Abstract
Background:
Monocytes in human peripheral blood are heterogeneous and can be divided into 2 groups, inflammatory and pro-inflammatory, according to the differential expression of CD14 and CD16. Pro-inflammatory monocytes (CD14+CD16+) seem to contribute to the development of coronary artery disease. This study aimed to investigate the involvement of specific human peripheral monocyte subsets in the development of future coronary events.
Methods and Results:
We enrolled 271 patients who were suspected to have either stable angina pectoris or silent myocardial ischemia and underwent coronary angiography (CAG). Two monocyte subsets (CD14+CD16−
and CD14+CD16+) were measured by flow cytometry. Patients who did not undergo coronary artery revascularization at initial CAG were followed as the medical therapy group, which included 136 patients among whom 15 had future coronary events. The frequency of CD14+CD16+
monocytes was significantly higher in patients who had future coronary events than in those who did not (P<0.01). Furthermore, the frequencies of CD14+CD16+
monocyte were not significantly different between patients who had future coronary events and those who underwent coronary revascularization at initial CAG (P<0.33). Multivariate analysis revealed that the frequency of CD14+CD16+
monocytes was an independent predictor for future coronary events (P<0.01).
Conclusions:
An increase in the abundance of human peripheral pro-inflammatory monocytes is related to the development of future coronary events.
Monocytes in human peripheral blood are heterogeneous and can be divided into 2 groups, inflammatory and pro-inflammatory, according to the differential expression of CD14 and CD16.1–3
CD14+CD16−
monocytes, which are considered as inflammatory, express C-C motif chemokine receptor 2, whereas CD14+CD16+
monocytes, which are considered as pro-inflammatory, express C-X3-C motif chemokine receptor 1 (CX3CR1). In terms of the relationship between human monocyte subsets and ischemic heart disease, we previously revealed that an increase in CD14+CD16+
monocytes is associated with the prevalence and severity of stable angina pectoris (SAP).4,5
In addition, the pro-inflammatory subset of monocytes contributes to the pathogenesis of acute coronary syndrome by upregulating the expression of toll-like receptor 4 and/or P-selectin glycoprotein ligand-1.6,7
Thus, pro-inflammatory monocytes are deemed to be diversely correlated with the development of coronary artery disease (CAD).
Pro-inflammatory monocytes are further divided into 2 groups: the patrolling and intermediate monocyte subsets.8,9
Recent several studies revealed that an increase in the human peripheral pro-inflammatory monocyte subset, especially the intermediate monocyte subset, can predict the prevalence of future cerebrocardiovascular events.10–13
Conversely, another report demonstrated that inflammatory monocytes are a predictor for future cardiovascular events.14
Therefore, it is still unclear which human monocyte subset can truly predict cerebrocardiovascular events. Moreover, the endpoints of past studies have involved several atherosclerotic diseases, including cardiac events, cerebral infarction, and peripheral artery disease, and were thus not limited to coronary events.
In this study, we investigated whether human peripheral monocytes are related to the development of future coronary events. Furthermore, we focused on high-risk populations who were suspected to have stable CAD, but were assessed otherwise based on invasive coronary angiography (CAG) and hemodynamic testing.
Methods
Patient Population
We enrolled patients who were suspected to have SAP or silent myocardial ischemia (SMI). Diagnosis of SAP and SMI were done through combinations of assessing for the presence of effort chest pain, electrocardiography, echocardiography, computed tomography angiography and/or cardiac scintigraphy. Exclusion criteria were artificial dialysis, collagen disease, valvular heart disease and malignant disease. The study protocol was approved by the Institutional Ethics Committee of Wakayama Medical University (535) and written informed consent was given by either the patient or a family member.
Clinical Parameters
Clinical parameters assessed included age, sex, medications, and coronary risk factors, which included hypertension (blood pressure ≥140/90 mmHg and/or a history of antihypertensive medication), diabetes mellitus (fasting plasma glucose >126 mg/dL, casual plasma glucose ≥200 mg/dL, or a diabetic pattern in 75-g oral glucose tolerance test), hyperlipidemia (serum total cholesterol >220 mg/dL), smoking status, and family history.
Cytometric Analysis
For cytometric analysis, monoclonal antibodies against CD14 (fluorescein isothiocyanate [FITC]-conjugated, clone M5E2; BD Biosciences) and CD16 (phycoerythrin [PE]-Cy5-conjugated, clone 3G8; BD Biosciences) were used as described previously.4–7
Matched-isotype antibodies (FITC-conjugated mouse IgG2aκ isotype, clone G155-178, and PE-Cy5 mouse IgG1κ isotype, clone MOPC-21; BD Biosciences) were used as negative controls. A total of 100 μL of blood was incubated for 15 min at room temperature in the dark. For erythrocyte lysis and leukocyte fixation, 1 mL of lysis solution was added (BD FACS Lyse, Lysing Solution; Becton Dickinson, Germany).
