Abstract
Background:
The usefulness of electrocardiographic (ECG) voltage criteria for diagnosing hypertrophic cardiomyopathy (HCM) in pediatric patients is poorly defined.
Methods and Results:
ECGs at the 1st grade (mean [±SD] age 6.6±0.3 years) were available for 11 patients diagnosed with HCM at around the 7th grade (13.2±0.3 years). ECGs were available for another 64 patients diagnosed with HCM in the 1st (n=15), 7th (n=32), and 10th (n=17) grades. Fifty-one voltage criteria were developed by grade and sex using 62,841 ECGs from the general population. Voltage criteria were set at the 99.95th percentile (1/2,000) point based on the estimated prevalence of childhood HCM (2.9 per 100,000 [1/34,483]) to decrease false negatives. Conventional criteria were from guidelines for school-aged children in Japan. Of 11 patients before diagnosis, 2 satisfied conventional criteria in 1st grade; 5 (56%) of the remaining 9 patients fulfilled 2 voltage criteria (R wave in limb-lead I [RI]+S wave in lead V3 [SV3] and R wave in lead V3 [RV3]+SV3). Robustness analysis for sensitivity showed RV3+SV3 was superior to RI+SV3. For all patients after diagnosis, RI+SV4 was the main candidate. However, conventional criteria were more useful than voltage criteria.
Conclusions:
Early HCM prediction was possible using RV3+SV3 in >50% of patients in 1st grade. Voltage criteria may help diagnose prediagnostic or early HCM, and prevent tragic accidents, although further prospective studies are required.
Hypertrophic cardiomyopathy (HCM) remains one of the major causes of sudden cardiac death (SCD) or aborted cardiac arrest (ACA) in youth.1–5
Electrocardiographic (ECG) findings overlap between HCM and athletes.6
Current recommendations for ECG interpretation are based on asymptomatic athletes aged 12–35 years.7
In contrast, the median age of patients with childhood-onset HCM was reported to be 12.2 years.3
A recommendation for ECG interpretation is required for asymptomatic children because many potential competitive or professional athletes may start sports activities before these ages. Early diagnosis and early intervention, such as lifestyle modification or the introduction of medications, may prevent children and adolescents from competitive sports-related SCD or ACA.
A standard 12-lead ECG in HCM patients shows a variable combination of left ventricular hypertrophy (LVH), ST and T wave abnormalities, and pathological Q waves.1
Of these, voltage criteria have been reported for LVH screening.8–15
However, despite interventricular hypertrophy being a characteristic feature of HCM, few studies have investigated whether single R or S waves or a combination of R and S waves can be used to detect interventricular hypertrophy in pediatric HCM patients.16
A nationwide, school-based ECG screening program for heart diseases in the 1st, 7th, and 10th graders (aged 6, 12 and 15 years, respectively) in Japan was set by law in 1994;17
the program is also been performed in 4th graders in some regions. As part of this screening program in Japan , HCM is most frequently diagnosed around the 7th grade.18
A previous study showed that approximately 60% (27/44) of school-aged children and adolescents who experienced SDS or ACA were not diagnosed with HCM before their cardiac events,19
suggesting that the current screening system may not be effective for the early diagnosis of HCM and may not allow for interventions before the appearance of symptoms.18
When participants are diagnosed with HCM at the 7th grade screening or later, the 1st grade ECGs are available for review in some areas in Japan where the ECGs of participants are digitally stored.20
The aim of the present study was to determine whether voltage criteria could be used to predict a potential diagnosis of HCM at the 1st grade screening in patients who were diagnosed at the 7th grade or later screening (i.e., approximately 6 years before the actual HCM diagnosis). Furthermore, we examined the utility of voltage criteria and conventional criteria for diagnosing HCM patients who were diagnosed at the 1st, 7th, and 10th grade screening.
Methods
Subjects
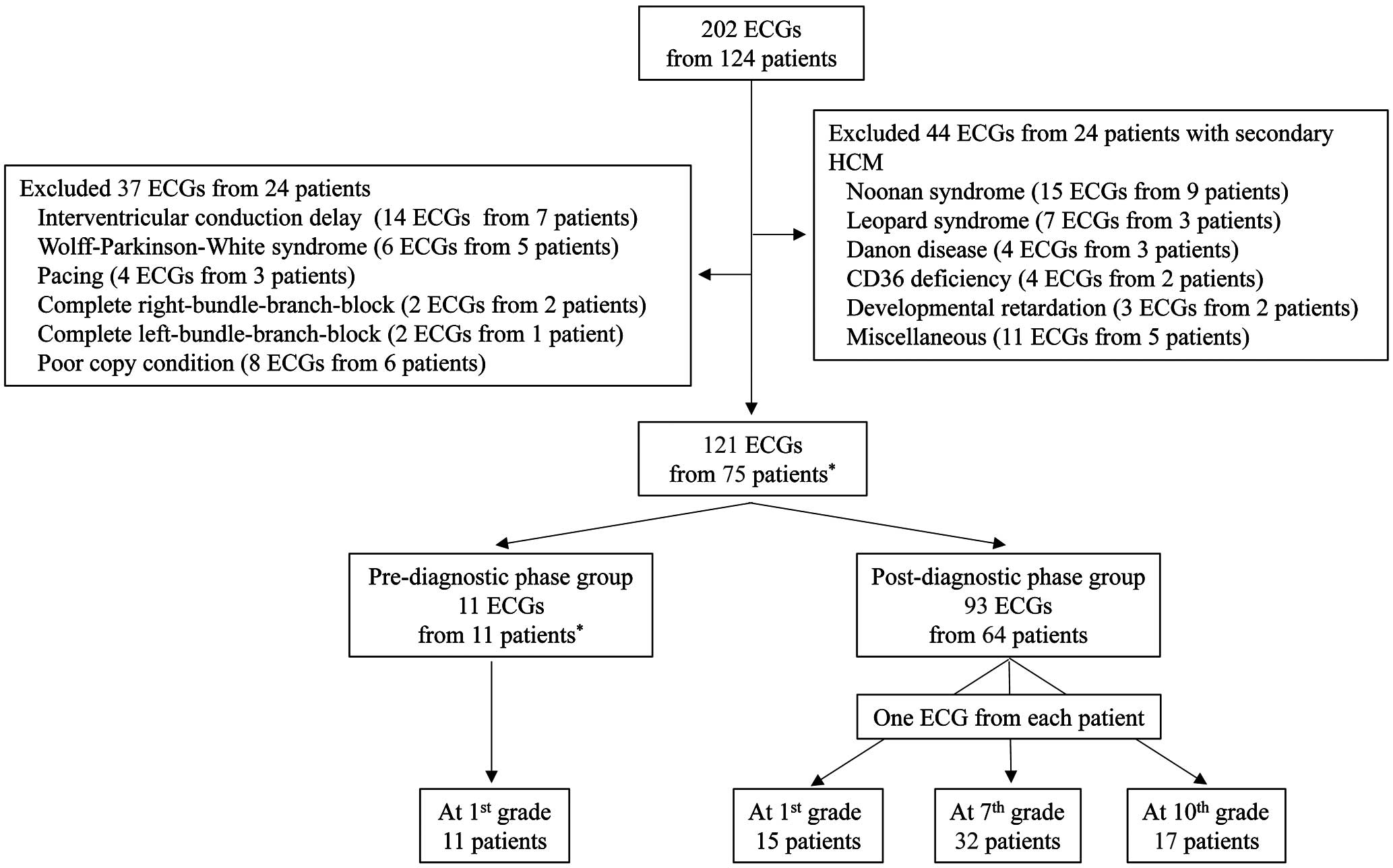
In all, 124 patients with HCM who visited 1 of 14 hospitals in Japan from 2000 to 2019 and who were <20 years old at their first visit were included in this study. Of 202 ECGs from 124 patients, 44 ECGs from 24 patients with secondary HCM and 37 ECGs from 24 patients with findings that affect the QRS voltages (i.e., complete bundle branch block) were excluded (Figure 1). Patients were divided into pre- and post-diagnostic groups.
