Abstract
Background:
Characteristics and treatment outcomes of acute myocardial infarction (AMI) patients have been studied; however, those of recent myocardial infarction (RMI) patients remain unclear. This study aimed to clarify characteristics, treatment strategy, and in-hospital outcomes of RMI patients in the Tokyo CCU network database.
Methods and Results:
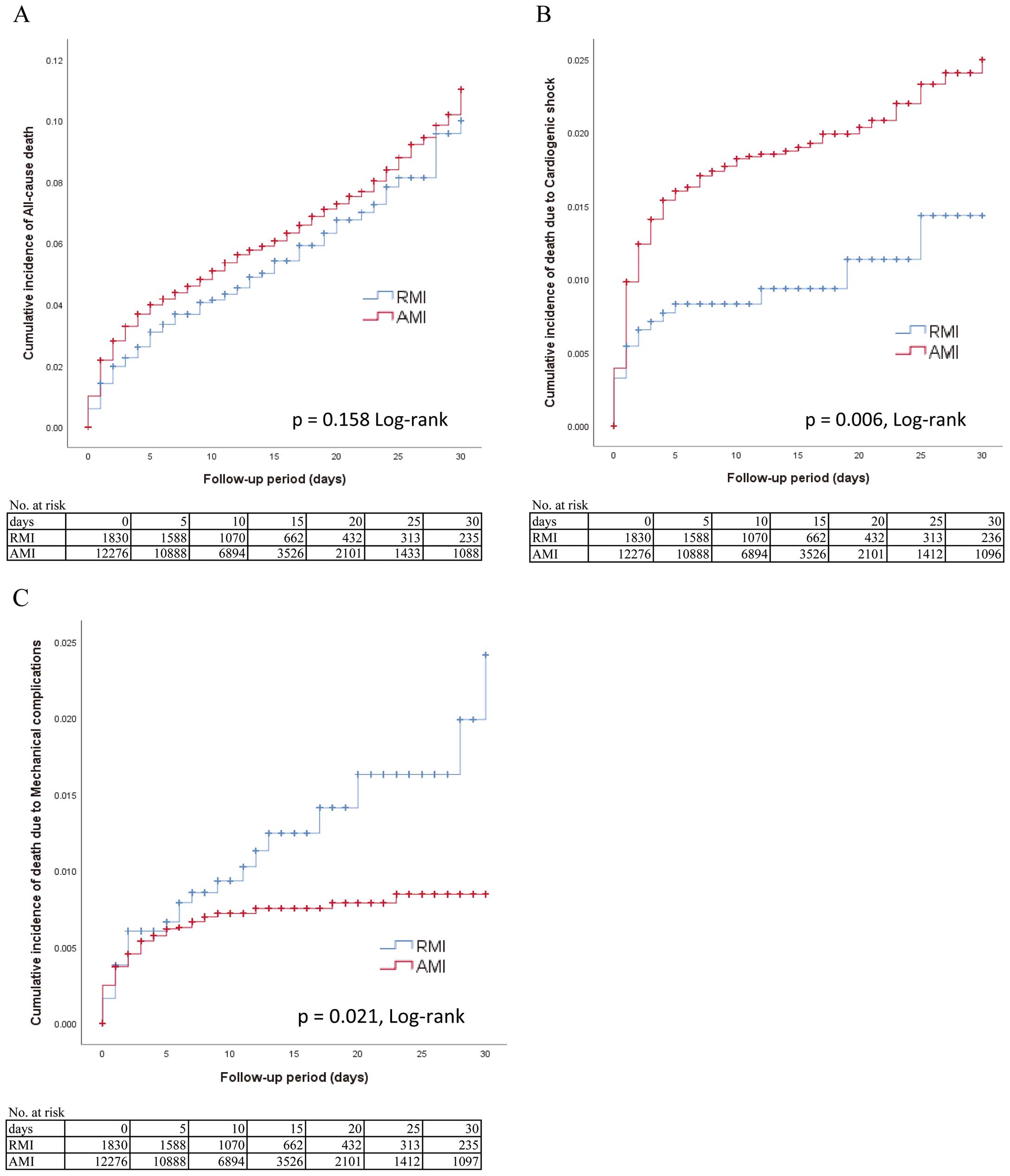
In total, 1,853 RMI and 12,494 AMI patients from the Tokyo CCU network database during 2013–2016 were compared. Both RMI and AMI were redefined by onset times of 2–28 days and ≤24 h, respectively. The RMI group had a higher average age (70.4±12.9 vs. 68.0±13.4 years, P<0.001), more women (27.6% vs. 23.6%, P<0.001), lower proportion of patients with chest pain as the chief complaint (75.2% vs. 83.6%, P<0.001), higher prevalence of diabetes mellitus (35.9% vs. 31.0%, P<0.001), and higher mechanical complication incidence (3.0% vs. 1.5%, P<0.001) than did the AMI group. Thirty-day mortality was comparable (5.3% vs. 5.8%, P=0.360); major causes of death were cardiogenic shock and mechanical complications in the AMI and RMI groups, respectively. Death from mechanical complications (not onset time) in the AMI group plateaued almost 1 week after hospitalization, whereas it continued to increase in the RMI group.
