Abstract
Background: The applicability of the Stages of Change model for cardiovascular disease-related behaviors, such as smoking, exercise, diet, and sleep quality, is unclear.
Methods and Results: Using a large-scale epidemiological dataset, we found that baseline behavior change intention, as per the transtheoretical model, was associated with modifications of unhealthy lifestyles including cigarette smoking, physical inactivity, skipping breakfast, and poor sleep quality.
Conclusions: Our results suggest that an individual’s motivation to change assessed by a general questionnaire may contribute to lifestyle modification and potentially prevent subsequent cardiovascular disease.
Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality worldwide, underscoring the pressing need for effective strategies to promote cardiovascular health.1 Among such strategies, adopting healthy lifestyle behaviors, such as maintaining a healthy diet, engaging in physical activity, avoiding smoking/nicotine, and practicing good sleep hygiene, are considered pivotal.2 Given the historical recognition of the importance of behavior change in promoting cardiovascular health, the Stages of Change model, also known as the Transtheoretical Model, has garnered widespread attention as a framework for facilitating the adoption and maintenance of healthy behaviors, especially in the field of smoking cessation. This model posits that individuals progress through 5 stages of behavior change (viz. precontemplation, contemplation, preparation, action, and maintenance) as they strive to adopt and maintain desired health behaviors.3,4 Surprisingly, only a small number of studies have assessed how much the baseline stages of change can predict future behavior in the clinical setting.3,5,6 In Japan, under the supervision of The Ministry of Health, Labour and Welfare, the Stage of Change model is assessed by “standard questionnaire” for every participant who undergoes a routine health checkup,7 which presents a unique opportunity to evaluate the impact of baseline stage of change on future cardiovascular healthy behaviors.
Methods
Study Design
This was a retrospective observational analysis using data from the JMDC Claims Database (JMDC, Tokyo, Japan), which is a health claims database in Japan, between 2005 and 2021.8 The JMDC Claims Database includes individual health insurance claims data from >60 insurers. The JMDC Claims Database includes workplace employees’ annual health checkup data, including demographics, medical history, medications, and hospital claims with International Classification of Diseases, 10the Revision (ICD-10) coding.
Definition
Taking into account recent research on healthy behaviors that affect cardiovascular health, we chose and defined 4 key behaviors (abstaining from smoking, engaging in regular physical activity, maintaining a healthy diet, and achieving good sleep quality) to align with our database definitions2: avoidance of nicotine as nonsmoking; physical activity as 30-min exercise ≥twice per week, or ≥1 h walk per day; healthy sleep as good rest with sleep; healthy diet as skipping breakfast <3 times per week, which were validated in our previous study.9
Study Population
We analyzed people with unhealthy behavior separately; smoking habit (n=365,259, median age 45 years; 309,667 [84.8%] men), physical inactivity (n=759,272, median age 45 years; 474,305 [62.5%] men), skipping breakfast (n=314,999, median age 42 years; 229,542 [72.9%] men), and poor sleep quality (n=557,898, median age 45 years; 341,995 [61.3%] men) at the initial health checkup (Table 1). We excluded individuals with a prior history of CVD or renal replacement therapy (n=64,481).