This study was approved by the Ethics Committee of the National Hospital Organization Kagoshima Medical Center (27-9 and 27-28).
Prediagnostic Group
The prediagnostic group included 11 patients (9 boys, 2 girls) who visited the National Hospital Organization Kagoshima Medical Center and were diagnosed with HCM at a mean (±SD) age of 13.2±2.0 years and whose ECGs at the 1st grade screening program were retrospectively available (Table 1). The mean (±SD) interval between the 1st grade ECG recordings and actual diagnosis was 6.4±1.8 years. A diagnosis of HCM was made when the left ventricular (LV) wall thickness was ≥15 mm; this is a robust diagnostic criterion for adults in this group.1
Two patients with LV wall thickness <15 mm were pathologically diagnosed by myocardial biopsy (Cases 10 and 11).9
Table 1.
Characteristics of Subjects in the Prediagnostic Group
| |
Sex |
Age at
Dx |
Dx
events |
IVSThd at
Dx (mm) |
PWThd at
Dx (mm) |
Type of
HCMe |
Age at
1st ECG |
Intervala
(years) |
Prognosis |
Genes |
Variants |
| Case no. |
| 1 |
M |
11.9 |
Screening |
20.8 |
11.1 |
ASH |
6.6 |
5.3 |
Alive |
Not
identified |
|
| 2 |
M |
12.3 |
Screening |
27.0 |
10.2 |
ASH |
6.2 |
6.0 |
Sudden
death |
Not
done |
|
| 3 |
M |
13.1 |
Screening |
16.4 |
13.1 |
Diffuse |
7.0 |
6.0 |
Alive |
Not
done |
|
| 4 |
F |
16.0 |
Screening |
17.1 |
11.0 |
ASH |
6.9 |
9.1 |
Alive |
MYH7 |
c.3158G>A,
p.R1053Q,
rs587782962 |
| 5b |
F |
9.6 |
Screening |
17.2 |
6.1 |
Apicalf |
6.3 |
3.3 |
Alive |
MYH7 |
c.1357C>T,
p.R453C,
rs121913625 |
| 6b |
M |
13.0 |
Familial
study |
18.3 |
13.1 |
ASH |
6.8 |
6.2 |
Alive |
MYH7 |
c.1357C>T,
p.R453C,
rs121913625 |
| 7 |
M |
12.6 |
Screening |
15.2 |
12.0 |
Diffuse |
6.4 |
6.2 |
Alive |
MYBPC3 |
c.1484G>A,
p.R495Q,
rs200411226 |
| 8 |
M |
12.3 |
Screening |
27.5 |
9.3 |
ASH |
6.2 |
6.0 |
Alive |
Not
identified |
|
| 9 |
M |
12.9 |
Screening |
18.7 |
8.8 |
ASH |
6.9 |
6.0 |
ACA |
MYH7 |
c.2155C>T,
p.R719W,
rs121913637 |
| 10c |
M |
15.6 |
Screening |
11.9 |
11.9 |
Diffuse |
6.7 |
8.9 |
Alive |
Not
identified |
|
| 11c |
M |
16.3 |
OHCA |
14.0 |
10.0 |
ASH |
6.5 |
9.9 |
ACA |
TNNT2 |
c.418C>T,
p.R140C,
homozygous,
rs397516463 |
| Mean±SD |
|
13.2±2.0 |
|
18.6±4.9 |
10.6±2.1 |
|
6.6±0.3 |
6.4±1.8 |
|
|
|
aInterval between the age at the time of electrocardiography (ECG) in 1st grade and the age at diagnosis. bCases 5 and 6 were members of the same family. cCases 10 and 11 were diagnosed pathologically. dMeasurements of the left ventricular wall were made at the maximum point of the interventricular septum or the posterior wall. eAsymmetric septal hypertrophy was defined as a ratio of the septum to posterior wall thickness ≥1.3 according to the traditional definition,33 whereas diffuse-type septal hypertrophy was defined as a ratio <1.3. fCase 5 showed hypertrophy of the apical region (apical hypertrophy type) that extended to the distal portion of the interventricular septum and lateral portion of the left ventricle. ACA, aborted cardiac arrest; Apical, apical hypertrophy; ASH, asymmetric septal hypertrophy; Dx, diagnosis or diagnostic; F, female; IVSTh, interventricular septum thickness (in mm); M, male;
MYBP3, myosin binding protein C;
MYH7, β-myosin heavy chain; OHCA, out-of-hospital cardiac arrest; PWTh, posterior wall thickness (in mm);
TNNT2, troponin T.
The genetic background in this group was determined using the ClearSeq Halo HS cardiomyopathy panel (Agilent Technologies, Santa Clara, CA, USA), which included 34 genes, and using a bench top-type next-generation sequencing machine (MiSeq; Illumina, San Diego, CA, USA). Data were analyzed using SureCall software (Agilent Technologies). Detected variants were confirmed using the Sanger method and variants classified as pathogenic or likely pathogenic in ClinVar (https://www.ncbi.nlm.nih.gov/clinvar/) were judged as pathogenic mutations.
Post-Diagnostic Group
The post-diagnostic group included 64 patients who were already diagnosed with HCM in 1 of 14 hospitals (mean [±SD] 11.2±3.9 years;
Table 2). ECGs were obtained in the 1st, 7th, and 10th grades, and the earliest ECGs from each patient were used (Figure 1). A diagnosis of HCM was made using the 2014 European Society of Cardiology (ESC) guidelines1
as follows: wall thickness ≥15 mm or z-score >2, where the z-score is defined as the number of standard deviations from the population mean in this group. Genetic tests were not mandatory in this group.