Conclusions:
Both RMI and AMI patients have distinctive clinical features, sequelae, and causes of death. Although treatment of RMI patients adhered to guidelines, it was insufficient, and death from mechanical complications continues to increase.
Acute myocardial infarction (acute MI; AMI) is a major cause of morbidity and mortality, not only in Japan, but also worldwide. Patient characteristics and outcomes of AMI have been sufficiently investigated and treatment strategies have been established, such as the earlier primary percutaneous coronary intervention (PCI).1–5
In contrast, in asymptomatic patients, routine PCI of an occluded infarct-related artery 24 or 48 h or more after onset is not indicated, especially for ST-segment elevation MI (STEMI).3,6–8
However, the clinical features of these recent MI (RMI) 24 h or more after onset have not been fully evaluated. Furthermore, even in this modern age when the prognosis of AMI patients has improved, there are a certain number of RMI patients whose prognosis has not improved. Accordingly, the purpose of the present study was to clarify characteristics, treatment strategy, and in-hospital outcomes of RMI patients in the Tokyo CCU network database within the contemporary real-world setting.
Methods
Study Design
This study was performed using data from the Tokyo CCU network database, collected between January 2013 and December 2016. Only the data of patients with MI were selected. Diagnoses of AMI were based on the universal definition.9
The therapeutic strategies for AMI were decided by the cardiologists in each hospital, and all patients received treatment according to the Japanese Circulation Society, European Society of Cardiology, and American Council for Capital Formation/American Heart Association guidelines for the treatment of MI.2–4
The Tokyo CCU network database is an ongoing multicenter registry that prospectively collects information regarding emergency admissions to acute cardiac care facilities in Japan.10
The Tokyo CCU network was established in 1978 with the goal of treating patients with emergency cardiovascular events as promptly as possible, with the help of ambulance units dispatched through the Tokyo Fire Department. Deducing from the regional distribution of these 72 hospitals (as of 31 December 2016), the Tokyo CCU network probably includes 95% of all patients who have had an AMI within the Tokyo metropolitan area, serving a population of 13.5 million.5
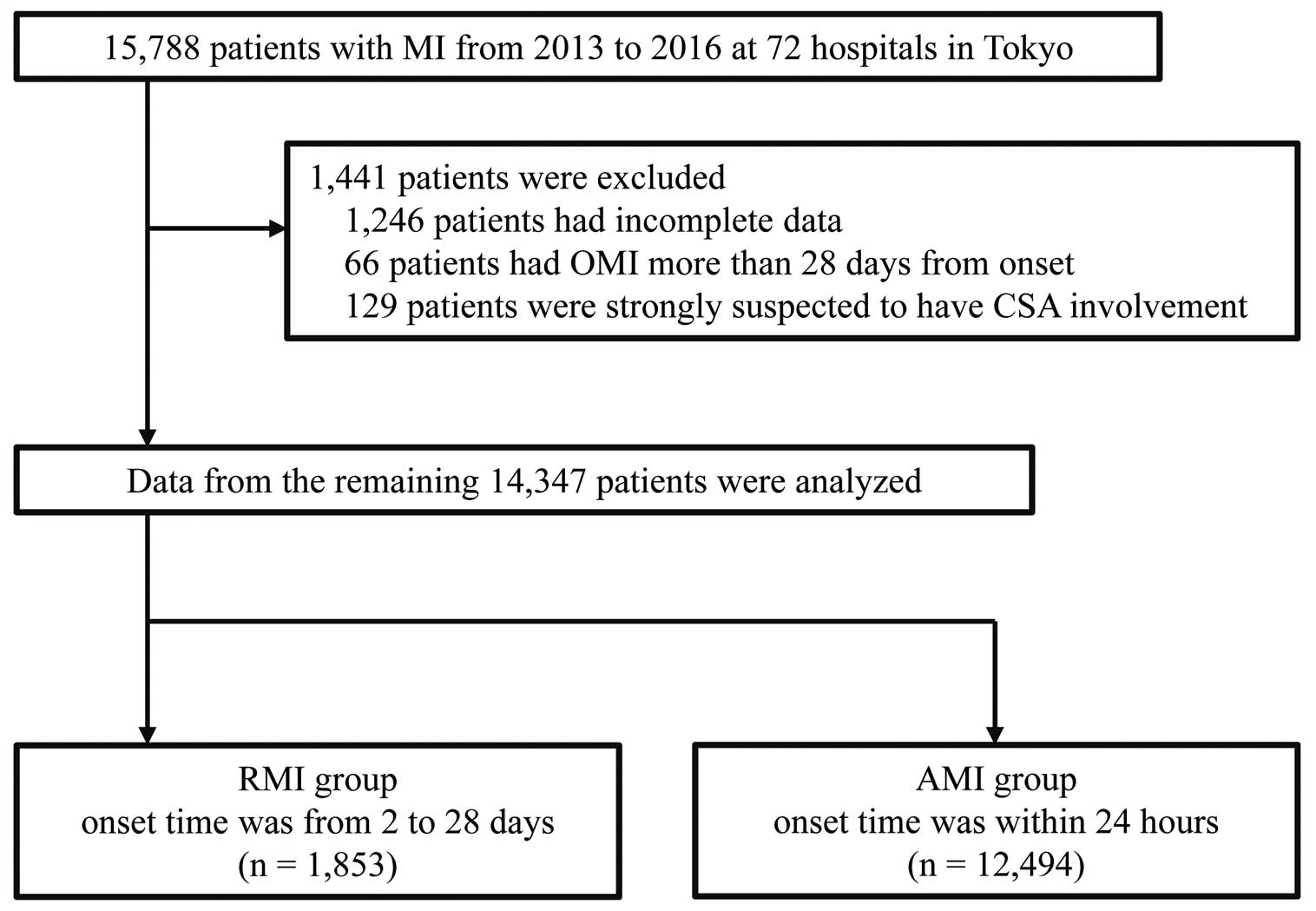
For this study, 15,788 consecutive patients who satisfied the MI definition were identified. However, 1,246 patients (2 patients based on age, 9 on detailed diagnosis, 389 on Killip classification, 61 on ST-segment elevation, 228 on medical history, 139 on medical treatment, 42 on angiographic findings, 287 on invasive treatment, and 89 on clinical outcomes and early post-infarction complications) with incomplete data, were excluded from the analysis. We also excluded 66 patients with old MI of more than 28 days from onset and 129 patients strongly suspected of involvement of coronary spastic angina. Data from the remaining 14,347 patients were analyzed. Both RMI and AMI were redefined as follows: RMI patients whose onset-time was from 2 to 28 days and AMI patients whose onset-time was within 24 h. We compared 1,853 RMI patients and 12,494 AMI patients (Figure 1).
This study was conducted in accordance with the Declaration of Helsinki, in line with the Ethical Guidelines for Epidemiological Research by the Japanese government and approved by the Ethics Committee of the Tokyo CCU Network Scientific Committee (approval number 16-002). According to the guidelines, the study satisfied the conditions for waiving the requirement for informed consent from individual participants, which was approved by the Ethics Committee of Tokyo CCU Network Scientific Committee. In accordance with rules set forth by the Ministry of Internal Affairs and Communications, patient data collection policies are displayed at each individual Tokyo CCU network institution, and patients can refuse to provide their own data.