Table 1. Baseline Characteristics of Each Behavior Population
| |
Smoking
(n=365,259) |
Physical inactivity
(n=759,272) |
Skipping breakfast
(n=314,999) |
Poor sleep quality
(n=557,898) |
| Age, years |
45 (39–52) |
45 (40–52) |
42 (35–48) |
45 (39–52) |
| Female, n (%) |
55,592 (15.2) |
284,967 (37.5) |
85,457 (27.1) |
215,903 (38.7) |
| BMI, kg/m2 |
22.9 (20.8–25.4) |
22.6 (20.4–25.1) |
22.6 (20.5–25.2) |
22.5 (20.3–25) |
| Obesity, n (%) |
103,911 (28.4) |
196,729 (25.9) |
84,460 (26.8) |
142,876 (25.6) |
| Hypertension, n (%) |
67,848 (18.6) |
139,628 (18.4) |
49,012 (15.6) |
96,366 (17.3) |
| Diabetes, n (%) |
19,688 (5.4) |
31,901 (4.2) |
10,714 (3.4) |
22,806 (4.1) |
| Dyslipidemia, n (%) |
170,943 (46.8) |
321,776 (42.4) |
132,760 (42.1) |
223,593 (40.1) |
| Alcohol consumption, n (%) |
134,139 (36.7) |
185,163 (24.4) |
89,104 (28.3) |
125,644 (22.5) |
| Smoking, n (%) |
365,259 (100) |
207,336 (27.3) |
138,878 (44.1) |
152,319 (27.3) |
| Skipping breakfast, n (%) |
138,878 (38.0) |
180,065 (23.7) |
314,999 (100) |
143,932 (25.8) |
| Physical inactivity, n (%) |
207,336 (56.8) |
759,272 (100) |
180,065 (57.2) |
337,017 (60.4) |
| Poor sleep quality, n (%) |
152,319 (41.7) |
337,017 (44.4) |
143,932 (45.7) |
557,898 (100) |
| SBP, mmHg |
119 (109–129) |
118 (108–128) |
118 (108–128) |
117 (107–128) |
| DBP, mmHg |
74 (66–82) |
73 (66–82) |
73 (66–81) |
73 (65–81) |
| Blood sugar, mg/dL |
92 (86–100) |
92 (86–99) |
92 (86–99) |
92 (86–98) |
| Baseline stage of change, n (%) |
| Precontemplation |
110,448 (30.2) |
192,318 (25.3) |
81,225 (25.8) |
127,989 (22.9) |
| Contemplation |
140,725 (38.5) |
330,525 (43.5) |
132,967 (42.2) |
232,972 (41.8) |
| Preparation |
51,567 (14.1) |
122,930 (16.2) |
50,262 (16.0) |
88,111 (15.8) |
| Action |
29,887 (8.2) |
65,443 (8.6) |
27,870 (8.8) |
50,846 (9.1) |
| Maintenance |
32,632 (8.9) |
48,056 (6.3) |
22,675 (7.2) |
57,980 (10.4) |
Hypertension was defined as SBP ≥140 mmHg, DBP ≥90 mmHg, or use of blood pressure-lowering medications. Diabetes was defined as fasting glucose level ≥126 mg/dL or use of glucose-lowering medications. Dyslipidemia was defined as low-density lipoprotein cholesterol level ≥140 mg/dL, high-density lipoprotein cholesterol level <40 mg/dL, triglyceride level ≥150 mg/dL, or use of lipid-lowering medications. Alcohol consumption was defined based on self-reported questionnaires administered during health checkups, specifically identifying daily alcohol consumption. BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Standard questionnaire question items used in Japanese health checkups include “Are you going to start, or have you started lifestyle modifications? (e.g., increase physical activity, improve dietary habits)”. The responses include: 1, I don’t intend to start; 2, I’m going to start in the future (e.g., within 6 months); 3, I’m going to start soon (e.g., in a month) or have just started some of them; 4, I already started (<6 months ago) and 5, I already started (≥6 months ago). These responses correlate with the 5 stages of behavior change: precontemplation, contemplation, preparation, action, and maintenance, respectively.7,10
Statistical Analysis and Ethics Approval
We examined the association between the baseline stage of behavior change and each unhealthy lifestyle at 1 and 2 years following the baseline checkup using logistic regression models adjusted for potential confounders that included age, sex, body mass index, hypertension, diabetes, dyslipidemia, alcohol consumption, and unhealthy lifestyle (other than the target unhealthy behaviors). In addition, we also evaluated the relationship between the baseline stage of behavior change and continuity of each unhealthy lifestyle for 2 years. In these analyses, we did not adjust the stage of change and other variables 1 year later. This study was approved by the Institutional Review Board of the University of Tokyo in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived because all data in the JMDC Claims Database are deidentified.