Table 2.
Characteristics of the Post-Diagnostic Groups
| |
1st grade
(n=15) |
7th grade
(n=32) |
10th grade
(n=17) |
| No. males/females |
7/8 |
19/13 |
9/8 |
| Age at ECGa (years) |
6.7±0.6 |
12.9±0.6 |
15.8±0.7 |
| Age at diagnosis (years) |
5.2±2.4 |
12.1±1.6 |
14.6±1.6 |
| Intervalb (years) |
1.5±2.3 |
0.9±1.3 |
1.2±1.9 |
| Diagnostic events |
| At screening |
5 (33) |
25 (78) |
9 (53) |
| Through symptoms |
0 |
1 (3) |
3 (18) |
| Familial study |
4 (27) |
1 (3) |
0 |
| By chance |
6 (40) |
4 (13) |
1 (6) |
| Unknown |
0 |
1 (3) |
3 (18) |
| Age at echocardiographyc (years) |
6.7±0.5 (n=10) |
13.0±0.8 (n=23) |
16.3±2.5 (n=11) |
| IVSTh (mm) |
16.1±5.7 |
16.0±6.6 |
17.0±5.5 |
| PWTh (mm) |
7.6±1.3 |
11.4±4.7 |
13.4±5.3 |
| Prognosis |
| Alive |
15 (100) |
26 (81) |
14 (82) |
| OHCA |
0 |
3 (9) |
1d (6) |
| Transplantation |
0 |
1 (3) |
0 |
| Death |
0 |
1 (3) |
1d (6) |
| Unknown |
0 |
1 (3) |
2 (12) |
Unless indicated otherwise, data are given as the mean±SD or n (%). aAge at which electrocardiograms (ECG) used in this study were recorded. bInterval between the age at diagnosis and the age at the time of ECG recording. cAge at which echocardiography was performed in the 1st, 7th, or 10th grades. dThe same patient. IVSTh, interventricular septum thickness; OHCA, out-of-hospital cardiac arrest; PWTh, posterior wall thickness.
Estimated Prevalence of Pediatric HCM
The true prevalence of HCM in childhood is unknown. The annual occurrence of new cases of childhood HCM ranges from 0.24 to 0.47 per 100,000.21–24
The mean annual occurrence of new cases of childhood HCM (aged <20 years) between 2015 and 2019 in Japan was 0.36 per 100,000 (95% confidence interval [CI] 0.25–0.45 per 100,000),25
which corresponds with previous reports.21–24
For example, Arola et al reported a mean annual occurrence of HCM between 1980 and 1991 of 0.24 per 100,000 (95% CI 0.17–0.33 per 100,000) and a prevalence of HCM at the end of 1991 of 2.9 per 100,000 (95% CI 2.0–4.0 per 100,000).21
Thus, the prevalence of childhood HCM in Japan may be slightly higher than that reported.21
To decrease the number of false-negative results, a screening rate between 1/2,000 or 1/5,000 may be acceptable. In the present study, we used a screening rate of 1/2,000 (99.95th percentile point) of the reference population.
Reference ECGs to Establish Screening Criteria for Increased R/S Wave Voltages
To establish the screening voltage criteria, ECGs of 1st, 7th, and 10th graders among the general population who participated in screening programs were obtained.26
ECGs were recorded at school at a speed of 25 mm/s and a sampling rate of 500 Hz using a portable PC-based system (Fukuda Denshi, Tokyo, Japan). In the Japanese screening programs, where numerous ECGs of children are recorded at the same time, narrow bandwidth filters (0.5–35 Hz) were occasionally used to remove noise. Thus, we prepared 2 ECG reference values for a narrow bandwidth and a routine bandwidth (0.05–150 Hz), as detailed below.
Reference ECGs for the Narrow Bandwidth
The process used to develop the ECG reference values was previously reported.26
Briefly, 56,753 digitally stored ECGs of participants in a school-based ECG screening system in Kagoshima, Japan, were obtained. Each ECG was manually reviewed by 2 pediatric cardiologists, and only ECGs with sinus rhythm were included. ECGs of subjects with arrhythmias, ST/T changes, or inappropriate recordings were excluded. Finally, 48,401 ECGs from 16,773 1st graders (8,350 boys, 8,423 girls), 18,126 7th graders (8,943 boys, 9,183 girls), and 13,502 10th graders (6,477 boys, 7,025 girls) were selected.26
Reference Values for the Routine Bandwidth
In all, 29,605 ECGs were recorded at the schools using a portable PC-based system (Fukuda Denshi) in Kagoshima, Ehime, Kanagawa, and Tokyo in 2016 and 2017. After reviewing the ECGs using the same process as for the narrow bandwidth ECGs, a final number of 14,400 ECGs from 2,994 1st graders (1,611 boys, 1,383 girls), 3,646 7th graders (1,634 boys, 2,012 girls), and 7,758 10th graders (4,019 boys, 3,739 girls) were selected.
Screening Criteria for Increased R/S Wave Voltages
The following 51 voltage criteria were assessed as screening criteria for screening HCM patients at 1/2,000 point in the general population:
1. R/S waves of each single lead
• An R wave of each of the 12 leads (the voltages of the R and R’ waves were summed if present)
• An S wave of each of the 12 leads
2. A combination of R/S waves of different leads that have already been published
• Cornell criteria: R wave in lead aVL (RaVL)+S wave in lead V3 (SV3) [RaVL+SV3]8
(Criterion A)
• Pediatric-specific criteria (RaVL+SV2)9
• Gubner-Ungerleider criteria: R wave in lead I (RI)+S wave in lead III (SIII) [RI+SIII]10
• Lewis criteria: RI+SIII−(R wave in lead III [RIII]+S wave in lead I [SI]) [RIII+SI]11
• Sokolow-Lyon criteria: SV1+RV5 and SV1+RV612
• The deepest S wave in any lead (SD) and the S wave in lead V4 (SD+SV4)13
(Criterion B)
• RI+SV414
(Criterion C)
RaVL+SV4, SD+SV3, RI+S2, and RI+SV3 were included to compare Criteria of A, B, and C. Approximately 80% of the reference population showed the deepest S wave in lead V2. Thus, SD+SV2 was not investigated. In addition, the total 12-lead QRS voltage15
was not investigated in the present study because it is difficult to use in the clinical setting.
3. A combination of an R wave in lead V1 (RV1) and S waves in the mid-precordial leads: RV1+SV2, RV1+SV3, and RV1+SV4
In one case in the prediagnostic group, high voltage R waves in lead V1 and relatively deep S waves in the precordial leads were seen. Thus, a combination of RV1 and S waves in the precordial leads was included.