Cytometric analysis was performed using a flow cytometer (FACS Aria, Becton Dickinson) as described previously.7
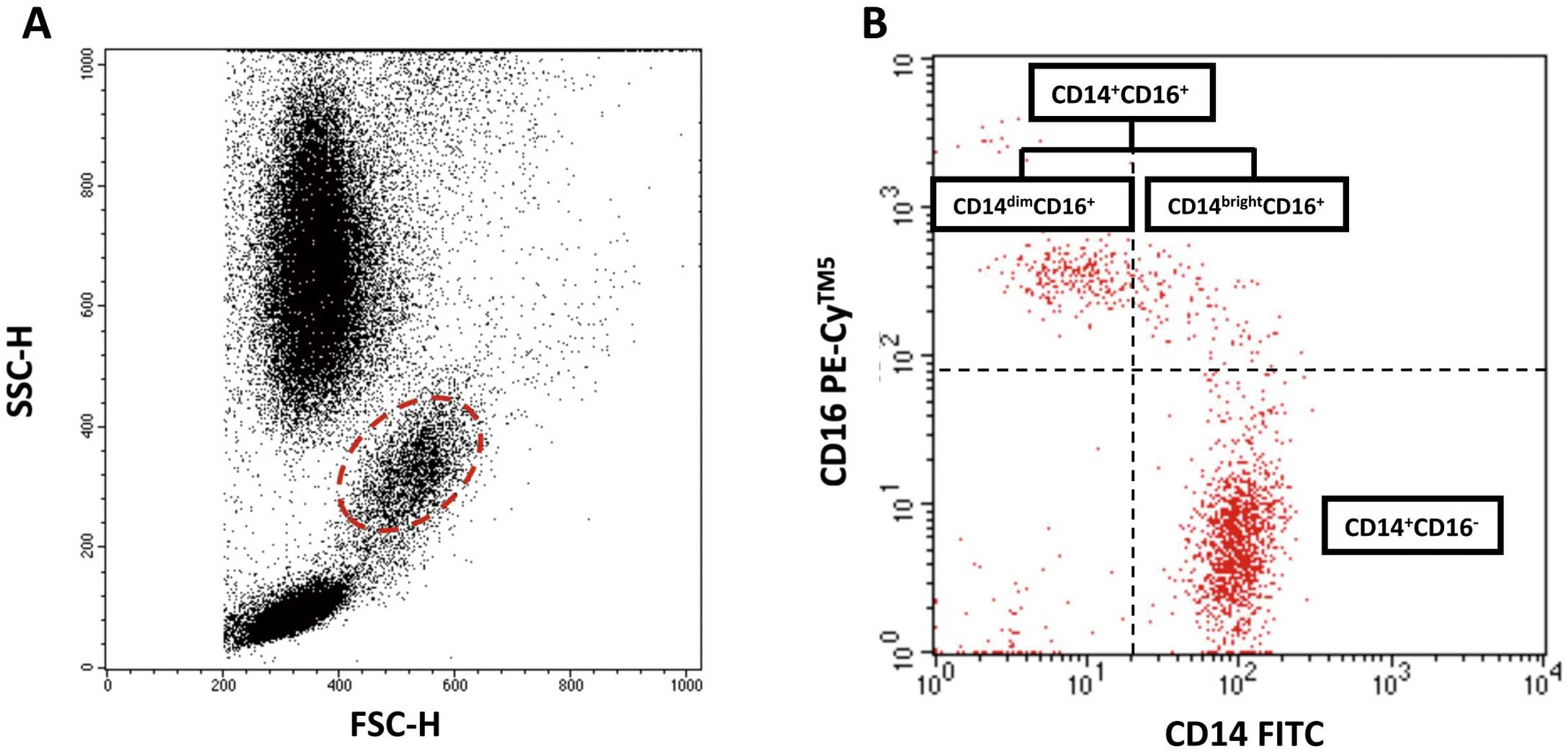
Monocytes were first gated in a forward scatter/sideward scatter (FSC/SSC) dot plot, and 2-color fluorescence was then measured within the monocyte gate. CD14+CD16−
cells were defined as monocytes expressing CD14 but not CD16 (lower right quadrant). CD14+CD16+
cells were defined as monocytes expressing CD16 and either a high level of CD14 (upper right quadrant; CD14brightCD16+) or a low level of CD14 (upper left quadrant; CD14dimCD16+). Thus, CD14brightCD16+
and CD14dimCD16+
were not analyzed separately (Figure 1).
Blood Sampling and Analysis
Peripheral blood samples were collected from all subjects upon admission in preparation for planned percutaneous coronary intervention (PCI). Plasma samples were collected in ethylenediaminetetraacetic acid anticoagulant tubes and stored at −80℃ until assayed. Plasma levels of soluble fractalkine (s-FKN), tumor necrosis factor α (TNF-α), and interleukin 10 (IL-10) were analyzed using a commercially available kit (Quantiline ELISA; R&D systems).
