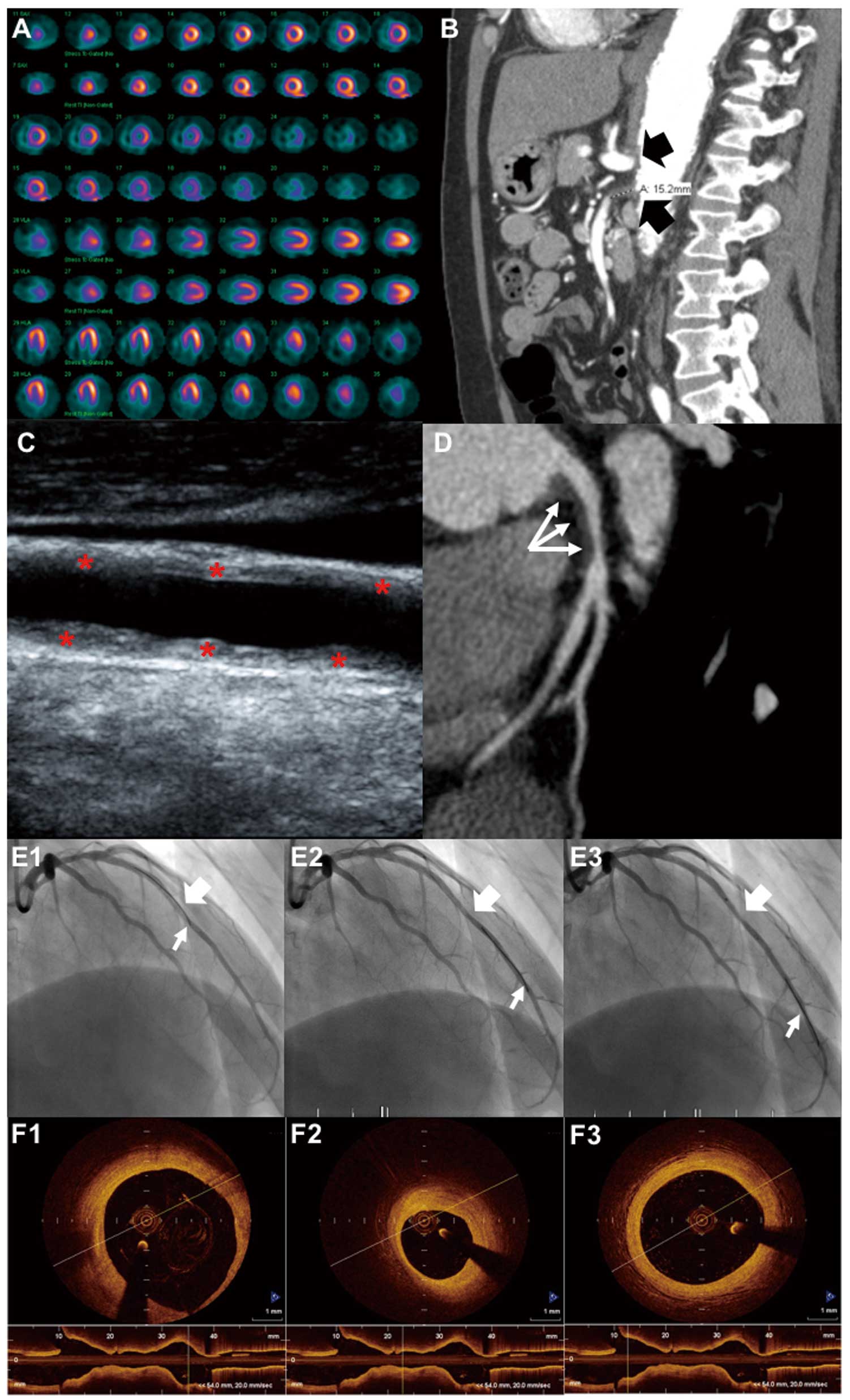
A 39-year-old man with chronic myelogenous leukemia treated with imatinib presented with recurrent chest pain. On myocardial perfusion stress test, decreased radiotracer uptake was noted in the apico-septal segment (Figure A). Ischemic heart disease, imatinib-induced cardiotoxicity, and vasculitis were considered. Abdominal computed tomography angiography (CTA) showed narrowing of the proximal celiac artery with post-stenotic dilatation and thrombosed proximal superior mesenteric artery with near immediate reconstitution after the ostium (Figure B). Carotid Doppler showed long echogenic plaques involving bilateral common carotid segments (Figure C). Coronary CTA showed a significant non-calcified plaque affecting the proximal left anterior descending (LAD) artery (Figure D). These findings suggested medium- and large-vessel vasculitis, most likely Takayasu arteritis (TA). Coronary angiography showed an intermediate proximal LAD lesion (Figure E1) that was further assessed on fractional flow reserve (FFR;
Figure E1–E3) with no requirement for stenting. Optical coherence tomography (OCT) indicated characteristic diffuse disease, with a superimposed focal stenosis in the proximal LAD (Figure F1) and high tissue backscatter at the intermediate lesion level (Figure F2) and distally (Figure F3), confirming the diagnosis of TA. The patient was started on prednisone and methotrexate with symptom relief.
Histologic diagnosis of TA is usually impractical because of the location of the arteries involved, which is unsuitable for biopsy. A multimodality approach including novel diagnostic techniques, such as FFR and OCT, adds value to the diagnosis and management of complex patients with cancer, coronary artery disease, and autoimmune disorders (Table S1).
Funding
No funding sources were allocated to this study.
Disclosures
The authors declare no conflicts of interest.
Supplementary Files
Supplementary File 1
Table S1.
Conditions associated with coronary lesions: multimodality findings
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-18-0445