4. A combination of R/S waves in the mid-precordial leads:
• RV2+SV2, RV2+SV3, and RV2+SV4
• RV3+SV2, RV3+SV3, and RV3+SV4
• RV4+SV2, RV4+SV3, and RV4+SV4
5. A combination of S waves of different mid-precordial leads: SV2+SV3, SV2+SV4, and SV3+SV4.
Screening Criteria for Cardiovascular Disease in the School-Based Screening Program in Japan
Screening criteria in the school-based screening program in Japan are available in published form27
and on through the Japanese Circulation Society website28
and include HCM-related findings (abnormal Q waves, ST depression, and T wave inversion), right ventricular hypertrophy, and LVH. The “conventional criteria” used in the present study are those included in these guidelines. In the present study, an ECG was considered abnormal if the patient fulfilled one of the criteria of “Group A” in those guidelines.27,28
Additional Criteria for Pathological Q Waves
The deepest Q wave of leads III and V6 was less than −0.7 mV in all 3 (1st, 7th, and 10th) grades in the general population for both the narrow and routine bandwidth groups. We defined a deep Q wave greater than −0.7 mV as an abnormal Q wave.
Statistical Analysis
All data are presented as the mean±SD. Statistical analyses were performed using IBM®
SPSS®
Statistics v23.0 (IBM Japan, Tokyo, Japan). Tentative criteria for increased R/S voltages at the 99.95th percentile (1/2,000) point were calculated by grade and sex. To estimate the 99.95th percentile (1/2,000) point, the bundled PERCENYILE.EXC function in EXEL 2016®
(Microsoft Japan, Tokyo, Japan) was used if the size of a group exceeded 2,000, where the percentile of the maximum value exceeds the 99.95th percentile (2,000/2,001=0.99950025>0.9995). When the size of a group, n, was <2,000 (e.g., n=1,611), the 99.95th percentile
x
was estimated by extrapolation using the following formula:

where
pnth=n/(n+1)=1,611/1,612 (0.99938),
pn–1th=(n−1)/(n+1)=1,610/1,612 (0.99875), and
xnth
and
xn–1th
are the largest and the second largest values of the group of size n, respectively.
When the sensitivity at the 99.95th percentile (1/2,000) screening point was the same between several voltage criteria, the robustness of the sensitivity of each voltage criterion was determined using additional 1/1,500 and 1/2,500 screening points. The sensitivity of a criterion was considered to be more robust than others when the square of the distance to the ideal sensitivity and specificity (i.e., [1−sensitivity]2+[1−specificity]2) was unchanged.
Results
Tentative Screening Criteria for Increased R/S Voltage Criteria in Each Lead
Tentative criteria for the increased R/S voltages at the 99.95th percentile (1/2,000) point for the narrow and routine bands are shown in
Supplementary Table 1A
and
1B, respectively.
Patients Fulfilling the Increased Voltage Criteria
First Graders of the Prediagnostic Group
For the 11 patients in the 1st grade in the prediagnostic group, the highest sensitivity (45%) was found for the screening criteria of RI+SV3, RV2+SV3, and RV3+SV3; all these criteria included the S wave voltage in lead V3 (Supplementary Table 2). Two of these 11 patients were screened using the conventional criteria during the 1st grade screening program (QS pattern [Case 10] and right ventricular hypertrophy [Case 11]). However, they were diagnosed as normal because they did not have an increased ventricular wall thickness or congenital heart diseases on echocardiography.20
The ECGs of all 11 patients are shown in
Supplementary Figure 1. The remaining 9 patients who showed a prominent LV wall thickness that fulfilled the diagnostic criteria for adults at their 7th grade screening did not fulfill conventional criteria at their 1st grade screening. Of these 9 patients, the highest sensitivity (56%) was still found for the screening criteria of RI+SV3 and RV3+SV3. The RV3+SV3 criterion was preferable to the RI+SV3 criterion because robustness analysis showed that the sensitivity, specificity, and deviation from the ideal point of the sensitivity and specificity ([1−sensitivity]2+[1−specificity]2) of RV3+SV3 was unchanged (robust), even when the screening point changed from 1/2,000 to 1/1,500 or 1/2,500 (Table 3). Thus, the tentative criterion of RV3+SV3 for the early diagnosis of 1st graders in the clinical setting was 6.0 and 5.0 mV in boys and girls, respectively, for the narrow bandwidth group and 6.5 and 6.1 mV in boys and girls, respectively, for the routine bandwidth group (Supplementary Table 1A,1B). Nevertheless, these criteria should be further revised after obtaining a larger number of ECGs for the routine bandwidth from the general population.
Table 3.
Robustness of Sensitivity of the Voltage Criteria of R Wave in Limb-Lead I (RI)+S Wave in Lead V3 (SV3) and R Wave in Lead V3 (RV3)+SV3 at the 1/1,500, 1/2,000, and 1/2,500 Screening Points
Screening
point |
RI+SV3 |
RV3+SV3 |
| Sensitivity |
Specificity |
Value |
Sensitivity |
Specificity |
Value |
| 1/1,500 |
0.5556 |
0.9993 |
0.1975 |
0.5556 |
0.9993 |
0.1975 |
| 1/2,000 |
0.5556 |
0.9995 |
0.1975 |
0.5556 |
0.9995 |
0.1975 |
| 1/2,500 |
0.4444 |
0.9996 |
0.3087 |
0.5556 |
0.9996 |
0.1975 |
Value refers to the square of the distance to the ideal sensitivity and specificity (i.e., [1−sensitivity]2+[1−specificity]2), with smaller values indicating a better candidate criterion.
First Graders of the Post-Diagnostic Group
Of the 15 patients in the 1st grade in the post-diagnostic group, the highest sensitivity (60%) was found for SV2+SV4, whereas the criteria with the second-highest (53%) sensitivity were RaVL+SV3, SD+SV3, RI+SV3, RI+SV4, and SV2+SV3 (Supplementary Table 3). In the post-diagnostic group, 10 of 15 patients (67%) met conventional criteria. Of remaining 5 patients who did not meet conventional criteria, 4 were diagnosed by chance (Supplementary Table 3). RaVL+SV3, SD+SV3, RI+SV3, RI+SV4, SV2+SV3, and SV2+SV4, which included the S wave voltages in leads V3 or V4 (SV3 or SV4, respectively), had a sensitivity of 60%. These 6 screening criteria had the same sensitivity at 1/1,500 and 1/2,500 (data not shown), suggesting that they are all candidate criteria for screening 1st graders in the post-diagnostic group who do not meet conventional criteria.