CAG
All patients underwent CAG before the subsequent therapeutic strategy was decided. All lesions with more than moderate stenosis in a major coronary artery were handled with evidence of ischemia according to a physiological test, including the measurement of fractional flow reserve (FFR) and/or cardiac scintigraphy.15,16
Prognostic Analysis
Patients who met the following criteria at initial CAG were followed as the medical therapy group: (1) did not undergo coronary artery revascularization by PCI or coronary artery bypass graft (CABG), and (2) did not have a hemodynamically significant ischemic lesion in the main branch of coronary arteries proofed by measuring FFR or on cardiac scintigraphy. Endpoint was new onset or recurrence of acute myocardial infarction (AMI), unstable angina (UAP), SAP, and/or coronary revascularization (PCI and CABG) for any cause.
Statistical Analysis
Statistical analysis was performed using JMP pro version 13.0 for Macintosh (SAS Institute, Cary, NC, USA). Results are expressed as mean±standard deviation (SD) or median (interquartile range). Qualitative data are presented as number (%). When more than 2 groups were compared, the Kruskal-Wallis test was used for continuous variables. Pearson’s chi-square test was applied for categorical variables. Receiver-operating characteristic curve analysis was used to determine the best cutoff value for CD14+CD16+
monocytes for future coronary event. Kaplan-Meier log-ranked survival probability analysis was applied for the different monocyte groups. Cox proportional hazards regression analysis was applied to determine independent predictors of future coronary events. A P-value <0.05 was considered statistically significant.
Results
Patients’ Enrollment
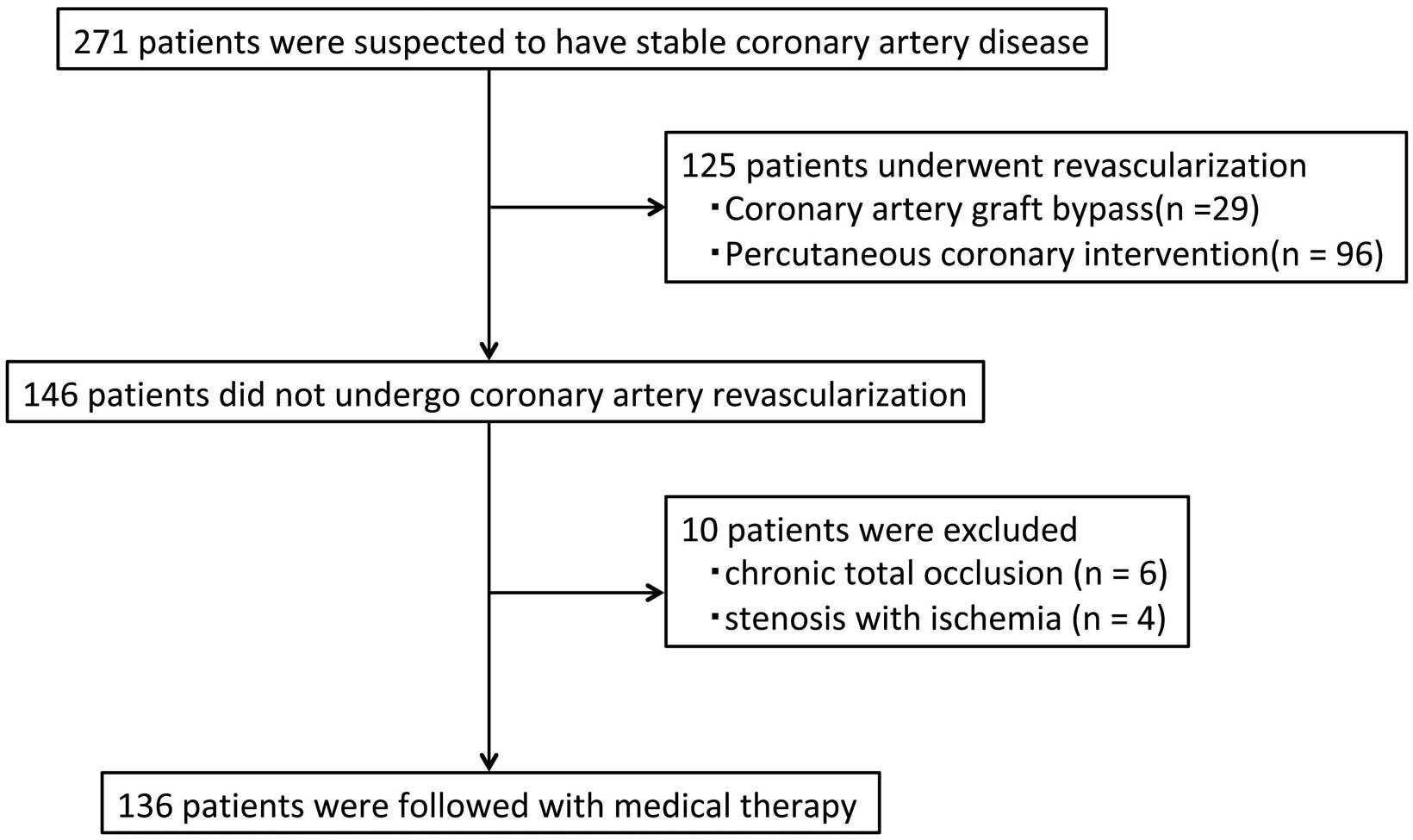
The study population is summarized in
Figure 2. A total of 271 patients were enrolled. In 125 patients, coronary artery revascularization (29 CABG and 96 PCI) was selected at initial cardiac catheterization. Among the patients who did not undergo coronary revascularization, 10 were excluded from the medical therapy group because of significant coronary artery stenosis and/or total occlusion in the main branch of the coronary artery. Therefore, a total of 136 patients were followed up with medical therapy.
