Abstract
Background: Equality in training opportunities, studying abroad, and satisfaction with work are not well investigated among Japanese cardiologists.
Methods and Results: We studied cardiologists’ career development using a questionnaire that was emailed to 14,798 cardiologists belonging to the Japanese Circulation Society (JCS) in September 2022. Feelings regarding equality in training opportunities, preferences for studying abroad, and satisfaction with work were evaluated with regard to cardiologists’ age, sex, and other confounding factors. Survey responses were obtained from 2,566 cardiologists (17.3%). The mean (±SD) age of female (n=624) and male (n=1,942) cardiologists who responded to the survey was 45.6±9.5 and 50.0±10.6 years, respectively. Inequality in training opportunities was felt more by female than male cardiologists (44.1% vs. 33.9%) and by younger (<45 years old) than older (≥45 years old) (42.0% vs. 32.8%). Female cardiologists were less likely to prefer studying abroad (53.7% vs. 59.9%) and less satisfied with their work (71.3% vs. 80.8%) than male cardiologists. Increased feelings of inequality and lower work satisfaction were investigated among cardiologists who were young, had family care duties, and had no mentors. In the subanalysis, significant regional differences were found in cardiologists’ career development in Japan.
Conclusions: Female and younger cardiologists felt greater inequality in career development than male and older cardiologists. A diverse workplace may prompt equality in training opportunities and work satisfaction for both female and male cardiologists.
Globally, the proportion of female physicians has increased over the past 3 decades. In Japan, in 2020, 22.8% of physicians were female, and the proportion of women is higher in younger generations.1 Although it is anticipated that more women will become doctors in the future, they are still markedly underrepresented in cardiology,2 especially in interventional cardiology, which is persistently ranked at the bottom in terms of gender equality.3 As of March 2022, the Japanese Circulation Society (JCS) had 32,620 members.4 Although the overall number of members in the JCS has increased, the proportion of young members has decreased. To increase the number of young cardiologists with support, academic societies need to urgently improve the working environment for cardiologists, regardless of gender. Moreover, a diverse workplace environment that allows female and younger cardiologists to work comfortably can also be considered a good workplace environment for male cardiologists. Sharma et al5 recommend gender equality in training opportunities and the development of mentoring programs to enhance the recruitment, retention, and career development of female cardiologists. In Japan, the medical office system, the regions cardiologists belong to, child care or family nursing duties, having mentors, and the number of female cardiologists in each region may promote or inhibit feelings of equality with regard to training opportunities, studying abroad, and overall satisfaction with work. However, there have been few studies on the current status of career development among Japanese cardiologists.
In this study we analyzed the current status of subspeciality selection and perceptions of equality regarding training opportunities, preferences for study abroad, and work satisfaction according to cardiologists’ gender using a qualitative survey method to identify background factors that may obstruct career development, with the aim of improving the workplace environment.
Methods
Study Design
A qualitative survey was conducted by the research team of the Committee for Diversity Promotion of the JCS to investigate cardiologists’ career development and satisfaction with work. Demographic information, such as gender, age, subspecialities in cardiology, child- or eldercare duties, belonging to university hospitals, belonging to the medical offices, degree status, the presence of mentors, and district, was collected to examine gender and regional differences in career development.
A Google form was used for the questionnaire (Supplementary File); valid responses were those in which all survey questions had been answered. The questionnaire was sent by email to 14,798 cardiologists who were JCS members in September 2022. The questionnaire requested respondents’ some personal information (e.g., age, years as a cardiologist or subspecialist, and career aspirations or experiences). Survey responses were obtained from 2,566 cardiologists (17.3% response rate), with all identifying personal information removed.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Further, the study design was approved by the JCS Ethics Committee (Reference no. 15). Informed consent was obtained from all participants according to the protocol approved by the JCS Ethics Committee.
Outcomes
We investigated factors promoting or inhibiting feelings of equality in training opportunities, studying abroad, and overall satisfaction with work for career development among cardiologists in Japan.