Seventh Graders of the Post-Diagnostic Group
The highest sensitivity was found for RI+SV4 (44%;
Table 4). Of the 32 patients in this group, 29 (91%) fulfilled the conventional criteria. Of the 3 remaining patients who did not meet the conventional criteria, 2 fulfilled the voltage criterion of RI+SV4. However, of these 3 patients, 2 showed a flat T wave (and not an inverted T wave as in the conventional criteria) in the left precordial leads and 1 showed a very low voltage R wave in the left precordial leads. Overall, these findings suggest that nearly all 7th graders with HCM may be screened using conventional criteria and abnormal findings.
Table 4.
Number of Patients Who Fulfilled the Criteria and the Sensitivity of All Surrogate Markers in the Pre- and Post-Diagnostic Groups
| |
Pre-diagnostic phase |
Post-diagnostic phase |
1st grade
(n=11) |
1st grade
(n=15) |
7th grade
(n=32) |
10th grade
(n=17) |
| RI |
0 (0) |
2 (13) |
12 (38) |
1 (6) |
| RII |
0 (0) |
3 (20) |
2 (6) |
3 (18) |
| RIII |
0 (0) |
1 (7) |
1 (3) |
3 (18) |
| RaVR |
0 (0) |
5 (33) |
2 (6) |
4 (24) |
| RaVL |
0 (0) |
2 (13) |
9 (28) |
3 (18) |
| RaVF |
0 (0) |
1 (7) |
1 (3) |
3 (18) |
| RV1 |
2 (18) |
2 (13) |
8 (25) |
1 (6) |
| RV2 |
1 (9) |
2 (13) |
6 (19) |
2 (12) |
| RV3 |
0 (0) |
1 (7) |
1 (3) |
2 (12) |
| RV4 |
0 (0) |
1 (7) |
1 (3) |
0 (0) |
| RV5 |
0 (0) |
2 (13) |
2 (6) |
0 (0) |
| RV6 |
0 (0) |
1 (7) |
2 (6) |
0 (0) |
| SI |
0 (0) |
3 (20) |
3 (9) |
2 (12) |
| SII |
0 (0) |
3 (20) |
1 (3) |
4 (24) |
| SIII |
0 (0) |
3 (20) |
6 (19) |
4 (24) |
| SaVR |
0 (0) |
3 (20) |
5 (16) |
2 (12) |
| SaVL |
0 (0) |
0 (0) |
0 (0) |
3 (18) |
| SaVF |
0 (0) |
3 (20) |
4 (13) |
4 (24) |
| SV1 |
0 (0) |
1 (7) |
1 (3) |
0 (0) |
| SV2 |
2 (18) |
4 (27) |
1 (3) |
1 (6) |
| SV3 |
4 (36) |
7 (47) |
1 (3) |
2 (12) |
| SV4 |
0 (0) |
7 (47) |
3 (9) |
2 (12) |
| SV5 |
1 (9) |
5 (33) |
4 (13) |
3 (18) |
| SV6 |
0 (0) |
5 (33) |
2 (6) |
3 (18) |
| RaVL+SV2 |
3 (27) |
6 (40) |
5 (16) |
2 (12) |
| RaVL+SV3 |
4 (36) |
8 (53) |
4 (13) |
5 (29) |
| RaVL+SV4 |
1 (9) |
7 (47) |
11 (34) |
5 (29) |
| RI+SIII |
0 (0) |
3 (20) |
11 (34) |
4 (24) |
| Lewis |
0 (0) |
3 (20) |
6 (19) |
3 (18) |
| SV1+RV5 |
0 (0) |
2 (13) |
3 (9) |
0 (0) |
| SV1+RV6 |
1 (9) |
1 (7) |
1 (3) |
0 (0) |
| SD+SV3 |
4 (36) |
8 (53) |
2 (6) |
3 (18) |
| SD+SV4 |
4 (36) |
7 (47) |
2 (6) |
2 (12) |
| RI+SV2 |
2 (18) |
7 (47) |
3 (9) |
1 (6) |
| RI+SV3 |
5 (45) |
8 (53) |
5 (16) |
4 (24) |
| RI+SV4 |
1 (9) |
8 (53) |
14 (44) |
6 (35) |
| RV1+SV2 |
1 (9) |
1 (7) |
3 (9) |
2 (12) |
| RV1+SV3 |
3 (27) |
4 (27) |
2 (6) |
3 (18) |
| RV1+SV4 |
3 (27) |
7 (47) |
11 (34) |
3 (18) |
| RV2+SV2 |
1 (9) |
2 (13) |
4 (13) |
3 (18) |
| RV2+SV3 |
5 (45) |
2 (13) |
4 (13) |
3 (18) |
| RV2+SV4 |
2 (18) |
6 (40) |
9 (28) |
4 (24) |
| RV3+SV2 |
2 (18) |
3 (20) |
2 (6) |
1 (6) |
| RV3+SV3 |
5 (45) |
4 (27) |
3 (9) |
2 (12) |
| RV3+SV4 |
1 (9) |
5 (33) |
6 (19) |
3 (18) |
| RV4+SV2 |
1 (9) |
4 (27) |
2 (6) |
0 (0) |
| RV4+SV3 |
3 (27) |
5 (33) |
2 (6) |
0 (0) |
| RV4+SV4 |
1 (9) |
6 (40) |
7 (22) |
1 (6) |
| SV2+SV3 |
3 (27) |
8 (53) |
1 (3) |
3 (18) |
| SV2+SV4 |
2 (18) |
9 (60) |
2 (6) |
3 (18) |
| SV3+SV4 |
4 (36) |
7 (47) |
3 (9) |
2 (12) |
| HCM-related |
1 (9) |
9 (60) |
27 (84) |
13 (76) |
| Abnormal Q |
1 (9) |
3 (20) |
8 (25) |
1 (6) |
| ST depression |
0 (0) |
4 (27) |
12 (38) |
5 (29) |
| T wave inversion |
0 (0) |
5 (33) |
19 (59) |
12 (71) |
| RVH |
1 (9) |
1 (7) |
2 (6) |
1 (6) |
| Conventional criteria |
2 (18) |
10 (67) |
29 (91) |
14 (82) |
Data show the number of patients with the sensitivity (%) of each marker given in parentheses. HCM, hypertrophic cardiomyopathy; RVH, right ventricular hypertrophy.
Tenth Graders of the Post-Diagnostic Group
The highest sensitivity was found for RI+SV4, although the sensitivity was low (35%;
Table 4). Of the 17 patients, 14 (82%) fulfilled the conventional criteria, whereas the remaining 3 patients also had a flat T wave in lead V6, a deep S wave (1.3 mV) in lead V6, and fulfilled the voltage criteria of RV2+SV2 and RV3+SV3.