Data Collection and Endpoint
Individual clinical information is recorded into the database by network members at each institution, and the final datasets are collected by the Tokyo CCU Network Scientific Committee under anonymity, according to the ethical guidelines on epidemiological surveys released from the Japanese Ministry of Health, Labor, and Welfare. Data collection and maintenance for the Tokyo CCU network registry were financially supported by the Tokyo Metropolitan Government, which had no role in the execution of this study or the interpretation of the results. From the hospital records of eligible patients, we extracted information on demographics, medical history, clinical data, clinical course, and the use of therapeutic interventions such as PCI, surgery, and medical circulatory support. The primary endpoint was all-causes of hospital mortality within 30 days, beginning from the first day of hospitalization. For this study, it is important to note the 30-day follow-up period after admission and that there were no data on prognosis collected after discharge.
Statistical Analysis
Continuous variables were presented as means±standard deviations or medians and interquartile range, and categorical variables as percentages. Categorical variables were tested using the Chi-squared test or, if not applicable, Fisher’s exact test. Continuous variables were presented as means±standard deviations and were tested using the Student’s t-test or the Mann-Whitney U-test. In the Chi-squared analyses involving variables with more than 2 coding categories, adjusted standardized residuals were used to identify the contribution of different cells to the significance of the chi squares. Cumulative mortality during the first 30 days after admission was evaluated using Kaplan-Meier curves, and a log-rank test was used for comparisons between the groups.
For all analyses, 2-tailed probability values of <0.05 were considered significant. Statistical analysis was performed using IBM SPSS statistics 25 (IBM Corporation, Armonk, NY, USA).
Results
Baseline Clinical Characteristics
Baseline characteristics were different in several aspects between the RMI and AMI groups (Table 1). Elderly females with low body mass index (BMI) were significantly more common in the RMI than the AMI group. Although most patients with AMI complained of chest pain, the prevalence of dyspnea was higher in patients with RMI than in those with AMI. The RMI group had a significantly higher prevalence of hypertension, diabetes mellitus, and peripheral artery disease. The RMI group had more Killip class II and III patients and more patients who had self-hospitalized, and only half of the RMI group had availed ambulance transportation services (including inter-hospital transfer). ST-segment elevation was more common in the AMI group. The RMI profile tended to involve high C-reactive protein (CRP) on admission and lower maximum creatine phosphokinase (CPK). There were no significant differences in the prevalence of dyslipidemia and smoking history between the 2 groups. Onset-to-balloon time and door-to-balloon time tended to be shorter in the AMI group than in the RMI group. However, there was a substantial amount of missing data in the time course; in particular, the differences between door-to-balloon time and onset-to-balloon time were because of missing door-time data in several cases. The percentage of missing data was 18.1%, 41.5%, and 1.6% for onset-time, door-time, and balloon-time, respectively. With the exception of time course, the mean percentage of missing data among variables in
Table 1
was 1.1% for both groups; the highest proportion of missing data was for smoking history (5.6% and 6.6%), followed by BMI (4.9% and 6.7%) and value of max CPK (5.8% and 3.2%), respectively.