We analyzed the impact of medical offices, an organizational system used in departments of university hospitals in which Ikyoku-Kouza are academic teaching units at a university’s school of medicine.6 We also investigated the awareness of career development according to urban or rural region, with areas divided into 3 groups based on prefecture population: <1.5 million (rural), 1.5–3 million (suburban), and >3 million (urban). In order to investigate the impact of cardiologist density on feelings of inequality, preference for studying abroad, and work satisfaction, the number of the JCS doctor members per 100,000 population in each prefecture was classified into 3 groups (<20, 20–25, and >25 per 100,000 population), with cardiologists’ perception examined in each group. In addition, we analyzed cardiologists’ feelings of inequality, preference for studying abroad, and work satisfaction according to the percentage of female JCS members in each prefecture. We used population data by prefecture from the Basic Resident Ledger by age group as of January 1, 2022.7
Statistical Analysis
JCS member characteristics were compared using the χ2
test for non-continuous variables and an unpaired t-test for normally distributed continuous data in SPSS v22 (IBM Inc., Armonk, NY, USA). Non-continuous variables are presented as percentages and normally distributed continuous data are presented as the mean±SD.
A logistic regression analysis was used to analyze the contribution of each factor to perceived inequalities in opportunities, preferences for studying abroad, and overall satisfaction with work, with factors showing P<0.05 in univariate analysis included in the logistic regression analysis. Differences between groups were examined using the Bonferroni method for multiple comparison tests. We used the Cochrane-Armitage test to test the trend of the proportions using Easy R (EZR).8 Briefly, EZR is a modified version of the R command designed to add statistical functions frequently used in biostatistics. The level of significance was set at an α level of 0.05.