Candidate Criteria for 1st, 7th, and 10th Graders in the Post-Diagnostic Groups
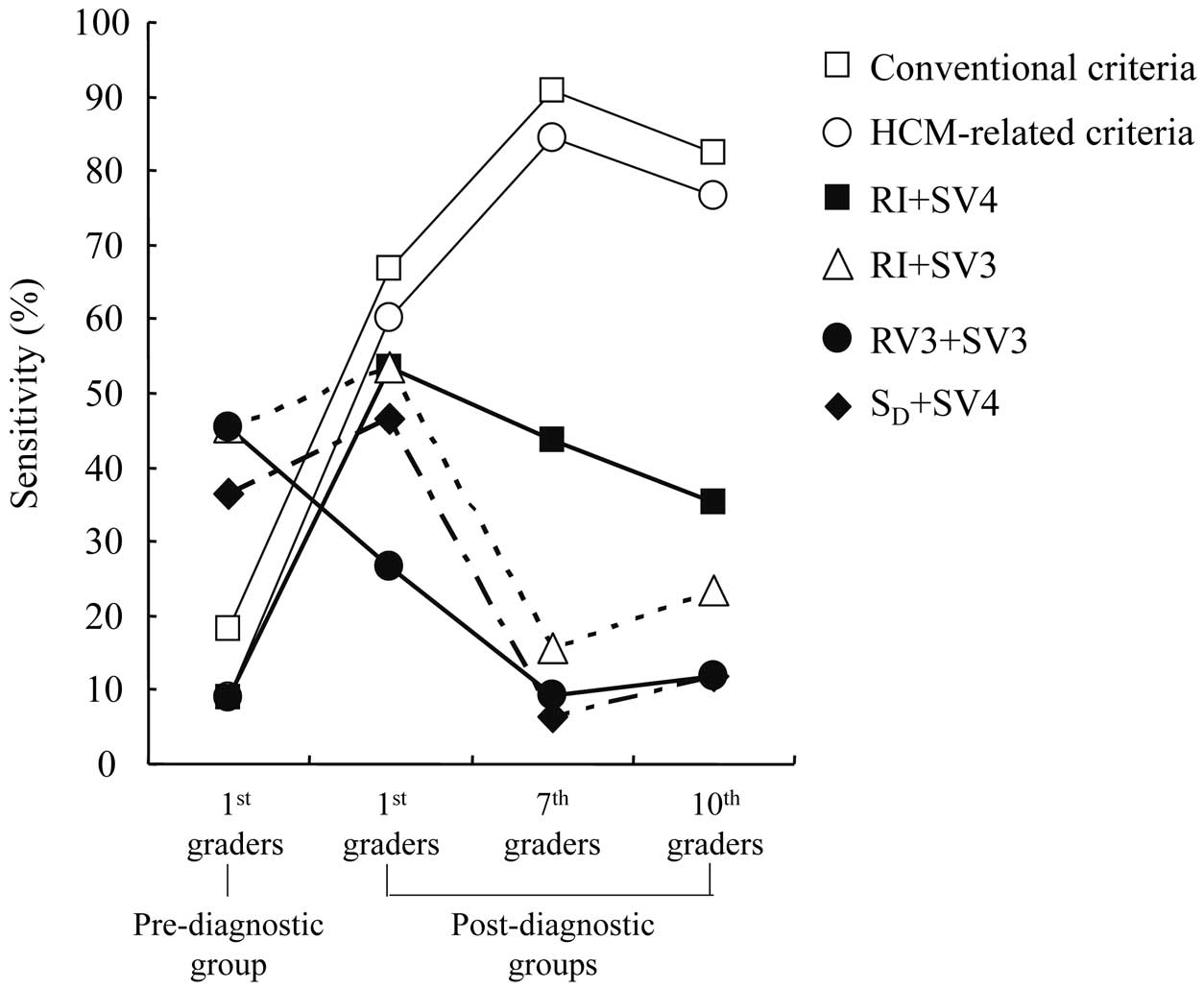
The sensitivity of representative voltage criteria for the pre- and post-diagnostic groups, including subjects who fulfilled the conventional screening criteria, is shown in
Figure 2. RI+SV4 was a potential candidate criterion for all post-diagnostic groups because it had one of the highest sensitivities in 1st graders who did not meet conventional criteria, and showed the highest sensitivity in 7th and 10th graders. However, conventional diagnostic criteria were better at diagnosing patients with HCM than the voltage criteria, particularly in the case of 7th and 10th graders (Figure 2; Table 4). The tentative criterion of RI+SV4 for 1st graders in the clinical setting was 3.2 and 3.0 mV for boys and girls, respectively, and 3.6 mV for both boys and girls with a routine bandwidth (Supplementary Table 1). Nevertheless, these criteria should be further revised after obtaining a larger number of ECGs for the routine bandwidth from the general population.
A summary of the sensitivity of each criterion is presented in
Table 4. The specificity of each criterion was approximately 99.95% for all screening criteria because the criteria were set to screen 1/2,000 of the general population.
Discussion
The present study showed that early prediction of a potential diagnosis of HCM was possible using the voltage criteria of RI+SV3 and RV3+SV3 in >50% of patients in the 1st grade who were diagnosed in the 7th grade. The robustness of sensitivity data showed that RV3+SV3 was superior to RI+SV3. This strategy may help prevent tragic accidents in patients, although future prospective studies are required. RI+SV4 was also useful for diagnosing patients with HCM in the post-diagnostic groups. The present study showed that the voltage criteria had a lower sensitivity for screening patients with HCM than the conventional criteria for post-diagnostic groups, particularly for 7th and 10th graders.
ECG findings in HCM patients are known to precede echocardiographic findings.20,29,30
Early diagnosis via ECG may prevent children and adolescents from competitive sports-related SCD or ACA. One strategy may be to compare ECG findings between normal controls and patients with positive pathogenic variants without overt LVH using imaging techniques such as echocardiography.30–32
A limitation of this strategy is the low penetrance of HCM during childhood.31,32
Previous studies in children with positive mutations reported that 2 (17%) of 12 children (12±5 years old)31
and 8 (7%) of 119 children (12±3 years old)32
developed overt HCM during follow-up.
In the present study we used a unique strategy of retrospectively examining ECGs approximately 6 years before the actual HCM diagnosis to determine whether they fulfilled our voltage criteria. We used the 99.95th percentile (1:2,000) point as the voltage criterion for screening criteria, indicating that specificity was approximately 99.95% for all screening criteria. This strategy showed that 2 screening criteria (RI+SV3 and RV3+SV3) could predict a potential diagnosis of HCM in 5 of 9 patients (56% sensitivity) in the prediagnostic group. These patients did not fulfill the conventional criteria while in 1st grade, but showed a prominent LV wall thickness approximately 6 years later, suggesting that screening with voltage criteria is a useful strategy for the early screening of patients at risk of future marked LVH, although the efficacy was not optimal.