Results
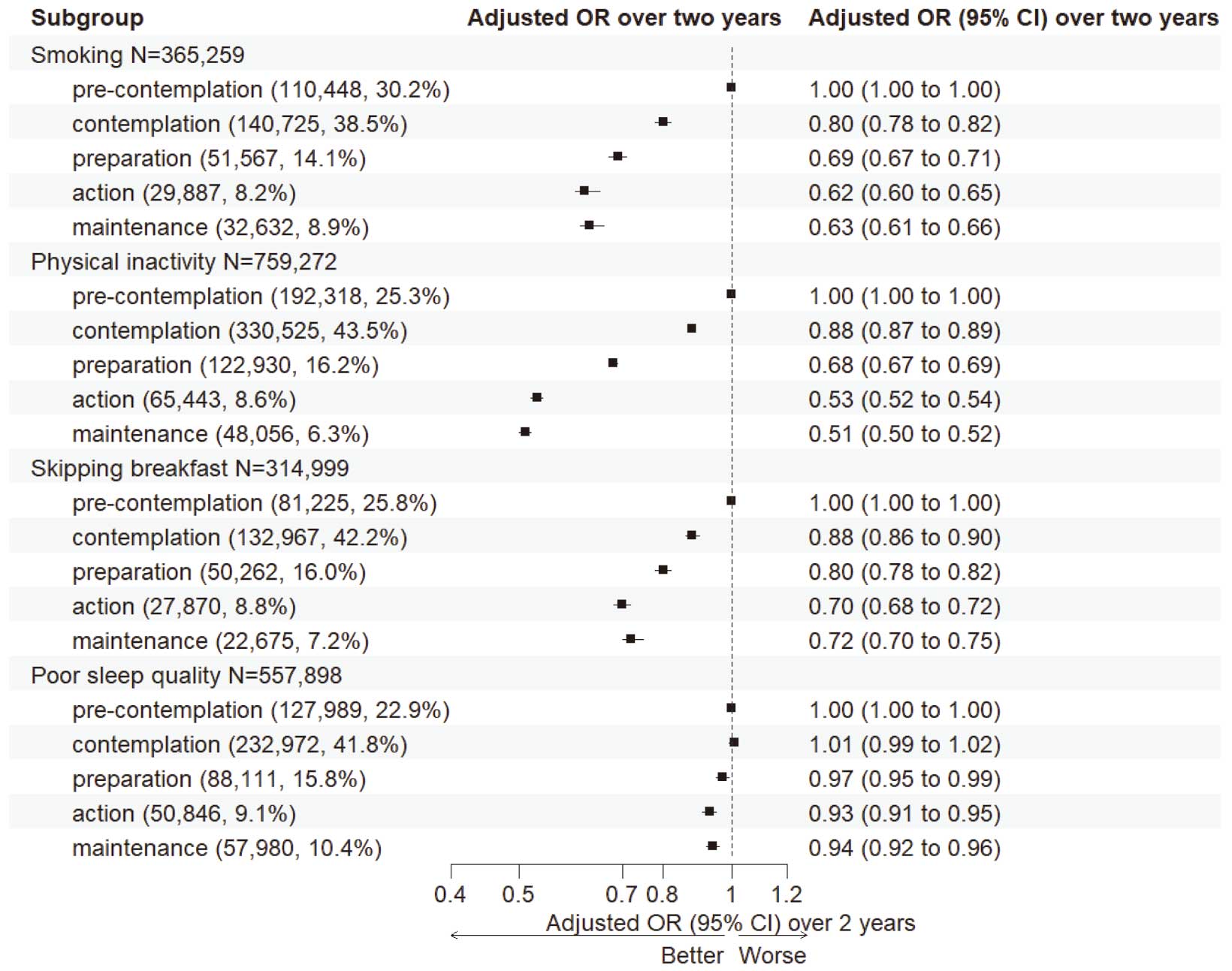
Of all enrolled individuals, 341,852/365,259 (93.6%) failed to quit smoking, 611,106/759,272 (80.5%) did not engage in regular exercise, 256,808/314,999 (81.5%) did not establish a regular breakfast habit, and 413,408/557,898 (74.1%) failed to improve their sleep quality at 1 year. At 2 years, 328,026/365,259 (89.8%) were unable to quit smoking, 588,591/759,272 (77.5%) did not engage in regular exercise, 238,520/314,999 (75.7%) did not establish a regular breakfast habit, and 384,741/557,898 (69.0%) failed to improve their sleep quality. Over the course of these 2 years, it is noteworthy that certain individuals succeeded in adopting and sustaining healthy behaviors, but there were also cases of relapse (Table 2). Even after adjusting for covariates, the baseline stage of behavior change level was associated with the persistence of unhealthy lifestyles at 1 and 2 years after baseline (Figure 1). Likewise, when analyzing the persistence of unhealthy behaviors throughout the 2-year study duration, we discovered consistent patterns that aligned with the findings from each individual year (Figure 2). As the Figures show, the effect of the difference in baseline stage of change varied across the target behaviors.