Table 1.
Baseline Clinical Characteristics
| |
Total |
RMI |
AMI |
P value |
| n |
14,347 |
1,853 |
12,494 |
|
| Age (years) |
68.3±13.3 |
70.4±12.9 |
68.0±13.4 |
<0.001 |
| Female |
3,459 (24.1) |
511 (27.6) |
2,948 (23.6) |
<0.001 |
| BMI (kg/m2) |
23.8±4.0 |
23.6±4.0 |
23.9±4.0 |
0.003 |
| Coronary risk factor |
| Hypertension |
8,730 (60.8) |
1,175 (63.4) |
7,555 (60.5) |
0.015 |
| Dyslipidemia |
6,041 (42.1) |
769 (41.5) |
5,272 (42.2) |
0.571 |
| Diabetes mellitus |
4,538 (31.6) |
665 (35.9) |
3,873 (31.0) |
<0.001 |
| Smoking |
7,642 (56.9) |
970 (55.4) |
6,672 (57.2) |
0.172 |
| Hyperuricemia |
842 (5.9) |
142 (7.7) |
700 (5.6) |
<0.001 |
| Cardiovascular history |
| MI |
1,161 (8.1) |
118 (6.4) |
1,043 (8.3) |
0.004 |
| PCI |
1,435 (10.0) |
132 (7.1) |
1,303 (10.4) |
<0.001 |
| CABG surgery |
231 (1.6) |
27 (1.5) |
204 (1.6) |
0.575 |
| Heart failure |
276 (1.9) |
34 (1.8) |
242 (1.9) |
0.765 |
| Cerebral infarction |
923 (6.4) |
122 (6.6) |
801 (6.4) |
0.777 |
| Hemodialysis |
398 (2.8) |
54 (2.9) |
344 (2.8) |
0.694 |
| Peripheral artery disease |
225 (1.6) |
42 (2.3) |
183 (1.5) |
0.010 |
| Chief complaint |
| Chest pain |
11,841 (82.5) |
1,394 (75.2) |
10,447 (83.6) |
<0.001 |
| Dyspnea |
1,470 (10.2) |
312 (16.8) |
1,158 (9.3) |
<0.001 |
| Killip classification |
|
|
|
<0.001 |
| Class I |
10,235 (72.7) |
1,277 (70.5) |
8,958 (73.1) |
|
| Class II |
1,748 (12.4) |
311 (17.2) |
1,437 (11.7) |
|
| Class III |
749 (5.3) |
119 (6.6) |
630 (5.1) |
|
| Class IV |
1,337 (9.5) |
105 (5.8) |
1,232 (10.1) |
|
| SBP (mmHg) |
135 (116–156) |
132 (114–150) |
136 (116–157) |
<0.001 |
| HR (beats/min) |
80.0±21.9 |
83.9±21.6 |
79.4±21.9 |
<0.001 |
| Laboratory findings |
| Maximum CPK value (IU/L) |
1,470 (591–3,123) |
627 (275–1,437) |
1,629 (686–3,346) |
<0.001 |
| CRP (mg/dL) |
0.25 (0.10–0.78) |
1.21 (0.29–5.27) |
0.20 (0.09–0.55) |
<0.001 |
| Hospitalization process |
|
|
|
<0.001 |
| Ambulance transportation services (including inter-hospital transfer) |
10,629 (74.3) |
1,008 (54.6) |
9,621 (77.2) |
|
| Self-hospitalization |
2,773 (19.3) |
701 (37.8) |
2,072 (16.6) |
|
| In-hospital onset |
419 (2.9) |
42 (2.3) |
377 (3.0) |
|
| ST-segment elevation |
10,908 (76.0) |
1,167 (63.0) |
9,741 (78.0) |
<0.001 |
| Time course |
| |
(n=7,450) |
(n=510) |
(n=6,940) |
|
| Door-to-Balloon time (min) |
71.0 (48.0–109.0) |
99.5 (58.0–281.0) |
69.0 (48.0–105.0) |
<0.001 |
| |
(n=10,482) |
(n=661) |
(n=9,821) |
|
| Onset-to-Balloon time (h) |
3.95 (2.33–9.50) |
41.2 (22.9–81.2) |
3.67 (2.25–7.83) |
<0.001 |
Data are presented as n (%), mean±standard deviation (SD), or median (interquartile range; IQR), unless otherwise stated. AMI, acute myocardial infarction; BMI, body mass index; CABG, coronary artery bypass grafting; CPK, creatine phosphokinase; CRP, C-reactive protein; HR, heart rate; MI, myocardial infarction; PCI, percutaneous coronary intervention; RMI, recent myocardial infarction; SBP, systolic blood pressure.