Both criteria included the SV3 (Supplementary Table 2). Of the 5 first graders in the post-diagnostic group who did not fulfill the conventional criteria, 3 fulfilled the voltage criteria that included SV3 or SV4 (Supplementary Table 3). In 7th and 10th graders in the post-diagnostic group, the highest sensitivity (44%) was found for RI+SV4, although nearly all patients met conventional criteria or had some abnormal findings. Our data suggest that the efficacy of the deep S wave in the mid-precordial leads shifts from V3 to V4 with age and/or with the development of HCM phenotypes. Our findings are consistent with reports that SD+SV413
or RI+SV414
were the most effective screening criteria for adult patients with LVH, both of which include SV4.
With regard to the effect of the R wave voltage, the voltage criterion of RV3+SV3 (effective for the prediagnostic group) showed a low sensitivity (20%) for patients who did not meet conventional criteria in 1st grade in the post-diagnostic group. Rather, the combined voltage criteria, including the R wave voltage in leads aVL or I, showed high sensitivity (Table 4). These findings are consistent with previous studies in adults showing the importance of the R wave in leads aVL7
or I,10,11,14
suggesting that the R wave vector progresses leftward and slightly upward of the frontal plane with age and/or phenotypic LVH progression.
The voltage criteria had a lower sensitivity for screening children and adolescents with HCM than the conventional criteria for the post-diagnostic groups. A potential reason for this is that the ECG may change with the development of the HCM phenotype. The QRS voltages of children and adolescents with HCM (Supplementary Figure 2), as well as those in the general population,24
increase with age, particularly in males. Nevertheless, only a small number of patients showed a constant increase in the QRS. Furthermore, many patients will develop HCM-related ECG abnormalities rather than an increase in QRS voltages after developing the HCM phenotype and pathological changes.
The present study showed that the voltage criterion of RV3+SV3 is effective in predicting a potential diagnosis of HCM in the 1st grade for the prediagnostic group. For the 1st grader’s post-diagnostic group, 6 screening criteria, including RI+SV4, were candidates for screening 1st graders who did not meet conventional criteria. In the 7th and 10th grade screening programs, the conventional criteria may be sufficient, but the voltage criterion of RI+SV4 may be applicable in the 7th grade screening program because 14 of 32 (44%) patients in the 7th grade post-diagnostic group (Figure 2;
Table 4) and 2 of 3 (67%) patients who did not fulfill the conventional criteria in the 7th grade post-diagnostic group fulfilled the criterion of RI+SV4. These data indicate that the voltage criteria of RV3+SV3 and RI+SV4 could be included in the 1st grade screening program and that the voltage criterion of RI+SV4 may be applicable to the 7th grade screening program.
This study has some limitations. First, the number of patients in the prediagnosis group was very small. Nevertheless, this is the first report examining the ECGs of patients 6 years before a diagnosis of HCM. Furthermore, our strategy was able to detect 5 of 9 patients (56%) with increased QRS voltages who did not meet conventional criteria. If we expand the number of patients using this strategy, the early diagnosis of HCM before the development of a phenotype may be possible. Second, we only presented tentative voltage criteria. QRS voltages have been reported to differ between races and/or studies.19
Thus, future studies are required to develop the exact diagnostic voltage criteria for different races and/or ethnicities based on ECGs from their general populations. Third, the number of reference ECGs for the routine bandwidth was relatively small compared with that for the narrow bandwidth. This should be expanded in future studies. Finally, we did not discuss approaches to minimize the concerns of patients and families regarding the potential for developing HCM in the future. Further studies are required to confirm the sensitivity and specificity of our voltage criteria to provide sufficient information to minimize their concerns and develop requirements for follow-up.
In conclusion, early prediction of a potential diagnosis of HCM was possible using the voltage criterion of RV3+SV3 in >50% of patients in the 1st grade who were diagnosed in the 7th grade. This strategy may help prevent competitive activities-associated tragic accidents in these patients, although further prospective studies are required. For example, patients should be followed-up every few years, with the interval based on their ECG and echocardiography findings. Finally, the conventional criteria for HCM or abnormal findings can diagnose nearly all patients in the 7th and 10th grades.
Acknowledgments
The authors thank Edanz Group (https://en-author-services.edanz.com/ac) for editing a draft of this manuscript.
Sources of Funding
This work was supported by Health and Labour Sciences Research Grants from the Japanese Ministry of Health, Labour, and Welfare (Comprehensive Research on Cardiovascular Diseases; H27-019, H29-034, and 20FC1051) and grants from the Suzuken Memorial Foundation.
Disclosures
H. Tsutsui is a member of
Circulation Journal’s Editorial Team. The remaining authors have no conflicts of interest to declare.
IRB Information
This study was approved by the Ethics Committee of the National Hospital Organization Kagoshima Medical Center (27-9 and 27-28).
Supplementary Files
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-21-0376
References
- 1.
Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy. Eur Heart J 2014; 35: 2733–2779.
- 2.
Maron BJ, Ommen SR, Semsarian C, Spirito P, Olivotto I, Maron MS. Hypertrophic cardiomyopathy: Present and future, with translation into contemporary cardiovascular medicine. J Am Coll Cardiol 2014; 64: 83–99.
- 3.
Norrish G, Cantarutti N, Pissaridou E, Ridout DA, Limongelli G, Elliott PM, et al. Risk factors for sudden cardiac death in childhood hypertrophic cardiomyopathy: A systematic review and meta-analysis. Eur J Prev Cardiol 2017; 24: 1220–1230.
- 4.
Maurizi N, Passantino S, Spaziani G, Girolami F, Arretini A, Targetti M, et al. Long-term outcomes of pediatric-onset hypertrophic cardiomyopathy and age-specific risk factors for lethal arrhythmic events. JAMA Cardiol 2018; 3: 520–525.
- 5.
Kitaoka H, Tsutsui H, Kubo T, Ide T, Chikamori T, Fukuda K, et al; on behalf of the Japanese Circulation Society Joint Working Group. JCS/JHFS 2018 guideline on the diagnosis and treatment of cardiomyopathies. Circ J 2021; 85: 1590–1689.
- 6.
Zorzi A, Calore C, Vio R, Pelliccia A, Corrado D. Accuracy of the ECG for differential diagnosis between hypertrophic cardiomyopathy and athlete’s heart: Comparison between the European Society of Cardiology (2010) and international (2017) criteria. Br J Sports Med 2018; 52: 667–673.
- 7.
Sharma S, Drezner JA, Baggish A, Papadakis M, Wilson MG, Prutkin JM, et al. International recommendations for electrocardiographic interpretation in athletes. Eur Heart J 2018; 39: 1466–1480.
- 8.
Casale PN, Devereux RB, Kligfield P, Eisenberg RR, Miller DH, Chaudhary BS, et al. Electrocadiographic detection of left ventricular hypertrophy: Development and prospective validation of improved criteria. J Am Coll Cardiol 1985; 6: 572–580.