Table 2. Proportions of Individuals With and Without Achieved Healthy Behaviors
| At 1 year |
At 2 years |
n (%) |
| Smoking (n=365,259) |
| Not Achieved |
Not Achieved |
321,627 (88.1) |
| Not Achieved |
Achieved |
20,225 (5.5) |
| Achieved |
Not Achieved |
6,399 (1.8) |
| Achieved |
Achieved |
17,008 (4.7) |
| Physical inactivity (n=759,272) |
| Not Achieved |
Not Achieved |
522,761 (68.9) |
| Not Achieved |
Achieved |
88,345 (11.6) |
| Achieved |
Not Achieved |
65,830 (8.7) |
| Achieved |
Achieved |
82,336 (10.8) |
| Skipping breakfast (n=314,999) |
| Not Achieved |
Not Achieved |
219,886 (69.8) |
| Not Achieved |
Achieved |
36,922 (11.7) |
| Achieved |
Not Achieved |
18,634 (5.9) |
| Achieved |
Achieved |
39,557 (12.6) |
| Poor sleep quality (n=557,898) |
| Not Achieved |
Not Achieved |
331,457 (59.4) |
| Not Achieved |
Achieved |
81,951 (14.7) |
| Achieved |
Not Achieved |
53,284 (9.6) |
| Achieved |
Achieved |
91,206 (16.3) |
Discussion
To the best of our knowledge, this is the first large-scale study to investigate the association between the baseline stage of behavior change intention and future cardiovascular healthy behaviors. We obtained 3 major findings from this study. First, the baseline stage of change model obtained by a general questionnaire was associated with future cardiovascular healthy behaviors. Second, this association was found to be significant not just at the 1-year mark but also at the 2-year evaluation point. Third, when considering cardiovascular healthy behaviors, the predictability of each stage of change model may differ across the behaviors (e.g., better association with smoking cessation, physical activity, and healthy diet than with sleep quality).
Focusing on health behaviors such as diet, physical activity, nicotine exposure, and sleep, as well as health factors such as body mass index, blood lipids, blood glucose, and blood pressure will help to enhance cardiovascular health outcomes.10–12 Several systematic reviews have demonstrated the efficacy of the Stage of Change model in improving each of these health behaviors, including smoking cessation, physical activity, healthy diet, and better sleep quality, which aligns with the findings of our study.11–13 Unlike previous studies that focused on specific behaviors (e.g., the precontemplation stage to quit smoking), our study included a questionnaire seeking information about general lifestyle changes. This approach has shown that a simple, general stages of change questionnaire can predict many aspects of future cardiovascular health behavior, including sleep health, which is believed to be an important factor in reducing the incidence of CVD. Because the term “lifestyle modification” can encompass a broad range of behaviors, our study highlights the usefulness of a general questionnaire to effectively capture the stage of change across multiple behaviors. This approach has the potential to promote more comprehensive and personalized interventions to improve cardiovascular health outcomes. Furthermore, our study has also revealed that a noteworthy portion of individuals engaging in unhealthy behaviors (e.g., smoking) in one area perceive their lifestyle modifications as being in the stage of “maintenance”.
Study Limitations
Although we defined cardiovascular healthy behaviors, both behavior intention and actual behavioral change were only defined by questionnaires and surveys. For instance, the inclusion of sleep duration as a measure of health-promoting behavior would provide a more comprehensive understanding than focusing solely on sleep quality. Further study is required to evaluate the effect of each baseline stage of health behavior change on actual behavior monitored by wearable devices. The relationship between behavior change intention and improved sleep quality was weaker than for the other 3 behaviors. Various factors underlying poor sleep quality may have contributed to this result. There could also be unmeasured confounders in our dataset and residual bias even after adjustment of available variables. The clinical course after the initial checkup could have affected the outcomes.