Medication during hospitalization such as antiplatelet and statin were used more frequently in AMI than RMI patients, with the exception of β-blocker, which was not significantly different (Table 2). The mean percentage of missing data among variables in
Table 2
was 0.5% in the RMI and 0.4% in the AMI group; the highest proportion of missing data was for statin (both 0.8%).
Table 2.
Medication During Hospitalization
| |
Total |
RMI |
AMI |
P value |
| Heparin |
13,209 (92.5) |
1,667 (90.5) |
11,542 (92.8) |
<0.001 |
| Aspirin |
13,604 (95.1) |
1,729 (93.7) |
11,875 (95.3) |
0.003 |
| Thienopyridine |
12,239 (85.6) |
1,480 (80.2) |
10,759 (86.4) |
<0.001 |
| Statin |
11,740 (82.5) |
1,439 (78.3) |
10,301 (83.1) |
<0.001 |
| β-blocker |
9,746 (68.2) |
1,242 (67.3) |
8,504 (68.3) |
0.400 |
| ACEI / ARB |
9,602 (67.2) |
1,200 (65.0) |
8,402 (67.5) |
0.037 |
Data are presented as n (%). ACEI, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II receptor blocker. Other abbreviations as in Table 1.
The RMI group had more left anterior descending artery (LAD) lesions and multi-vessel coronary disease than the AMI group. Initial Thrombolysis in MI (TIMI) flow grade 0 was less prevalent in the RMI group than in the AMI group. Compared with the AMI group, fewer patients underwent emergency coronary angiography (CAG), and PCI treatment was reduced, but more patients underwent coronary artery bypass grafting (CABG) in the RMI group. The frequency of using the circulatory assist device was higher in the AMI group (Table 3). The attainment rate of final TIMI flow grade 3 was similar in the 2 groups, whereas the prevalence of PCI within 90 min or 24 h of door-to-balloon times was less in the RMI group. The mean percentage of missing data among variables in
Table 3
was 4.8% in the RMI and 1.7% in the AMI group; the highest proportion of missing data was for initial TIMI flow grade (12.9% and 6.6%), followed by infarct-related artery (11.2% and 3.9%), and multi-vessel coronary disease (8.9% and 2.7%), respectively.
Table 3.
Angiographic Findings and Invasive Procedures
| |
Total |
RMI |
AMI |
P value |
| Emergency CAG |
13,748 (95.8) |
1,655 (89.3) |
12,093 (96.8) |
<0.001 |
| Location of culprit lesion |
|
|
|
<0.001 |
| RCA |
4,935 (36.2) |
512 (31.1) |
4,423 (36.8) |
|
| LMT |
341 (2.5) |
28 (1.7) |
313 (2.6) |
|
| LAD |
6,373 (46.7) |
855 (52.0) |
5,518 (46.0) |
|
| LCX |
1,923 (14.1) |
242 (14.7) |
1,681 (14.0) |
|
| Others |
78 (0.6) |
8 (0.5) |
70 (0.6) |
|
| Multi-vessel coronary disease |
6,349 (45.9) |
924 (54.7) |
5,425 (44.6) |
<0.001 |
| Initial TIMI flow |
|
|
|
<0.001 |
| Grade 0 |
7,537 (56.7) |
758 (47.0) |
6,779 (58.0) |
|
| Grade 1 |
1,679 (12.6) |
236 (14.6) |
1,443 (12.4) |
|
| Grade 2 |
2,090 (15.7) |
312 (19.3) |
1,778 (15.2) |
|
| Grade 3 |
1,981 (14.9) |
308 (19.1) |
1,673 (14.3) |
|
| Treatment |
| PCI |
12,852 (89.6) |
1,463 (79.0) |
11,389 (91.2) |
<0.001 |
| TIMI grade 3 flow post PCI |
11,772 (93.9) |
1,330 (93.2) |
10,442 (93.9) |
0.271 |
| |
(n=7,450) |
(n=510) |
(n=6,940) |
|
| Door-to-balloon times under 90 min |
4,959 (66.6) |
234 (45.9) |
4,725 (68.1) |
<0.001 |
| Door-to-balloon times under 24 h |
7,177 (96.3) |
420 (82.4) |
6,757 (97.4) |
<0.001 |
| CABG |
521 (3.7) |
110 (6.0) |
411 (3.3) |
<0.001 |
| IABP |
2,294 (16.0) |
221 (11.9) |
2,073 (16.6) |
<0.001 |
| ECMO |
450 (3.1) |
27 (1.5) |
423 (3.4) |
<0.001 |
Data are presented as n (%). CAG, coronary angiography; ECMO, extra-corporeal membrane oxygenation; IABP, intra-aortic balloon pumping; LAD, left anterior descending artery; LCX, left circumflex artery; LMT, left main coronary trunk; RCA, right coronary artery; TIMI, Thrombolysis in Myocardial Infarction. Other abbreviations as in Table 1.