- 9.
Brothers MB, Oster ME, Ehrlich A, Strieper MJ, Mahle WT. Novel electrocardiographic screening criterion for hypertrophic cardiomyopathy in children. Am J Cardiol 2014; 113: 1246–1249.
- 10.
Gubner R, Ungerleider HE. Electrocardiographic criteria of left ventricular hypertrophy. Arch Intern Med 1943; 72: 196–209.
- 11.
Lewis T. Observations upon ventricular hypertrophy with special reference to one or other chamber. Heart 1914; 5: 367–403.
- 12.
Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 1949; 37: 161–186.
- 13.
Peguero JG, Lo Presti S, Perez J, Issa O, Brenes JC, Tolentino A. Electrocardiographic criteria for the diagnosis of left ventricular hypertrophy. J Am Coll Cardiol 2017; 69: 1694–1703.
- 14.
Narita M, Yamada M, Tsushima M, Kudo N, Kato T, Yokono Y, et al. Novel electrocardiographic criteria for the diagnosis of left ventricular hypertrophy in the Japanese general population. Int Heart J 2019; 60: 679–687.
- 15.
Dollar AL, W C Roberts WC. Usefulness of total 12-lead QRS voltage compared with other criteria for determining left ventricular hypertrophy in hypertrophic cardiomyopathy: Analysis of 57 patients studied at necropsy. Am J Med 1989; 87: 377–381.
- 16.
Erice B, Romero C, Andériz M, Gorostiaga E, Izquierdo M, Ibáñez J. Diagnostic value of different electrocardiographic voltage criteria for hypertrophic cardiomyopathy in young people. Scand J Med Sci Sports 2009; 19: 356–363.
- 17.
Yoshinaga M, Kucho Y, Nishibatake M, Ogata H, Nomura Y. Probability of diagnosing long QT syndrome in children and adolescents according to the criteria of the HRS/EHRA/APHRS expert consensus statement. Eur Heart J 2016; 37: 2490–2497.
- 18.
Yoshinaga M. Study on the characteristics and prognosis of childhood hypertrophic cardiomyopathy. In Report to the Grand by the Ministry of Health, Labour, and Welfare [H27-019]. [in Japanese] https://mhlw-grants.niph.go.jp/niph/search/NIDD00.do?resrchNum=201711005B (accessed on October 8, 2020).
- 19.
Abe Y, Ayusawa M, Kato M, Watanabe H, Cho A, Komori A, et al. Sudden death in schoolchildren: A retrospective study on hypertrophic cardiomyopathy and cardiac events occurring under school supervision. J Pediatr Cardiol Cardiac Surg 2018; 2: 60–67.
- 20.
Seki S, Yamashita E, Tanoue K, Nuruki N, Sonoda M, Ohno S, et al. Prediagnostic electrocardiographic and echocardiographic findings of biopsy-proven hypertrophic cardiomyopathy. J Arrhythm 2018; 34: 643–646.
- 21.
Arola A, Jokinen E, Ruuskanen O, Saraste M, Pesonen E, Kuusela AL, et al. Epidemiology of idiopathic cardiomyopathies in children and adolescents: A nationwide study in Finland. Am J Epidemiol 1997; 146: 385–393.
- 22.
Nugent AW, Daubeney PE, Chondros P, Carlin JB, Cheung M, Wilkinson LC, et al. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med 2003; 348: 1639–1646.
- 23.
Lipshultz SE, Sleeper LA, Towbin JA, Lowe AM, Orav EJ, Cox GF, et al. The incidence of pediatric cardiomyopathy in two regions of the United States. N Engl J Med 2003; 348: 1647–1655.
- 24.
Colan SD, Lipshultz SE, Lowe AM, Sleeper LA, Messere J, Cox GF, et al. Epidemiology and cause-specific outcome of hypertrophic cardiomyopathy in children: Findings from the Pediatric Cardiomyopathy Registry. Circulation 2007; 115: 773–781.
- 25.
Japanese Society of Pediatric Cardiology and Pediatric Surgery. Rare disease surveillance from 2015 to 2019. http://jspccs.jp/wp-content/uploads/rare_disease_surveillance_2015.pdf, http://jspccs.jp/wp-content/uploads/rare_disease_surveillance_2016_rev181201.pdf, http://jspccs.jp/wp-content/uploads/rare_disease_surveillance_2017_rev1901.pdf, http://jspccs.jp/wp-content/uploads/rare_disease_surveillance_2018.pdf, http://jspccs.jp/wp-content/uploads/rare_disease_surveillance_2019.pdf (accessed March 30, 2021).
- 26.
Yoshinaga M, Iwamoto M, Horigome H, Sumitomo N, Ushinohama H, Izumida N, et al. Standard values and characteristics of electrocardiographic findings in children and adolescents. Circ J 2018; 82: 831–839.
- 27.
Sumitomo N, Baba R, Doi S, Higaki T, Horigome H, Ichida F, et al; on behalf of the Japanese Circulation Society and the Japanese Society of Pediatric Cardiology and Cardiac Surgery of Joint Working Group. Guidelines for heart disease screening in schools (JCS 2016/JSPCCS 2016): Digest version. Circ J 2018; 82: 2385–2444.
- 28.
JCS Guidelines. Guidelines for heart disease screening in schools (JCS 2016/JSPCCS 2016): Digest version. https://www.jstage.jst.go.jp/article/circj/82/9/82_CJ-66-0153/_article/-char/en (accessed on April 3, 2021).
- 29.
Panza JA, Maron BJ. Relation of electrocardiographic abnormalities to evolving left ventricular hypertrophy in hypertrophic cardiomyopathy during childhood. Am J Cardiol 1989; 63: 1258–1265.
- 30.
Lakdawala NK, Thune JJ, Maron BJ, Cirino AL, Havndrup O, Bundgaard H, et al. Electrocardiographic features of sarcomere mutation carriers with and without clinically overt hypertrophic cardiomyopathy. Am J Cardiol 2011; 108: 1606–1613.
- 31.
Jensen MK, Havndrup O, Christiansen M, Andersen PS, Diness B, Axelsson A, et al. Penetrance of hypertrophic cardiomyopathy in children and adolescents: A 12-year follow-up study of clinical screening and predictive genetic testing. Circulation 2013; 127: 48–54.
- 32.
Vermeer AMC, Clur SB, Blom NA, Wilde AAM, Christiaans I. Penetrance of hypertrophic cardiomyopathy in children who are mutation positive. J Pediatr 2017; 188: 91–95.
- 33.
Armstrong WF, Ryan TR. Hypertrophic and other cardiomyopathies. In: Armstrong WF, Ryan TR, editors. Feigenbaum’s echocardiography, 8th edn. Philadelphia: Wolters Kluwer, 2019; 518–543.