Human Peripheral Monocyte Subsets and Endpoint
In the medical therapy group, the median and interquartile follow-up period was 4.7 [2.8–6.3] years. Overall, 15 patients had coronary events (3 AMI, 3 UAP, 9 SAP), and 3 CABG and 12 PCI were done. The baseline characteristics, laboratory blood test results and flow cytometry data of each group are described in
Table 1
and
Figure 3. The serum levels of total cholesterol, low-density lipoprotein and hemoglobin A1c were higher in the coronary revascularization group than in the medical group without coronary events. There were no significant differences between the medical groups with and without coronary events except for the frequency of CD14+CD16+
monocytes. The frequency of CD14+CD16+
monocytes was significantly higher in patients who had future coronary events than in those who did not (21.0 [16.3–24.0]% vs. 15.1 [10.4–18.2]%, P<0.01). Furthermore, the frequencies of CD14+CD16+
monocytes were not significantly different between patients who had future coronary events and those who underwent coronary revascularization at initial CAG (21.1 [16.3–24.0]% vs. 19.4 [13.9–23.6]%, P<0.33). In the Cox proportional hazards regression analysis, the frequency of CD14+CD16+
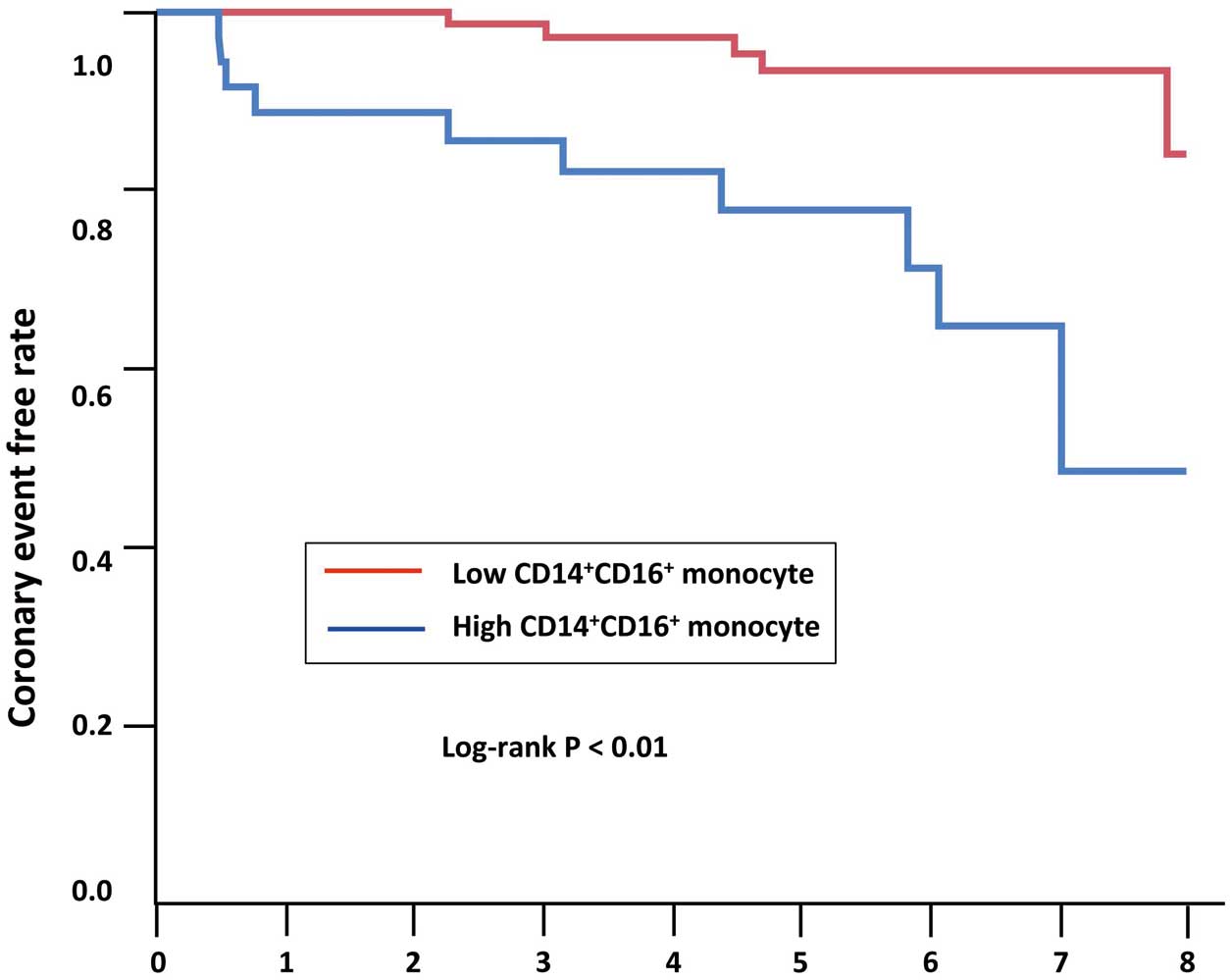
monocytes was determined as a significant prognostic factor (hazard ratio 1.14, 95% confidence interval 1.06–1.23, P<0.01) (Table 2). From the receiver-operating curve, the best cutoff value of the frequency of CD14+CD16+
monocytes to predict future coronary events was 19.2%.
