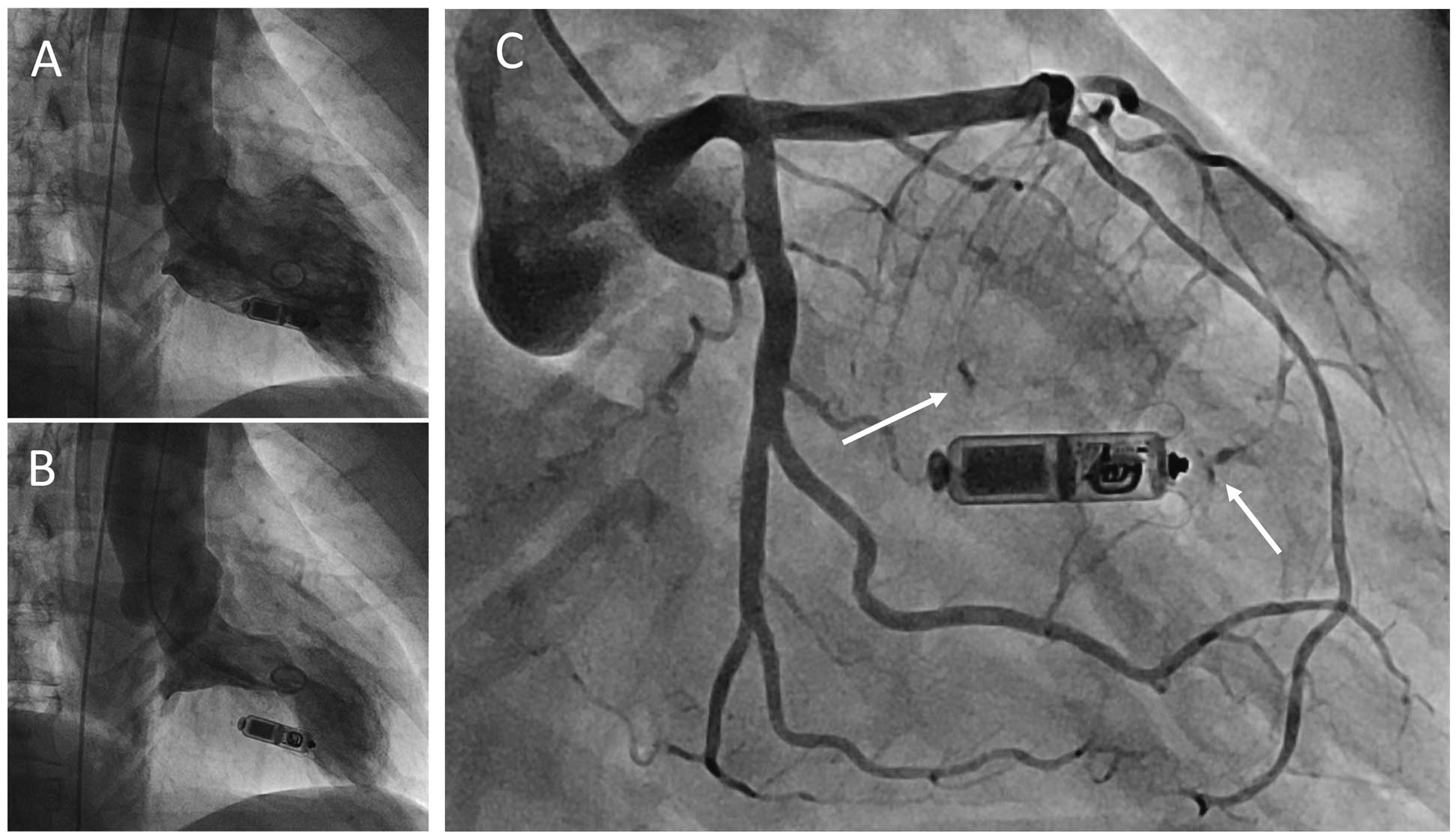
A 73-year-old woman was referred to hospital for pacemaker implantation due to transient atrioventricular block. She was on hemodialysis with a permanent indwelling catheter through the right subclavian vein, therefore we decided to implant a leadless pacemaker (LLPM). The first attempt at LLPM implantation failed because of a high pacing threshold at mid-septum, followed by successful implantation at lower mid-septum without any adverse events, but the patient complained of chest discomfort 1 week later. Electrocardiogram showed ST-segment elevation in the precordial leads. Coronary angiography (CAG) showed no significant stenosis in the epicardial coronary arteries, but left ventriculography showed takotsubo-like asynergy in diastole (Figure A) and systole (Figure B), which led to the diagnosis of takotsubo cardiomyopathy. CAG also indicated septal branch injuries at the LLPM implantation site and at the first attempt site (Figure C; Supplementary Movies 1,2).
The complication rate of LLPM implantation is slightly higher compared with that of conventional pacemaker implantation.1
In this case, the injury was clinically irrelevant, and fortunately additional intervention was not needed. The symptoms were thought to be due to takotsubo cardiomyopathy, not to the coronary injury, but there is a risk of critical coronary injury in LLPM implantation. Operators should choose the appropriate implantation site carefully, and refrain from multiple attempts at implantation in order to minimize the complication risk.
Disclosures
The authors declare no conflicts of interest.
Supplementary Files
Supplementary Movie 1.
CAG in RAO view.
Supplementary Movie 2.
CAG in RAO-Cranial view.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-19-0882