The incidence of mechanical complications was increased in the RMI group (3.0% vs. 1.5%, P<0.001). Detailed examination of mechanical complications revealed a similar prevalence of cardiac rupture in the 2 groups, and an increased prevalence of ventricular septal rupture for the RMI group (1.5% vs. 0.3%, P<0.001). The occurrence of ventricular tachycardia and fibrillation were more frequent in the AMI group as arrhythmic complications (Table 4). There were no missing data among the variables in
Table 4.
Table 4.
Early Post-Infarction Complications
| |
Total |
RMI |
AMI |
P value |
| Mechanical complications |
246 (1.7) |
56 (3.0) |
191 (1.5) |
<0.001 |
| Cardiac rupture |
136 (0.9) |
24 (1.3) |
112 (0.9) |
0.098 |
| Ventricular septal rupture |
70 (0.5) |
27 (1.5) |
43 (0.3) |
<0.001 |
| Papillary muscle rupture |
20 (0.1) |
2 (0.1) |
18 (0.1) |
0.512 |
| Arrhythmia event |
| VT/VF |
643 (4.5) |
48 (2.6) |
595 (4.8) |
<0.001 |
Data are presented as n (%). VF, ventricular fibrillation; VT, ventricular tachycardia. Other abbreviations as in Table 1.
During the 30-day follow-up period, all-causes of death occurred in 98 patients in the RMI and in 727 patients in the AMI group. In-hospital 30-day mortality was equivalent between the 2 groups (5.3% vs. 5.8%, P=0.360); the major cause of death in the AMI group was cardiogenic shock, whereas in the RMI group, it was mechanical complications (Table 5). There were no missing data among the variables in
Table 5. Stratified sub-analyses of STEMI and non-STEMI (NSTEMI) were conducted for the incidence of mechanical complications and 30-day mortality (Table 6). In the stratified analyses of STEMI and NSTEMI, the incidence of mechanical complications was increased in the RMI group, as in the overall analysis. There was no difference in the 30-day mortality rate between the 2 groups in the STEMI analysis, whereas in the RMI group, a lower 30-day mortality rate compared with the AMI group was found in the NSTEMI analysis. On Kaplan-Meier analysis, the 2 groups did not differ in all-causes of death, although there were significantly different cumulative incidences of death due to cardiogenic shock (P=0.006, Log-rank test) and mechanical complications (P=0.021, Log-rank test). Furthermore, death due to mechanical complications (not onset time) in the AMI group plateaued after about 1 week from hospitalization, whereas in the RMI group, it continued to increase (Figure 2A–C). As mentioned above, it is important to note the 30-day follow-up period after admission, and that there were no data on long-term prognosis in this study.
Table 5.
Clinical Outcomes
| |
Total |
RMI |
AMI |
P value |
| 30-day mortality |
825 (5.8) |
98 (5.3) |
727 (5.8) |
0.360 |
| Cause of death |
(n=825) |
(n=98) |
(n=727) |
0.024 |
| Cardiogenic shock |
248 (30.1) |
18 (18.4) |
230 (31.6) |
|
| Mechanical complications |
111 (13.5) |
22 (22.4) |
89 (12.2) |
|
| Multiple organ failure |
104 (12.6) |
10 (10.2) |
94 (12.9) |
|
| Cardiac failure |
75 (9.1) |
10 (10.2) |
65 (8.9) |
|
| Fatal arrhythmia |
82 (9.9) |
11 (11.2) |
71 (9.8) |
|
| Others |
205 (24.8) |
27 (27.6) |
178 (24.5) |
|
Data are presented as n (%). Abbreviations as in Table 1.
Table 6.
Stratified Analysis for STEMI and NSTEMI
| |
Total |
RMI |
AMI |
P value |
| STEMI group |
| n |
10,908 |
1,167 |
9,741 |
|
| Mechanical complications |
216 (2.0) |
42 (3.6) |
174 (1.8) |
<0.001 |
| 30-day mortality |
602 (5.5) |
65 (5.6) |
537 (5.5) |
0.936 |
| NSTEMI group |
| n |
3,439 |
686 |
2,753 |
|
| Mechanical complications |
31 (0.9) |
14 (2.0) |
17 (0.6) |
<0.001 |
| 30-day mortality |
223 (6.5) |
33 (4.8) |
190 (6.9) |
0.047 |
Data are presented as n (%). NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction. Other abbreviations as in Table 1.