Figure 4
shows the Kaplan-Meier curve for coronary events between the high (≥19.2%) and low (<19.2%) frequency of CD14+CD16+
monocyte groups. Coronary event-free periods were shorter in the patients with high frequency of CD14+CD16+
monocytes (P<0.01).
Table 1.
Patients’ Characteristics and Blood Test Data
| |
Medical therapy following
coronary event (−) |
Medical therapy following
coronary event (+) |
Coronary revascularization
CABG/PCI |
P value |
| Patient, n |
121 |
15 |
125 |
|
| Age (years) |
69±10 |
65±12 |
69±9 |
0.70 |
| Men |
90 (74) |
12 (80) |
102 (82) |
0.39 |
| Coronary risk factors |
| Hypertension |
87 (72) |
12 (80) |
95 (76) |
0.67 |
| Diabetes mellitus |
46 (38) |
8 (53) |
58 (46) |
0.29 |
| Dyslipidemia |
76 (63) |
10 (67) |
80 (64) |
0.95 |
| Family history |
15 (12) |
1 (7) |
15 (12) |
0.81 |
| Smoking |
49 (41) |
7 (47) |
69 (55) |
0.07 |
| Medications |
| Aspirin |
97 (80) |
14 (93) |
112 (90) |
<0.01 |
| Dual antiplatelet therapy |
38 (31) |
5 (36) |
76 (61) |
<0.01 |
| Anticoagulant |
8 (7) |
2 (13) |
8 (6) |
0.62 |
| Calcium antagonist |
31 (26) |
6 (40) |
48 (38) |
0.08 |
| ACEI/ARB |
79 (65) |
10 (67) |
60 (48) |
0.02 |
| β-blocker |
49 (41) |
7 (47) |
40 (32) |
0.30 |
| Statin |
62 (51) |
7 (47) |
65 (52) |
0.19 |
| Antihyperglycemic agent |
34 (28) |
3 (20) |
44 (35) |
0.29 |
| Total cholesterol, mg/dL |
179±34 |
175±49 |
189±36 |
0.04 |
| Triglycerides, mg/dL |
131±78 |
152±155 |
148±96 |
0.29 |
| High-density lipoprotein, mg/dL |
48±13 |
41±10 |
44±11 |
0.08 |
| Low-density lipoprotein, mg/dL |
101±30 |
106±41 |
112±32 |
0.02 |
| Hemoglobin A1c, % |
5.8±1.1 |
6.4±1.4 |
6.1±1.2 |
0.03 |