Results
Respondents’ Background
In all, 2,566 valid responses were received (Figure 1) from all districts around Japan. The mean age of female cardiologists (n=624; 24.3%) was 45.6±9.5 years, with 47.4% being of younger (<45 years) age; the mean age of male cardiologists (n=1,942; 75.7%) was 50.0±10.6 years, with 33.7% being of younger (<45 years) age. The characteristics of the respondents are presented in Table 1. In all, 2,461 respondents (95.9%) had specialist qualifications in cardiology, surgery, pediatrics, or others, or were preparing for the examination. A total of 71.0% of respondents had qualified with a doctor degree (PhD), 34.7% belonged to university hospitals, and 86.9% were engaged in cardiovascular internal medicine. Among the respondents, 50.7% had childcare duties, 7.9% had eldercare duties, and 7.2% had both.
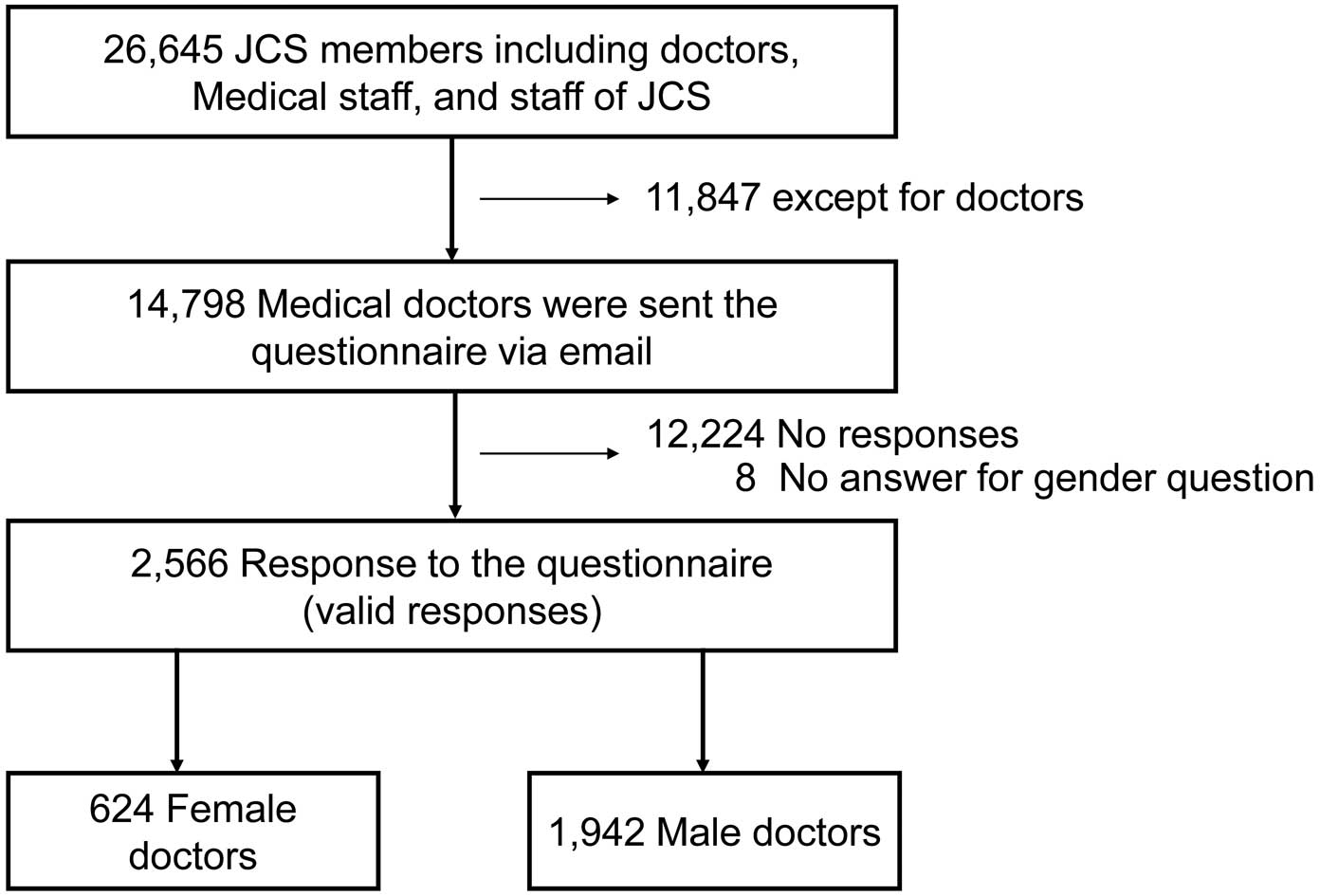
Table 1. Background Characteristics of the Respondents
| |
Female cardiologists |
Male cardiologists |
P value |
| Total number |
624 |
1,942 |
|
| Mean (±SD) age (years) |
45.6±9.5 |
50.0±10.6 |
0.0001 |
| Age group (years) |
| <30 |
17 (2.7) |
18 (0.9) |
|
| 30–39 |
156 (25.0) |
315 (16.2) |
|
| 40–49 |
230 (36.9) |
595 (30.6) |
|
| 50–59 |
163 (26.1) |
602 (31.0) |
|
| 60–69 |
36 (5.8) |
323 (16.6) |
|
| 70–79 |
4 (0.6) |
59 (0.3) |
|
| 80–89 |
2 (0.3) |
4 (0.2) |
|
| ≥90 |
0 (0.0) |
1 (0.1) |
|
| Unknown |
16 (2.6) |
25 (1.3) |
|
| Years as a cardiologist |
|
|
0.0001 |
| <3 |
28 (4.5) |
33 (1.7) |
|
| 3–5 |
33 (5.3) |
54 (2.8) |
|
| 6–10 |
89 (14.3) |
189 (9.7) |
|
| 11–20 |
260 (41.7) |
608 (31.3) |
|
| ≥21 |
214 (34.3) |
1,058 (54.5) |
|
| Specialist qualifications |
|
|
0.0001 |