Discussion
To the best of our knowledge, this is the first retrospective multicenter observational study to demonstrate the clinical differences between RMI and AMI in contemporary Japanese clinical practice. One of the relevant findings of the present study was that the RMI group tended to include more elderly females with a history of hypertension and diabetes mellitus. In general, ACS with atypical symptoms or no symptoms is often seen in elderly, diabetic, and female patients.11–14
As such, the diagnosis of AMI may be delayed or missed.15
In addition, the elderly have more comorbidities and are less likely to receive reperfusion therapy than younger patients.16,17
Females also tend to present more often with atypical symptoms; up to 30% in some registries.15,18,19
Even if the elderly female patients do not experience typical chest pain, it is necessary to instruct them to visit a hospital as soon as possible with any symptoms, particularly with dyspnea.
The second contribution of the present study was, despite finding that there was no difference in the in-hospital mortality rate of RMI patients compared with AMI patients, that the major cause of death was different; RMI patients had more mechanical complications. Furthermore, death due to mechanical complications continued to increase in RMI patients even while continuing hospitalization treatment. A long time from onset to hospitalization (especially ≥24 h) is a risk for occurrence of mechanical complications.20,21
In a previous study investigating 5,230 MIs, 77 mechanical complications (1.5%) were observed, and performing reperfusion therapy and time from symptom onset to hospitalization ≥6 h were independent predictors of mechanical complications.20
The incidence of mechanical complications in the present study was similar to previous reports, and was higher in the RMI group, which was also the same in the stratified analyses of STEMI and NSTEMI. Another study also reported that timely reperfusion therapy and administration of β-blocker, angiotensin-converting enzyme inhibitor (ACEI), and aspirin are effective in reducing the incidence of mechanical complications.22
The study found that aspirin, statins, and cardioprotective drugs such as ACEI and β-blocker were not sufficiently introduced, especially in patients with RMI, and optimal medical therapy for RMI patients might leave the door open to reduced mechanical complications.
As described above, RMI and AMI have different patient populations. RMI patients are considered to be a group of patients who have survived through the hyperacute phase of AMI, which has the highest mortality. The exact mortality rate of RMI patients is unknown because it is not possible to analyze patients who could not reach the hospital or those who did not visit the hospital without complications, but at least in-hospital mortality was equivalent to AMI. In RMI patients, deaths due to mechanical complications continued to increase even as hospitalization continued. In the stratified analyses of STEMI and NSTEMI, the incidence of mechanical complications was increased in the RMI group, as was the case in the overall analysis. However, there might have been more low-risk patients in the RMI group because of the lower mortality rate associated with NSTEMI than with STEMI. In other words, RMI patients might have had STEMI or NSTEMI; those with STEMI had advanced infarction and severe myocardial damage but survived until reaching the hospital, and those with NSTEMI had troponin positivity but no major myocardial damage. As the RMI severity may vary among patients, treatment strategies for RMI may need to be established separately from those for AMI. Further research to determine the optimal treatment strategy for RMI patients needs to be conducted.
Study Limitations
There are several limitations. First, the study was a retrospective observational study, and it is possible that unappreciated or unmeasurable confounding variables altered the results. Second, the present study was limited to a specific geographic area; therefore, there may have been some selection bias for enrollment, which may make it difficult to apply the present study results to all MI patients in Japan. Third, the date of death due to mechanical complications was different from the date of onset because the timing of mechanical onset was not tabulated. In the RMI group, deaths due to mechanical complications continued to increase during hospitalization, but the timing of their onset was unknown. Further research is needed to determine the frequency of occurrence of mechanical complications. Fourth, the cause of death was determined by the cardiologists in each hospital from clinical diagnosis or autopsy diagnosis. However, no detailed data were collected on the method used in determining the causes of death. Finally, this study was not a comparison of disease from onset but a comparison over a very limited time period from the admission. We conducted a comparative study of the same disease using different time periods, especially for the RMI group, because it was not possible to collect data until admission. Furthermore, as there were no data on prognosis after hospital discharge, the natural history of RMI was unknown. Additional detailed nationwide observational studies with long-term follow up are needed for further evaluation.
Conclusions
The RMI patients had distinctive clinical features and sequelae compared with AMI patients, and the major cause of death of RMI patients was different from that of AMI patients. Furthermore, in RMI patients, deaths due to mechanical complications continued to increase even as hospitalization continued. Further investigation is needed to clarify the treatment strategy for RMI patients.
Acknowledgments
The authors thank all members of the Tokyo CCU Network Scientific Committee, Tokyo Fire Department, Tokyo Medical Association, and Tokyo Metropolitan Government.
Data Availability
In principle, the availability of the data used in this study is not shared.
Disclosures
Data collection and maintenance for the Tokyo CCU network registry is financially supported by the Tokyo Metropolitan Government, which had no role in the execution of this study or in the interpretation of the results.
Although R.I. is affiliated with an endowed department sponsored by Abbott Vascular Japan Co., Ltd., there is no conflict of interest regarding this paper. The Conflict of Interest management committee of Tokyo CCU Network approves that the other authors have no relationships that could be construed as a conflict of interest.
References
- 1.