Data are mean±SD or n (%). ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention.
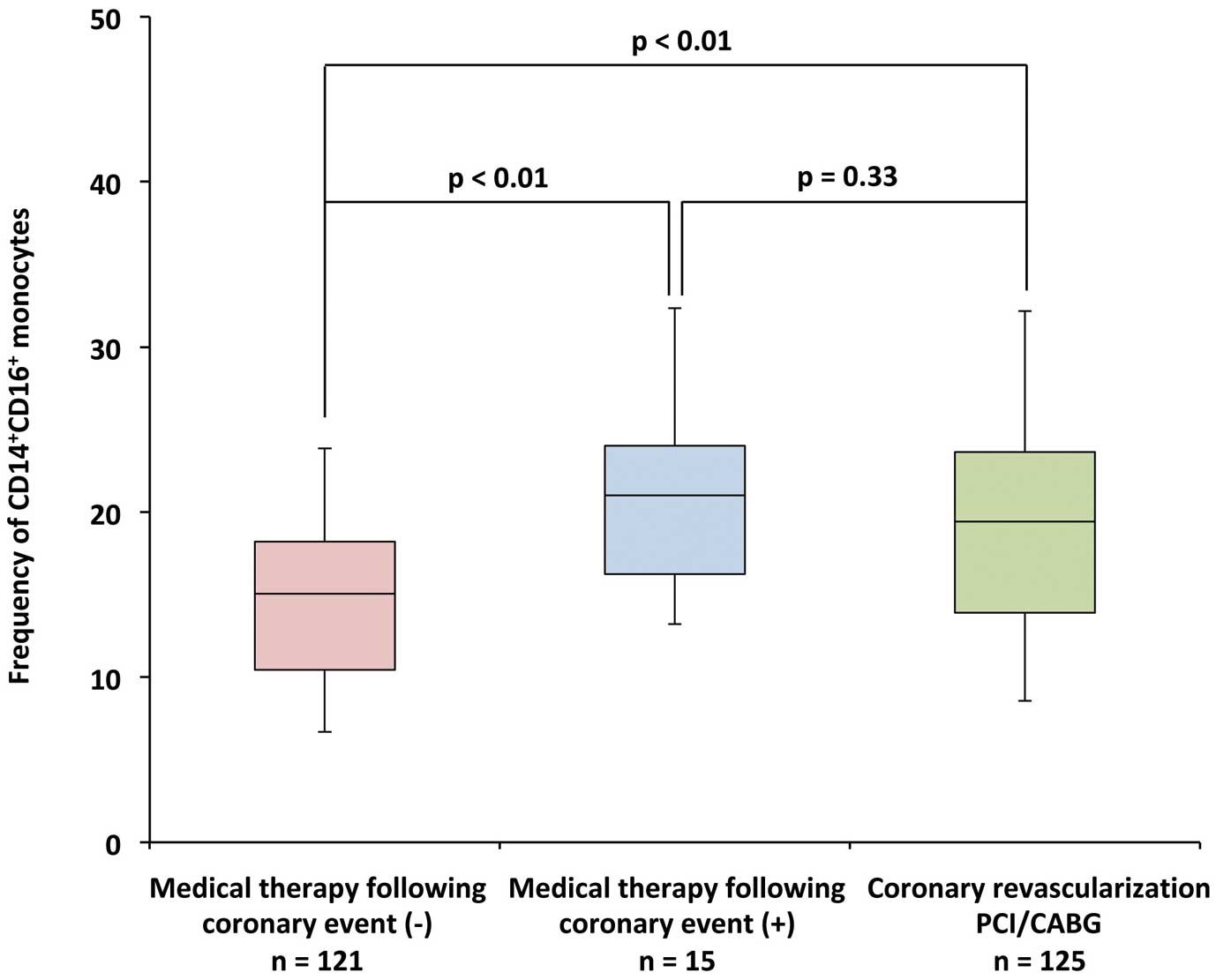
Table 2.
Multivariate Analysis
| |
HR (95% CI) |
P value |
| Hypertension |
2.71 (0.67–11.01) |
0.13 |
| Diabetes mellitus |
2.02 (0.68–6.05) |
0.21 |
| Dyslipidemia |
0.94 (0.29–3.06) |
0.92 |
| Family history |
0.33 (0.04–2.60) |
0.22 |
| Smoking |
1.03 (0.36–2.99) |
0.95 |
| C-reactive protein, mg/dL |
1.76 (0.81–3.82) |
0.23 |
| CD14+CD16+ monocytes, % |
1.14 (1.06–1.23) |
<0.01 |
CI, confidence interval; HR, hazard ratio.
Comparisons of inflammatory marker data among the 3 groups are shown in
Table 3. The plasma levels of TNF-α were significantly higher in the medical group with coronary events and the coronary revascularization group than in the medical group without coronary events (P<0.01). Other inflammatory markers were not significantly different among the 3 groups.
Table 3.
Inflammatory Marker Data
| |
Medical therapy following
coronary event (−)
(n=121) |
Medical therapy following
coronary event (+)
(n=15) |
Coronary revascularization
CABG/PCI
(n=125) |
P value |
| White blood cell, cells/μL |
6,200 [4,920–7,550] |
6,100 [5,455–6,820] |
6,120 [5,028–7,195] |
0.97 |
| C-reactive protein, mg/dL |
0.10 [0.04–0.16] |
0.13 [0.05–0.28] |
0.11 [0.05–0.29] |
0.27 |
| Tumor necrosis factor α, pg/mL |
1.56 [1.25–1.99] |
1.92 [1.61–2.25] |
1.93 [1.56–2.34] |
<0.01 |
| Soluble fractalkine, ng/mL |
0.65 [0.52–0.92] |
0.79 [0.61–0.90] |
0.76 [0.60–0.91] |
0.08 |
| Interleukin 10, pg/mL |
42.6 [24.0–60.7] |
32.4 [27.5–50.7] |
41.7 [30.6–57.4] |
0.37 |
Data are median [interquartile range]. CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention.
