A 77-year-old man presented to hospital with severe mitral regurgitation (MR). Transthoracic echocardiography showed P2 prolapse, and a partial prolapse of P3 was also suspected. Transesophageal echocardiography (TEE) for detailed evaluation was attempted but abandoned because of difficulty of insertion into the esophagus. Alternatively, ECG-gated enhanced computed tomography (CT) scan was performed. CT images after motion artifact correction with SnapShot Freeze 2 (GE Healthcare, Milwaukee, WI, USA) in mid-systole (20% of the R-R interval) showed a severe prolapse of the P2 lateral portion with flail leaflet and a mild prolapse of the P2 medial portion (Figure A), and also revealed prominent chordae in the P2 medial portion, which could affect intervention for the leaflets (Figure B–D). Considering the patient’s reduced pulmonary function, we opted to perform transcatheter edge-to-edge mitral valve repair (TEER) using the MitraClip system (Abbott Vascular, Lake Bluff, ILL, USA). Intraprocedural TEE showed the MR jet mainly originated from the major prolapse of the P2 lateral portion with flail leaflet, which corresponded with the CT findings. A single XTW clip was successfully implanted at the lateral portion of A2-P2, resulting in residual mild MR (Figure E,F).
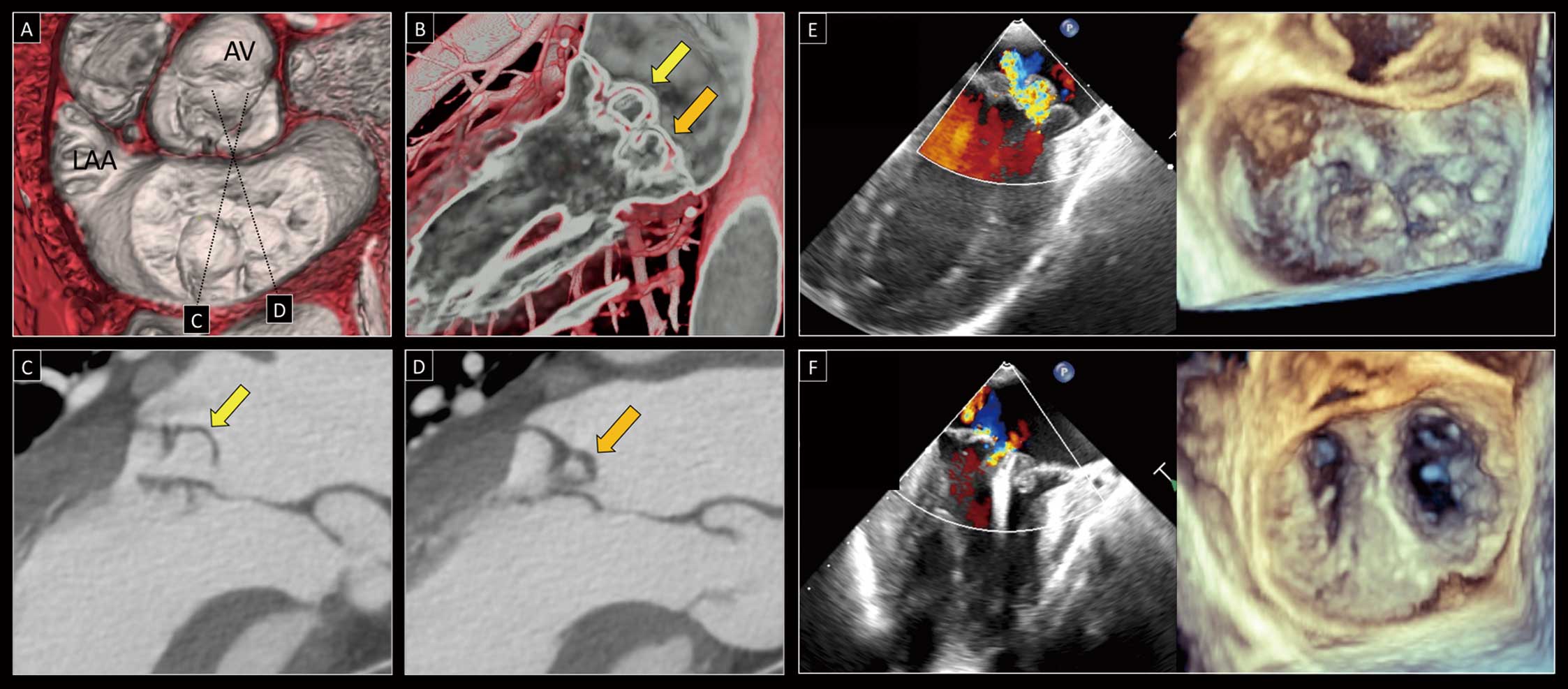
ECG-gated enhanced CT may be useful for preprocedural planning of TEER strategy in cases of inability to perform preprocedural TEE.
Conflict of Interest / Sources of Funding / IRB Iformation
None.
