Images in Cardiovascular Medicine
Neoatherosclerosis With Napkin Ring Calcification
2018 Volume 82 Issue 8 Pages 2208-2209

Details
2018 Volume 82 Issue 8 Pages 2208-2209
An 84-year-old woman on hemodialysis was admitted due to effort angina. She had a history of paclitaxel-eluting stent (PES) implantation for a diffuse stenotic lesion with a tiny calcification at the proximal left anterior descending artery 6 years earlier (Figure 1). Angiography showed a restenosis at the distal edge of the PES (Figure 2A). On optical coherence tomography a significant luminal narrowing with circumferential and thick calcium formation was noted around the stent edge (Figure 2B,C). Given that balloon angioplasty failed to dilate the lesion, rotational atherectomy was necessary. An everolimus-eluting stent (2.5–38 mm) was then successfully implanted to cover both the restenosis lesion and a subsequent diffuse lesion at the distal end of the stent.
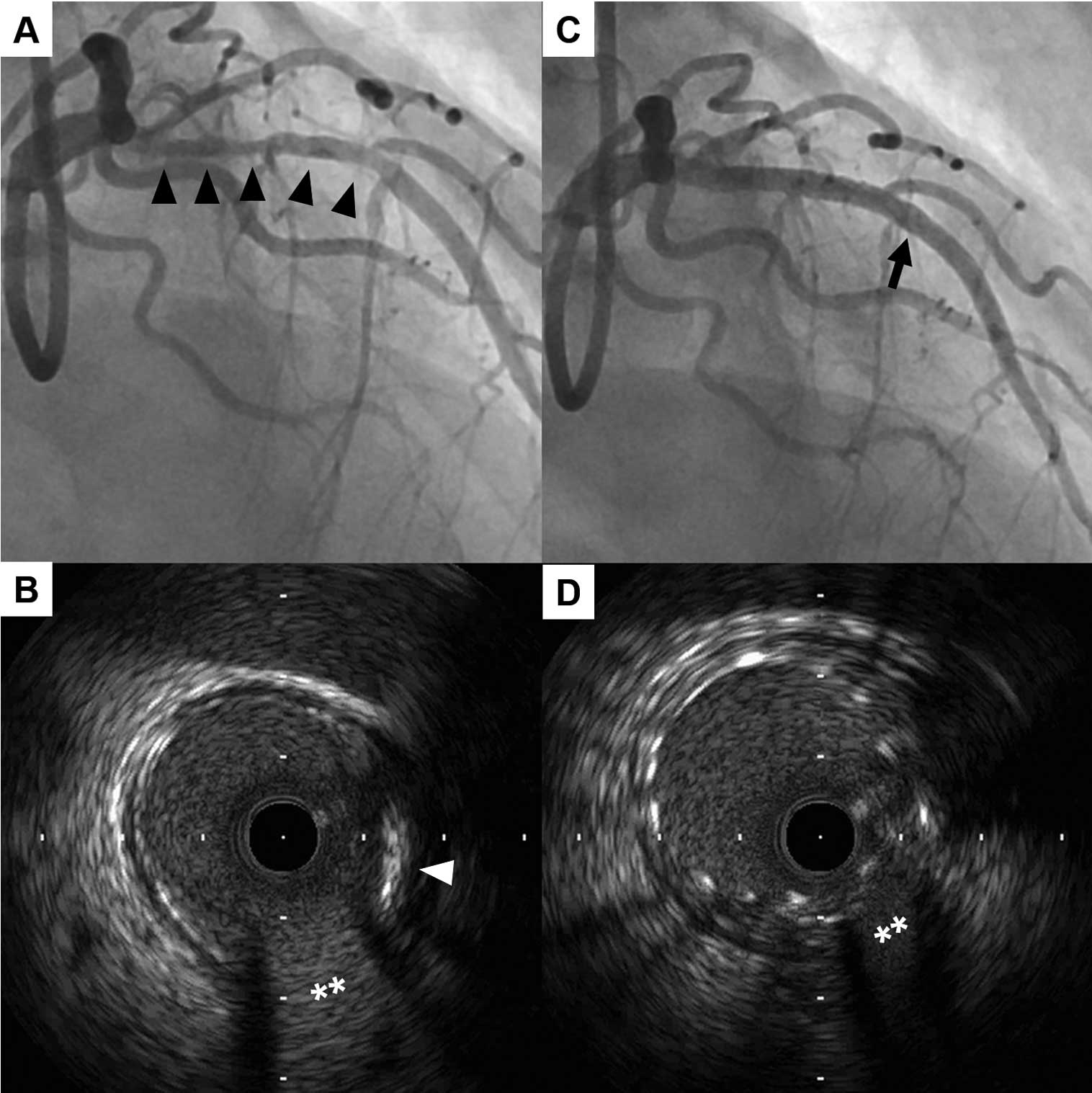
(A,C) Angiography and (B,D) intravascular ultrasound (IVUS) at the stent implantation 6 years earlier. (A) Angiogram showing a diffuse stenotic lesion (arrowheads) at the mid-left anterior descending artery. (B) IVUS showing a tiny calcification (arrowhead) without significant plaque deposition at the distal end of the lesion. (**) Septal branch. (C) Angiogram showing successful paclitaxel-eluting stent implantation. Arrow, distal edge of the stent. (D) IVUS showing the distal edge of the stent. The final minimum stent area was 6.15 mm2.

(A,E) Angiography and (B–D) optical coherence tomography (OCT) at the present revascularization. (A) angiogram showing tight restenosis around the distal edge of a paclitaxel-eluting stent (arrow). (B–D) OCT showing (B,C) circumferential and thick calcium formation (*) with significant luminal narrowing (arrowheads, stent struts; **, septal branch); and (D) the expanded lumen with a crack (arrow) by the ablation of circumferential calcification (*) using rotational atherectomy (arrowheads, stent struts). (E) Angiography showing successful revascularization with an everolimus-eluting stent. The final minimum stent area was 4.47 mm2.
Neoatherosclerosis has been reported as a cause of stent failure in the chronic phase.1 Herein, we report a case of neoatherosclerosis with extremely severe calcification requiring rotational atherectomy. Intriguingly, the neointimal tissue was completely occupied by thick and circumferential calcification although there had been a tiny calcification at the corresponding site before stenting. A higher prevalence of neointimal calcification has been noted in hemodialysis patients,2 and greater prevalence of neoatherosclerosis in first-generation drug-eluting stents (DES) than in bare metal stents.3 Thus, the combination of hemodialysis and first-generation DES may have contributed to the development of severe calcification within the neointimal tissue as an underlying mechanism, although the additional specific contributor in the present case is still unclear. Precise lesion evaluation and appropriate device selection using intracoronary imaging is also of clinical importance for the treatment of in-stent neoatherosclerotic lesions.
The authors declare no conflicts of interest.