Cannon CP, Gibson CM, Lambrew CT, Shoultz DA, Levy D, French WJ, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA 2000; 283: 2941–2947.
- 2.
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2015 ACC/AHA/SCAI Focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: An update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J Am Coll Cardiol 2016; 67: 1235–1250.
- 3.
Kimura K, Kimura T, Ishihara M, Nakagawa Y, Nakao K, Miyauchi K, et al; on behalf of the Japanese Circulation Society Joint Working Group. JCS 2018 guideline on diagnosis and treatment of acute coronary syndrome. Circ J 2019; 83: 1085–1196.
- 4.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Kardiol Pol 2018; 76: 229–313.
- 5.
Yamamoto T, Yoshida N, Takayama M, Tokyo CCU Network. Temporal trends in acute myocardial infarction incidence and mortality between 2006 and 2016 in Tokyo: Report from the Tokyo CCU Network. Circ J 2019; 83: 1405–1409.
- 6.
Hochman JS, Lamas GA, Buller CE, Dzavik V, Reynolds HR, Abramsky SJ, et al. Coronary intervention for persistent occlusion after myocardial infarction. N Engl J Med 2006; 355: 2395–2407.
- 7.
Ioannidis JP, Katritsis DG. Percutaneous coronary intervention for late reperfusion after myocardial infarction in stable patients. Am Heart J 2007; 154: 1065–1071.
- 8.
Erne P, Schoenenberger AW, Burckhardt D, Zuber M, Kiowski W, Buser PT, et al. Effects of percutaneous coronary interventions in silent ischemia after myocardial infarction: The SWISSI II randomized controlled trial. JAMA 2007; 297: 1985–1991.
- 9.
Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: A consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000; 36: 959–969.
- 10.
Miyachi H, Takagi A, Miyauchi K, Yamasaki M, Tanaka H, Yoshikawa M, et al. Current characteristics and management of ST elevation and non-ST elevation myocardial infarction in the Tokyo metropolitan area: From the Tokyo CCU network registered cohort. Heart Vessels 2016; 31: 1740–1751.
- 11.
Kosuge M, Kimura K, Ishikawa T, Shimizu T, Hibi K, Nozawa N, et al. Clinical implications of persistent ST segment depression after admission in patients with non-ST segment elevation acute coronary syndrome. Heart 2005; 91: 95–96.
- 12.
Kosuge M, Kimura K, Ishikawa T, Ebina T, Hibi K, Tsukahara K, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J 2006; 70: 222–226.
- 13.
Patel H, Rosengren A, Ekman I. Symptoms in acute coronary syndromes: Does sex make a difference? Am Heart J 2004; 148: 27–33.
- 14.
Maynard C, Litwin PE, Martin JS, Weaver WD. Gender differences in the treatment and outcome of acute myocardial infarction: Results from the Myocardial Infarction Triage and Intervention Registry. Arch Intern Med 1992; 152: 972–976.
- 15.
Brieger D, Eagle KA, Goodman SG, Steg PG, Budaj A, White K, et al. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: Insights from the Global Registry of Acute Coronary Events. Chest 2004; 126: 461–469.
- 16.
Malkin CJ, Prakash R, Chew DP. The impact of increased age on outcome from a strategy of early invasive management and revascularisation in patients with acute coronary syndromes: Retrospective analysis study from the ACACIA registry. BMJ Open 2012; 2: e000540.
- 17.
Toleva O, Ibrahim Q, Brass N, Sookram S, Welsh R. Treatment choices in elderly patients with ST: Elevation myocardial infarction-insights from the Vital Heart Response registry. Open Heart 2015; 2: e000235.
- 18.
Kaul P, Armstrong PW, Sookram S, Leung BK, Brass N, Welsh RC. Temporal trends in patient and treatment delay among men and women presenting with ST-elevation myocardial infarction. Am Heart J 2011; 161: 91–97.
- 19.
Diercks DB, Owen KP, Kontos MC, Blomkalns A, Chen AY, Miller C, et al. Gender differences in time to presentation for myocardial infarction before and after a national women’s cardiovascular awareness campaign: A temporal analysis from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation (CRUSADE) and the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network-Get with the Guidelines (NCDR ACTION Registry-GWTG). Am Heart J 2010; 160: 80–87.e83.
- 20.
Magalhaes P, Mateus P, Carvalho S, Leao S, Cordeiro F, Moreira JI, et al. Relationship between treatment delay and type of reperfusion therapy and mechanical complications of acute myocardial infarction. Eur Heart J Acute Cardiovasc Care 2016; 5: 468–474.
- 21.
Figueras J, Cortadellas J, Calvo F, Soler-Soler J. Relevance of delayed hospital admission on development of cardiac rupture during acute myocardial infarction: Study in 225 patients with free wall, septal or papillary muscle rupture. J Am Coll Cardiol 1998; 32: 135–139.
- 22.
Figueras J, Alcalde O, Barrabes JA, Serra V, Alguersuari J, Cortadellas J, et al. Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period. Circulation 2008; 118: 2783–2789.