Conclusions
Baseline behavior change intention according to the transtheoretical model was associated with modification of unhealthy behaviors including cigarette smoking, physical inactivity, skipping breakfast, and poor sleep quality, suggesting that individuals’ motivation to change unhealthy behavior may contribute to lifestyle modification and could be preventive of subsequent CVD.
Funding
This work was supported by grants from the Ministry of Health, Labour and Welfare, Japan (21AA2007) and the Ministry of Education, Culture, Sports, Science and Technology, Japan (20H03907, 21H03159, and 21K08123). The funding sources had nothing regarding this study.
Disclosures
Research funding and scholarship funds (H.K. and K.F.) from Medtronic Japan Co., Ltd.; Biotronik Japan; Simplex Quantum Co., Ltd.; Boston Scientific Japan Co., Ltd.; and Fukuda Denshi, Central Tokyo Co., Ltd. The remaining authors have nothing to disclose. I.K., H.M., and K.N. are members of Circulation Journal’s Editorial Team.
IRB Information
Name of the ethics committee: the Clinical Research Review Board of The University of Tokyo. Reference no. 2018-10862.
References
- 1.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global Burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 Study. J Am Coll Cardiol 2020; 76: 2982–3021.
- 2.
Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, et al. Life’s Essential 8: Updating and enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation 2022; 146: e18–e43.
- 3.
DiClemente CC, Prochaska JO, Fairhurst SK, Velicer WF, Velasquez MM, Rossi JS. The process of smoking cessation: An analysis of precontemplation, contemplation, and preparation stages of change. J Consult Clin Psychol 1991; 59: 295–304.
- 4.
Sekizuka H, Kida K. Behavior change and prognosis in patients with heart failure: Salt reduction guidance and readiness for heart failure treatment. Circ J 2021; 85: 1563–1564.
- 5.
Robinson AH, Norman GJ, Sallis JF, Calfas KJ, Rock CL, Patrick K. Validating stage of change measures for physical activity and dietary behaviors for overweight women. Int J Obes 2008; 32: 1137–1144.
- 6.
Jiménez-Zazo F, Romero-Blanco C, Castro-Lemus N, Dorado-Suárez A, Aznar S. Transtheoretical model for physical activity in older adults: Systematic review. Int J Environ Res Public Health 2020; 17: 9262.
- 7.
Ikeda N, Saito E, Kondo N, Inoue M, Ikeda S, Satoh T, et al. What has made the population of Japan healthy? Lancet 2011; 378: 1094–1105.
- 8.
Kaneko H, Itoh H, Yotsumoto H, Kiriyama H, Kamon T, Fujiu K, et al. Association of isolated diastolic hypertension based on the cutoff value in the 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines with subsequent cardiovascular events in the general population. J Am Heart Assoc 2020; 9: e017963.
- 9.
Kaneko H, Itoh H, Kiriyama H, Kamon T, Fujiu K, Morita K, et al. Possible association between eating behaviors and cardiovascular disease in the general population: Analysis of a nationwide epidemiological database. Atherosclerosis 2021; 320: 79–85.
- 10.
Nakayama S, Dote T, Hayashi E, Okamoto R, Kurokawa H, Yokoyama H, et al. Longitudinal relationships between Stages of Changes in the transtheoretical model and annual data changes in mandatory routine health checkups of university faculty. J Jpn Occupational Med Traumatol 2012; 60: 165–175.
- 11.
Bridle C, Riemsma RP, Pattenden J, Sowden AJ, Mather L, Watt IS, et al. Systematic review of the effectiveness of health behavior interventions based on the transtheoretical model. Psychol Health 2005; 20: 283–301.
- 12.
Hashemzadeh M, Rahimi A, Zare-Farashbandi F, Alavi-Naeini AM, Daei A. Transtheoretical model of health behavioral change: A systematic review. Iran J Nurs Midwifery Res 2019; 24: 83–90.
- 13.
Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al. Systematic review of the effectiveness of stage based interventions to promote smoking cessation. BMJ 2003; 326: 1175–1177.