Discussion
In the present study, the frequency of CD14+CD16+
monocytes was higher in patients with future coronary events than in those who did not. The role of each monocyte subset in murine atherosclerosis has been steadily elucidated, but many aspects of the association of human monocyte subsets in the prognosis of atherosclerosis are unknown. It is considered that circulating monocytes invade and accumulate in the endothelium of arterial walls. These monocytes subsequently differentiate into foam cells and contribute to plaque formation.17
Human CD14+CD16+
monocytes are supposed to play a key role in this process and contribute to vulnerable plaque formation.18
Many investigators have reported the elevation of CD14+CD16+
monocytes in patients CAD and argued those relationships. To date, there are several reports linking the human peripheral monocyte subset and the development of future cardiovascular events.11–14
Although the results have not been consistent, it is generally thought that specific monocyte subsets are likely to be associated with the development of future cardiovascular events, including stroke and peripheral artery disease. However, there has been little evidence regarding the relationship between monocyte subsets and peripheral artery disease, particularly stroke.19,20
Because there have been no reports regarding the association between human monocyte subsets and future coronary disease events, we focused on the prognosis of CAD in this study. In addition, we included patients who were strongly suspected to have CAD, and most of them indeed had atherosclerotic lesions; however, no ischemia was observed in the main coronary arteries as determined by physiological assessment. Therefore, our study population consisted of relatively vulnerable patients. As a result, CD14+CD16+
monocytes were identified as an independent predictor for future coronary events. More interestingly, the frequency of CD14+CD16+
monocytes in patients who deferred coronary artery revascularization at initial angiography was not significantly different to patients who were diagnosed with CAD and underwent coronary artery revascularization. This indicates that vulnerable patients have a high probability of undergoing coronary revascularization even if they defer invasive treatment. In addition, we previously reported that statins have the potential to stabilize coronary artery plaques by reducing CD14+CD16+
monocytes.21
Although elevation of C-reactive protein (CRP) is considered a strong predictor of cardiovascular events, we found no relation between CRP and future coronary artery events in this study.22
These results highlight the potential of monitoring CD14+CD16+
monocytes for prognosis, as well as for providing risk stratification of vulnerable patients so that they can consider undergoing aggressive and optimal therapeutic interventions.
In our results the plasma levels of TNF-α were elevated in patients who had future coronary events. TNF-α and FKN are cytokines that interact with CD14+CD16+
monocytes in the development of atherosclerosis.23–25
Human CD14+CD16+
monocytes express high levels of CX3CR1, and the interaction of CX3CR1 and FKN mediates the migration of circulating monocytes into the vessel wall. TNF-α also facilitates the adhesion of circulating monocytes onto the endothelium. In addition, CD14+CD16+
monocytes can further produce higher levels of TNF-α.26
FKN expression is normally induced by pro-inflammatory cytokines such as TNF-α. The upregulation of the abundance of human CD14+CD16+
monocytes might occur upstream of the interaction of monocytes and CX3CR1/FKN. Although lower levels of IL-10 have been associated with CAD, no significant difference was observed in our small study population.27,28
Study Limitations
The small sample size may make the results susceptible to the effects of biological heterogeneity. We had information about the administration of medications at initial CAG. We only investigated the differences in a limited number of cytokines between the 2 monocyte subsets. Therefore, our results might not be completely informative about the mechanistic link between monocytes and CAD. There were no data about the total number of monocytes in this study.
In conclusion, an increase in the abundance of human peripheral monocytes, especially CD14+CD16+
monocytes, was associated with the development of future coronary events. Our results support the hypothesis that CD14+CD16+
monocytes contribute to the development of coronary artery atherosclerosis.
Sources of Funding
This work was supported in part by JSPS KAKENHI Grant Number 20590835 (Grant-in-Aid for Young Scientists B).
Disclosures
There are no conflicts of interest in this study.
References
- 1.
Gerrity RG. The role of the monocyte in atherogenesis. II: Migration of foam cells from atherosclerotic lesions. Am J Pathol 1981; 103: 191–200.
- 2.
Geissmann F, Jung S, Littman DR. Blood monocytes consist of two principal subsets with distinct migratory properties. Immunity 2003; 19: 71–82.
- 3.
Gordon S, Taylor PR. Monocyte and macrophage heterogeneity. Nat Rev Immunol 2005; 5: 953–964.
- 4.
Kashiwagi M, Imanishi T, Tsujioka H, Ikejima H, Kuroi A, Ozaki Y, et al. Association of monocyte subsets with vulnerability characteristics of coronary plaques as assessed by 64-slice multidetector computed tomography in patients with stable angina pectoris. Atherosclerosis 2010; 212: 171–176.
- 5.
Ozaki Y, Imanishi T, Taruya A, Aoki H, Masuno T, Shiono Y, et al. Circulating CD14+CD16+ monocyte subsets as biomarkers of the severity of coronary artery disease in patients with stable angina pectoris. Circ J 2012; 76: 2412–2418.
- 6.
Ozaki Y, Imanishi T, Teraguchi I, Nishiguchi T, Orii M, Shiono Y, et al. Association between P-selectin glycoprotein ligand-1 and pathogenesis in acute coronary syndrome assessed by optical coherence tomography. Atherosclerosis 2014; 233: 697–703.
- 7.
Kashiwagi M, Imanishi T, Ozaki Y, Satogami K, Masuno T, Wada T, et al. Differential expression of Toll-like receptor 4 and human monocyte subsets in acute myocardial infarction. Atherosclerosis 2012; 221: 249–253.
- 8.
Ghattas A, Griffiths HR, Devitt A, Lip GY, Shantsila E. Monocytes in coronary artery disease and atherosclerosis: Where are we now? J Am Coll Cardiol 2013; 62: 1541–1551.
- 9.
Zawada AM, Rogacev KS, Schirmer SH, Sester M, Böhm M, Fliser D, et al. Monocyte heterogeneity in human cardiovascular disease. Immunobiology 2012; 217: 1273–1284.
