Images in Cardiovascular Medicine
Role of Invasive Hemodynamic Assessment During Trans-Catheter Paravalvular Leak Intervention
2020 Volume 84 Issue 3 Pages 531-

Details
2020 Volume 84 Issue 3 Pages 531-
A 54-year-old man had undergone surgical aortic and mitral valve replacement in 1999 for underlying rheumatic heart disease. His other medical conditions were chronic renal failure, treated with home peritoneal dialysis, and permanent atrial fibrillation. He had worsening dyspnea on exertion and had needed excess fluid removal during dialysis over the last 2 years. On further investigation he was found to have severe mitral paravalvular leak (PVL; Figure A) and hemolysis. After multi-disciplinary team discussion, he accepted trans-catheter closure of the mitral PVL. Under general anesthesia, after septal puncture the mean left atrial (LA) pressure was 25 mmHg with a V wave of 46–48 mmHg (Figure B), whereas trans-esophageal echocardiogram (TEE) demonstrated significant mitral PVL into the dilated LA. Angulation on fluoroscopy to view the vascular plug at the edge of the metallic mitral prosthesis was extreme right anterior oblique cranial. After initial deployment of an Amplatzer Vascular Plug III (14/5 mm), TEE demonstrated a well-positioned device (Figure C), but the hemodynamic tracing indicated mean LA pressure with a relatively prominent V wave (Figure D). Repeated attempts at capture and re-positioning of the device resulted in further reduction in the mean LA pressure and specifically the V wave (Figure F), although TEE appearence remained unchanged (Figure E). After confirmation of stability, the vascular plug was released, producing an excellent final result and symptomatic improvement.
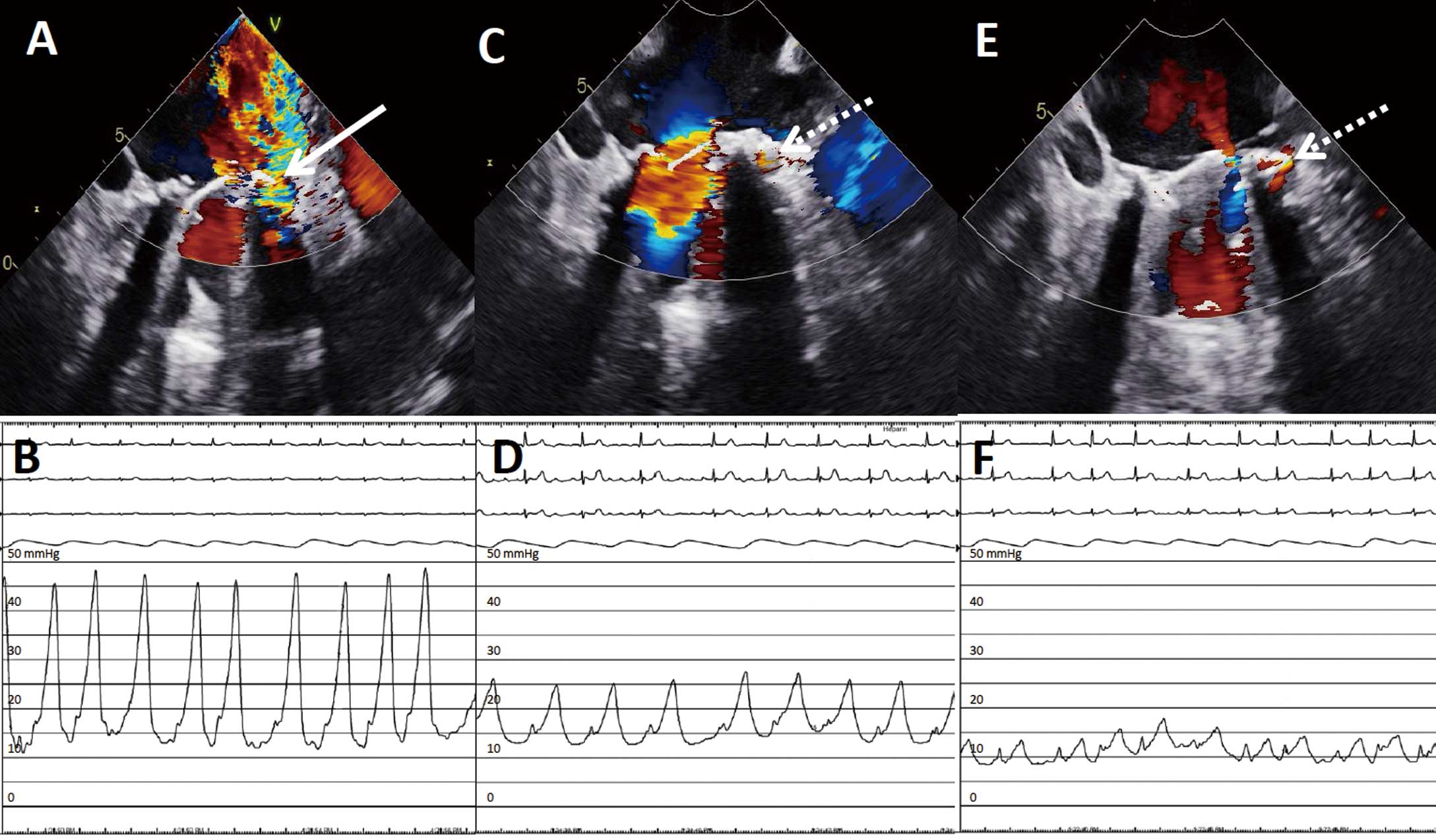
(A,C,E) Trans-esophageal echocardiography of mitral paravalvular regurgitation at (A) baseline; and after (C) initial and (E) final device deployment. (B,D,F) Hemodynamic tracing from the left atrium at (B) baseline, and after (D) initial and (F) final device deployment. Solid arrow, mitral paravalvular leak; broken arrow, deployed Amplatzer vascular plug.
Trans-catheter intervention in PVL offers an effective and alternative therapy to high-risk surgical repair. Although hemodynamic assessment of mitral PVL severity by measuring pulmonary capillary wedge or LA pressure has rarely been recommended, intra-procedural LA pressure measurement, in addition to TEE evaluation, should be utilized to achieve satisfactory procedural outcomes. It is paramount that the operators use all means available to assess the effectiveness of such an intervention.
The authors declare no conflicts of interest.