, Olivier M, Tretyakova N, Hecht SS, Hainaut P. Tobacco smoke carcinogens, DNA damage and p53 mutations in smoking-associated cancers. Oncogene 2002; 21: 7435–7451.
- 6.
Muendlein A, Kinz E, Gasser K, Leiherer A, Rein P, Saely CH, et al. Occurrence of the JAK2 V617F mutation in patients with peripheral arterial disease. Am J Hematol 2015; 90: E17–E21.
- 7.
Mahé G, Boulon C, Desormais I, Lacroix P, Bressollette L, Guilmot J-L, et al. Statement for Doppler waveforms analysis. Vasa, doi:10.1024/0301-1526/a000638.
- 8.
Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017; 69: e71–e126.