- 10.
Heine GH, Ortiz A, Massy ZA, Lindholm B, Wiecek A, Martínez-Castelao A, et al; European Renal and Cardiovascular Medicine (EURECA-m) working group of the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA). Monocyte subpopulations and cardiovascular risk in chronic kidney disease. Nat Rev Nephrol 2012; 8: 362–369.
- 11.
Heine GH, Ulrich C, Seibert E, Seiler S, Marell J, Reichart B, et al. CD14++CD16+ monocytes but not total monocyte numbers predict cardiovascular events in dialysis patients. Kidney Int 2007; 73: 622–629.
- 12.
Rogacev KS, Seiler S, Zawada AM, Reichart B, Herath E, Roth D, et al. CD14++CD16+ monocytes and cardiovascular outcome in patients with chronic kidney disease. Eur Heart J 2011; 32: 84–92.
- 13.
Rogacev KS, Cremers B, Zawada AM, Seiler S, Binder N, Ege P, et al. CD14++CD16+ monocytes independently predict cardiovascular events: A cohort study of 951 patients referred for elective coronary angiography. J Am Coll Cardiol 2012; 60: 1512–1520.
- 14.
Berg KE, Ljungcrantz I, Andersson L, Bryngelsson C, Hedblad B, Fredrikson GN, et al. Elevated CD14++CD16− monocytes predict cardiovascular events. Circ Cardiovasc Genet 2012; 5: 122–131.
- 15.
Emori H, Kubo T, Kameyama T, Ino Y, Matsuo Y, Kitabata H, et al. Diagnostic accuracy of quantitative flow ratio for assessing myocardial ischemia in prior myocardial infarction. Circ J 2018; 82: 807–814.
- 16.
Kubo T, Takahata M, Terada K, Mori K, Arita Y, Ino Y, et al. Retrospective comparison of long-term clinical outcomes between percutaneous coronary intervention and medical therapy in stable coronary artery disease with gray zone fractional flow reserve: COMFORTABLE retrospective study. Circ J 2018; 82: 3044–3051.
- 17.
Swirski FK, Pittet MJ, Kircher MF, Aikawa E, Jaffer FA, Libby P, et al. Monocyte accumulation in mouse atherogenesis is progressive and proportional to extent of disease. Proc Natl Acad Sci USA 2006; 103: 10340–10345.
- 18.
Yang J, Zhang L, Yu C, Yang XF, Wang H. Monocyte and macrophage differentiation: Circulation inflammatory monocyte as biomarker for inflammatory diseases. Biomarker Res 2014; 2: 1.
- 19.
Wildgruber M, Aschenbrenner T, Wendorff H, Czubba M, Glinzer A, Haller B, et al. The “intermediate” CD14++CD16+ monocyte subset increases in severe peripheral artery disease in humans. Sci Rep 2016; 6: 39483.
- 20.
Wildgruber M, Czubba M, Aschenbrenner T, Wendorff H, Hapfelmeier A, Glinzer A, et al. Increased intermediate CD14++CD16+ monocyte subset levels associate with restenosis after peripheral percutaneous transluminal angioplasty. Atherosclerosis 2016; 253: 128–134.
- 21.
Imanishi T, Ikejima H, Tsujioka H, Kuroi A, Ishibashi K, Komukai K, et al. Association of monocyte subset counts with coronary fibrous cap thickness in patients with unstable angina pectoris. Atherosclerosis 2010; 212: 628–635.
- 22.
Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med 2002; 347: 1557–1565.
- 23.
Woollard KJ, Geissmann F. Monocytes in atherosclerosis: Subsets and functions. Nat Rev Cardiol 2010; 7: 77–86.
- 24.
Eriksson EE, Werr J, Guo Y, Thoren P, Lindbom L. Direct observations in vivo on the role of endothelial selectins and alpha(4) integrin in cytokine-induced leukocyte-endothelium interactions in the mouse aorta. Circ Res 2000; 86: 526–533.
- 25.
Ancuta P, Rao R, Moses A, Mehle A, Shaw SK, Luscinskas FW, et al. Fractalkine preferentially mediates arrest and migration of CD16+ monocytes. J Exp Med 2003; 197: 1701–1707.
- 26.
Thieblemont N, Weiss L, Sadeghi HM, Estcourt C, Haeffner-Cavaillon N. CD14lowCD16high: A cytokine-producing monocyte subset which expands during human immunodeficiency virus infection. Eur J Immunol 1995; 25: 3418–3424.
- 27.
Kumari R, Kumar S, Ahmad MK, Singh R, Pradhan A, Chandra S, et al. TNF-α/IL-10 ratio: An independent predictor for coronary artery disease in North Indian population. Diabetes Metab Syndr 2018; 12: 221–225.
- 28.
Kumari R, Kumar S, Ahmad MK, Singh R, Kant Kumar S, Pradhan A, et al. Promoter variants of TNF-α rs1800629 and IL-10 rs1800871 are independently associated with the susceptibility of coronary artery disease in north India. Cytokine 2018; 110: 131–136.