| Yes or preparing |
582 (93.3) |
1,879 (96.8) |
|
| No, not planning |
42 (6.7) |
63 (3.2) |
|
| Having a doctor degree (PhD) |
|
|
0.0001 |
| Yes |
383 (61.4) |
1,438 (74.0) |
|
| Proceeding |
82 (13.1) |
189 (9.7) |
|
| No (not planned) |
159 (25.5) |
315 (16.2) |
|
| Caring duties |
|
|
0.001 |
| Childcare duties |
252 (40.4) |
1,049 (54.0) |
|
| Eldercare duties |
77 (12.3) |
125 (6.4) |
|
| Child- and eldercare duties |
44 (7.1) |
140 (7.2) |
|
| No caring duties |
251 (40.2) |
628 (32.3) |
|
| Working hospital |
|
|
0.991 |
| University hospital |
226 (36.2) |
664 (34.1) |
|
| City hospital (<10 doctors) |
148 (23.7) |
428 (22.0) |
|
| City hospital (10–19 doctors) |
63 (10.1) |
208 (10.7) |
|
| City hospital (≥20 doctors) |
96 (15.4) |
345 (17.8) |
|
| Clinic |
73 (11.7) |
264 (13.6) |
|
| Other |
18 (2.9) |
33 (1.7) |
|
| Speciality |
|
|
0.0001 |
| Cardiovascular medicine (internal) |
563 (90.2) |
1,666 (85.8) |
|
| Surgery |
19 (3.0) |
158 (8.1) |
|
| Pediatrics |
20 (3.2) |
52 (2.7) |
|
| Emergency department |
2 (0.3) |
17 (0.9) |
|
| Basic research |
8 (1.3) |
7 (0.4) |
|
| Others |
8 (1.3) |
10 (0.5) |
|
| Unknown |
4 (0.6) |
32 (1.6) |
|
| Subspeciality |
|
|
0.0001 |
| Ischemia |
81 (13.0) |
572 (29.5) |
|
| Arrhythmia |
73 (11.7) |
304 (15.7) |
|
| Heart failure |
71 (11.4) |
257 (13.2) |
|
| Imaging |
156 (25.0) |
132 (6.8) |
|
| Hypertension/vascular disease |
24 (3.8) |
112 (5.8) |
|
| Surgery |
15 (2.4) |
120 (6.2) |
|
| Basic |
27 (4.3) |
73 (3.8) |
|
| Pediatrics/congenital heart disease |
20 (3.2) |
65 (3.3) |
|
| Cardiac rehabilitation |
36 (5.8) |
49 (2.5) |
|
| Medical checkup |
40 (6.4) |
39 (2.0) |
|
| Emergency |
6 (1.0) |
63 (3.2) |
|
| Structural heart disease |
9 (1.4) |
51 (2.6) |
|
| None |
21 (3.4) |
26 (1.3) |
|
| Pulmonary hypertension |
7 (1.1) |
23 (1.2) |
|
| Others |
28 (4.5) |
50 (2.6) |
|
| Considering |
