Images in Cardiovascular Medicine
Myocardial Rupture Due to Metastasis of Urothelial Carcinoma
2019 Volume 83 Issue 4 Pages 839-

Details
2019 Volume 83 Issue 4 Pages 839-
An 80-year-old man presented with a myocardial rupture due to a metastatic urothelial carcinoma from the left ureter. He was admitted with subacute abdominal bloating caused by widely metastatic cancer of unknown primary origin and left hydronephrosis. During the detection of the primary origin, he suddenly developed a severe cardiac tamponade (Figure A) and died on the same day. Autopsy indicated bloody pericardial fluid and multiple white and well-demarcated myocardial nodules (Figure B, gray arrows), whereas the endocardium and the epicardium were grossly normal. One of the nodules in the right anterior wall penetrated the wall with blood clot and necrosis (Figure B, red arrow), which may have triggered the tamponade. Histologically, the features of the tumor cells were compatible with those of invasive urothelial carcinoma, defined as rounded and enlarged nuclei with clumped chromatin in abundant eosinophilic cytoplasms with rounded contours forming small nests (Figure C,D), and the tumor cells were positive for cytokeratin-7 but not for -20 (data not shown). In addition to the heart, the cancer had metastasized to various locations throughout the body, including the left kidney, lung, liver, and more.
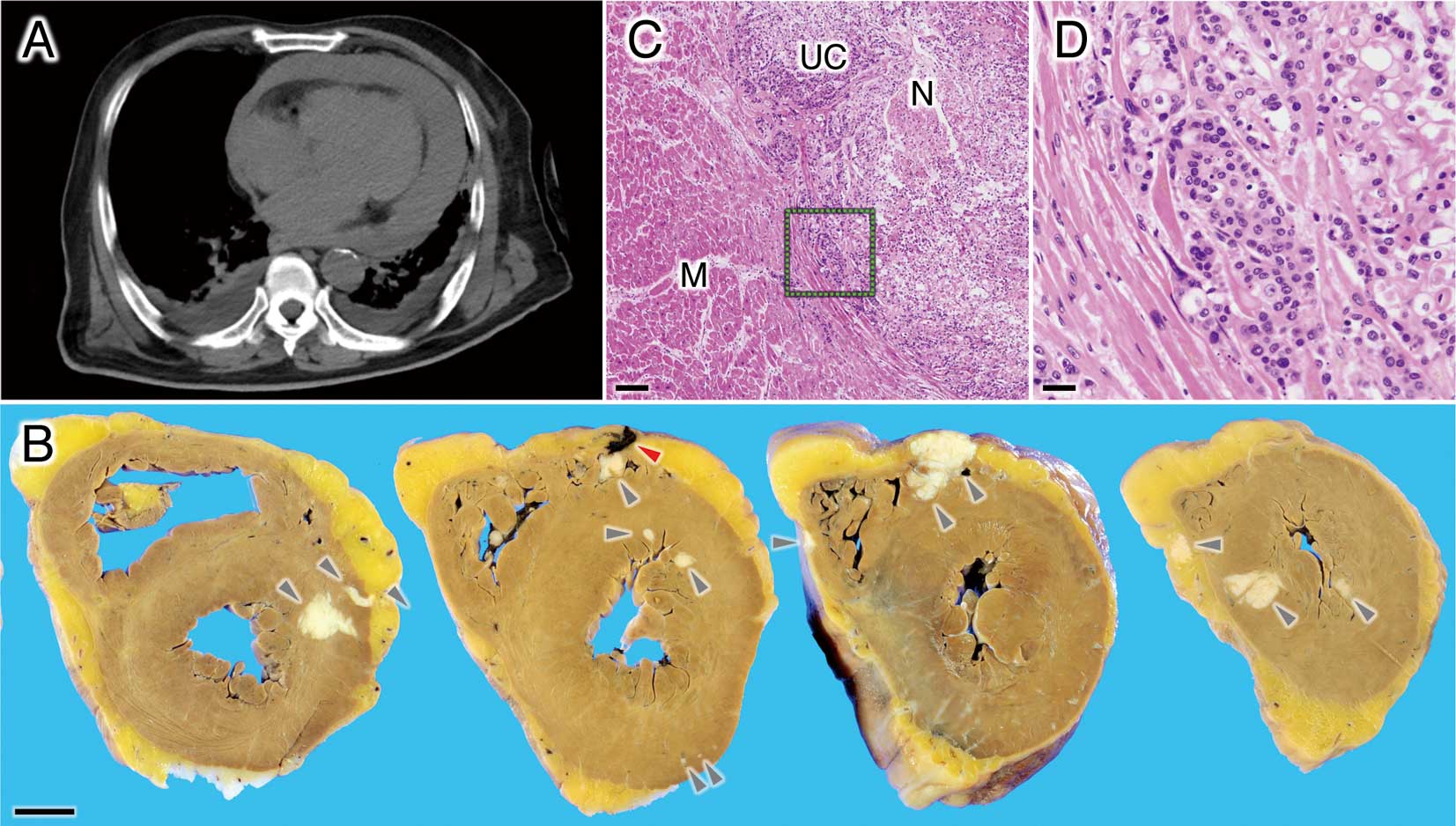
(A) Chest computed tomography showing cardiac tamponade with a fluid of moderate signal intensity. (B) Gross images of the heart. Gray arrowheads, multiple metastatic nodules; red arrowhead, blood clot penetrating the right anterior ventricular wall. Scale bar, 10 mm. (C,D) Microscopy of the metastatic tumor: (C) Low-power field. M, myocardium; N, necrosis; UC, urothelial carcinoma. Scale bar, 200 µm. (D) High-power field. Scale bar, 50 µm.
Metastasis to the heart is more frequent than one might suspect. The frequency of secondary metastatic tumors in the cardiovascular system has been reported to be up to 9.1% in patients with known malignancies,1,2 whereas primary cardiac tumors are extremely rare. Although the major causes of cardiac metastasis are lung cancer, breast cancer, hematologic malignancies, and malignant melanoma,2 a few cases derived from urothelial carcinoma have been reported.3,4 Most cardiac metastases are associated with widely metastatic conditions in late-stage cancer, and are often clinically silent.2 Thus, they tend to be diagnosed on postmortem examination. They should always be taken into consideration, however, when treating cancer patients with cardiac symptoms, because radiotherapy, chemotherapy, or catheterization would be useful tools for palliative and/or life-prolonging treatment in some cases.1,2
The authors declare no conflicts of interest.