A 62-year-old hypertensive woman was referred to hospital due to dyspnea and chest tightness. She had noticed low grade fever for 1 week. On admission, her blood pressure was 137/79 mmHg and heart rate was 95 beats/min. Physical examination indicated gallop rhythm with no cardiac murmur. Electrocardiogram showed ST elevation in the inferior and anterior leads. Chest X-ray showed mild pulmonary edema. Echocardiogram and cinemagnetic resonance imaging (CMRI) indicated an edematous anteroseptal wall with wall motion abnormality (Figure A). Creatinine kinase was elevated, at 686 IU/L, which was the highest on admission, with no peripheral eosinophilia. Cardiac catheterization showed normal coronary arteries and elevated pulmonary capillary wedge pressure. Right ventricular endomyocardial biopsy was performed.
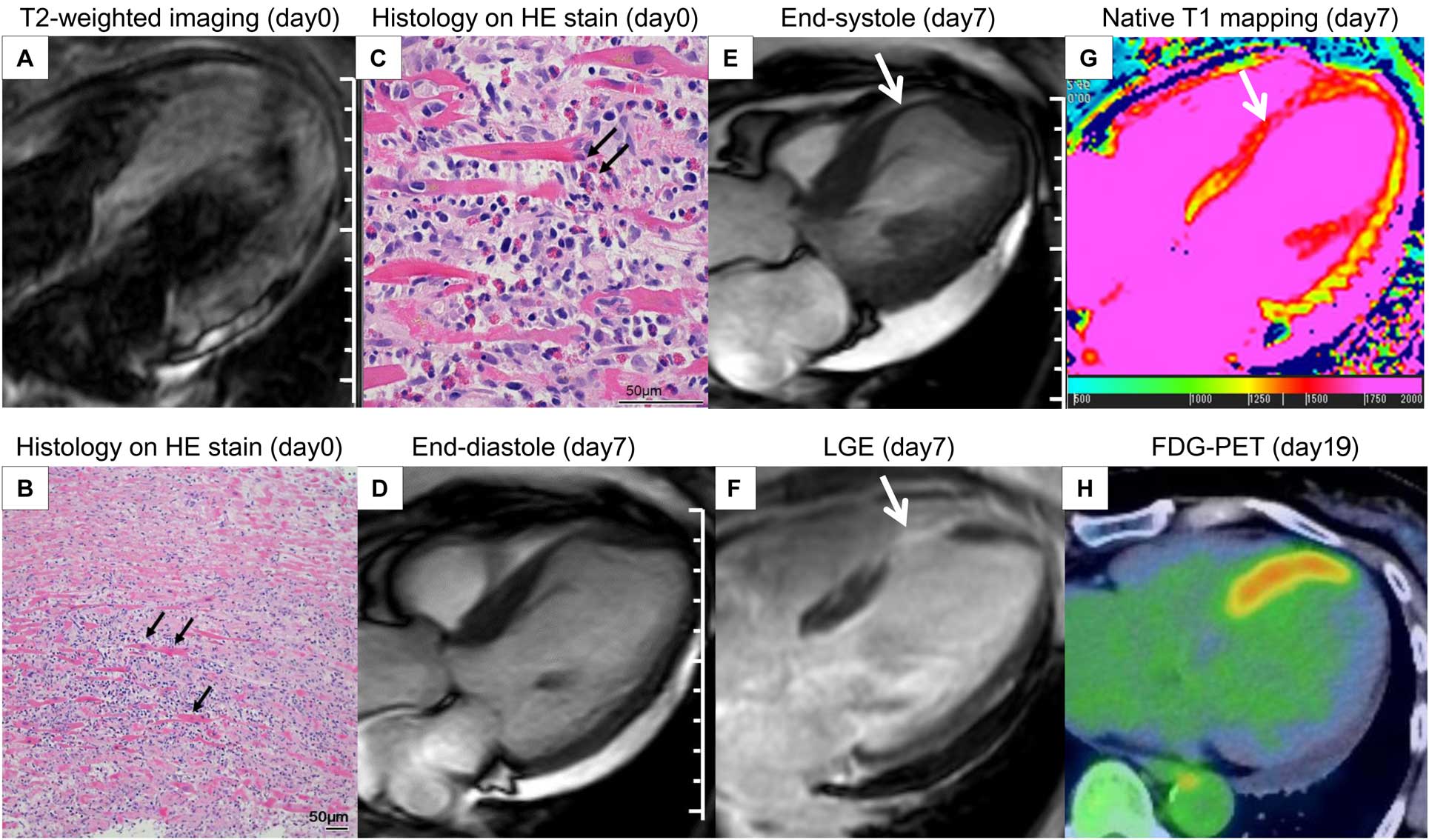
I.v. diuretics and low-dose vasodilator improved symptoms. On day 3, the biopsy specimen had marked interstitial eosinophil infiltration and degranulation, confirming the diagnosis of acute eosinophilic endocarditis (AEM;
Figure B,C). High-dose i.v. corticosteroids (1 g for 3 days) followed by oral prednisone 0.6 mg/kg/day was prescribed. On day 7, repeat CMRI showed localized septal aneurysm (Figure D,E). Increased native T1 (1,635 ms in the septum; normal, 1,294±39 ms) and late gadolinium enhancement in the anteroseptal wall suggested myocardial edema and fibrosis (Figure F,G). On day 19, fluorodeoxyglucose-positron emission tomography still showed a hot uptake in the septum (Figure H).
We herein present an extremely rare case of AEM complicated with ventricular septal aneurysm despite the use of corticosteroids. We speculate that excessive necrosis could have occurred in the septum before corticosteroids were initiated. Given that the degree and duration of eosinophilic exposure are related to disease severity,1
earlier diagnosis of EM and corticosteroids could be crucial to treat AEM with excessive myocardial necrosis.
Disclosures
The authors declare no conflicts of interest.