10 (1.6) |
6 (0.3) |
|
Unless indicated otherwise, data are given as n (%). PhD, Doctor of Philosophy.
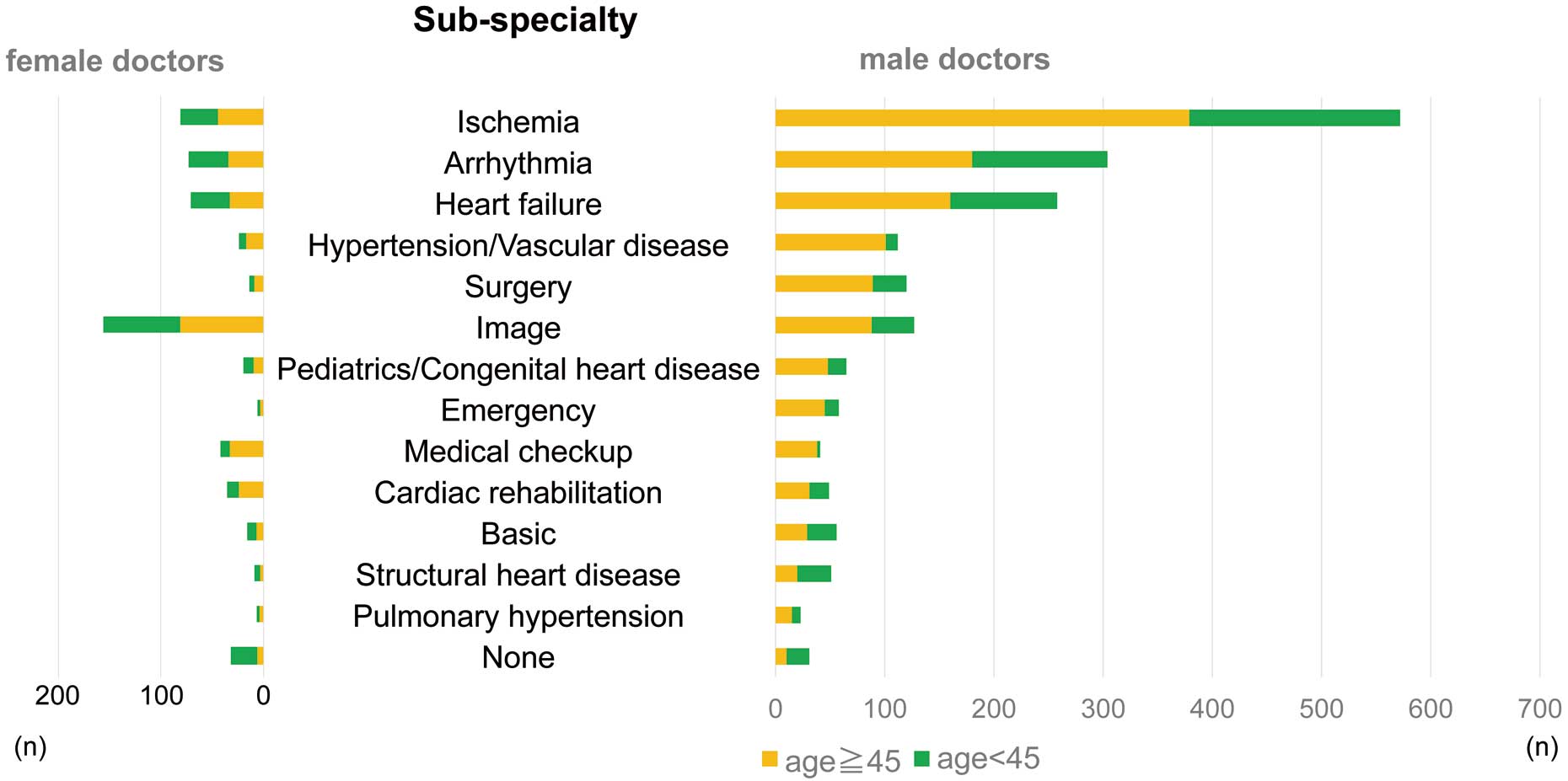
From the subspeciality analysis, the volume of cardiologists specializing in ischemia, arrhythmia, and heart failure was high (25.4%, 14.7%, and 12.8%, respectively; Table 1; Figure 2). There was a lower proportion of women than men specializing in ischemia (13.0% vs. 29.5%), cardiac surgery (2.4% vs. 6.2%), and emergency medicine (1.0% vs. 3.2%). Conversely, a lower-than-average (37.1%) proportion of younger (<45 years) respondents specialized in hypertension/vascular disease, medical checkup, emergency medicine, pediatrics/congenital heart disease, cardiac rehabilitation, and ischemia (Figure 3).
Factors Influencing Inequality of Training Opportunities, Studying Abroad, and Overall Satisfaction
Regarding training opportunities, female cardiologists felt more inequality, which was identified on the basis of the sum of ‘Yes’ and ‘Often Yes’ responses to the question regarding feelings of inequality, than males (44.1% vs. 33.9%; P<0.0001; Table 2). Female cardiologists also had a reduced preference for studying abroad, which was identified as ‘No’ responses to the question about preferring to study abroad (46.3% vs. 40.1%; P=0.012), and were less satisfied with their work, which was identified as the sum of ‘Yes’ and ‘Often Yes’ responses to the question about work satisfaction (71.3% vs. 80.8%, P<0.0001), than males (Table 2). Cardiologists belonging to medical offices preferred studying abroad compared with cardiologists not belonging to a medical office (P<0.0001). Regardless of gender, cardiologists who had mentors (49.8%) felt less inequality (30.6% vs. 48.6%; P=0.0001), were more motivated to study abroad (61.8% vs. 52.4%; P=0.0001), and felt higher overall satisfaction (89.1% vs. 68.2%; P<0.0001).
Table 2. Responses to the Questionnaire
| |
Female cardiologists
(n=624) |
Male cardiologists
(n=1,942) |
P value |
| District respondent belongs to |
|
|
0.001 |
| Hokkaido |
21 (3.4) |
76 (3.9) |
|
| Tohoku |
30 (4.8) |
120 (6.2) |
|
| Tokyo City |
148 (23.7) |
274 (14.1) |
|
| Kanto (except for Tokyo City) |
96 (15.4) |
337 (17.4) |
|
| Tokai |
51 (8.2) |
218 (11.2) |
|
| Hokuriku |
14 (2.2) |
48 (2.5) |
|
| Kinki |
115 (18.4) |
408 (21.0) |
|
| Shikoku |
33 (5.3) |
79 (4.0) |
|
| Chugoku |
29 (4.6) |
134 (6.9) |
|
| Kyushu |
87 (13.9) |
248 (12.8) |
|
| Belonging to university |
|
|
0.583 |
| Yes |
227 (36.4) |
670 (34.5) |
|
| No |
397 (63.6) |
1,272 (65.5) |
|
| Belonging to office |
|
|
0.597 |
| Yes |
445 (71.3) |
1,383 (71.2) |
|
| No |
179 (28.7) |
559 (28.8) |
|
| Presence of mentors |
|
|
0.684 |
| Yes |
79 (12.7) |
245 (12.6) |
|
| Often yes |
235 (37.7) |
720 (37.1) |
|
| Often no |
117 (18.8) |
385 (19.8) |
|
| No |
85 (13.6) |
210 (10.8) |
|
| No opinion |
108 (17.3) |
382 (19.7) |
|
| Feeling of inequality |
|
|
0.0001 |
| Yes |
79 (12.7) |
149 (7.7) |
|
| Often yes |
196 (31.4) |
510 (26.3) |
|
| No |
349 (55.9) |
1,283 (66.0) |
|
| Total no. “yes” and “often yes” responses |
275 (44.1) |
659 (33.9) |
|
| Prefer to study abroad |
|
|
0.012 |
| Yes, done |
152 (24.3) |
747 (38.5) |
|
| Yes, preparing |
25 (4.0) |
102 (5.3) |
|
| Yes, but cannot |
139 (22.3) |
264 (13.6) |
|
| Only domestic |
19 (3.0) |
50 (2.6) |
|
| No |
289 (46.3) |
779 (40.1) |
|
| Total no. except for “no” responses |
335 (53.7) |
1,163 (59.9) |
|
| Satisfied with work |
|
|
0.0001 |
| Yes |
126 (20.2) |
592 (30.5) |
|
| Often yes |
319 (51.1) |
977 (50.3) |
|
| Often no |
109 (17.5) |
219 (11.3) |
|
| No |
40 (6.4) |
97 (5.0) |
|
| No opinion |
30 (4.8) |
57 (2.9) |
|
| Total no. “yes” and “often yes” responses |
445 (71.3) |
1,569 (80.8) |
|
Unless indicated otherwise, data are given as n (%).
Male cardiologists with family care duties felt more inequality than those without family care duties (36.5% vs. 28.7%; P=0.001), whereas there was no significant difference in feelings of inequality between female cardiologists with and without family care duties (46.4% vs. 40.6%, respectively; P=0.156; Supplementary Table 1). Male cardiologists without family care duties were significantly more satisfied with their work than male cardiologists with family care duties (86.0% vs. 81.9%; P=0.026). Again, there was no significant difference in work satisfaction between female cardiologists with and without family care duties (73.0% vs. 77.7%, respectively; P=0.196).
Younger (<45 years) male cardiologists felt more inequality than older male cardiologists (40.5% vs. 30.5%; P=0.001), but the feelings of inequality were similar for younger and older female cardiologists (45.5% vs. 42.1%, respectively; P=0.402; (Supplementary Table 1). Preferences for studying abroad were similar between younger and older cardiologists, regardless of sex. Older cardiologists were more satisfied with work than younger cardiologists in both sexes (men, 87.4% vs. 75.0%, respectively [P=0.0001]; women, 81.1% vs. 67.4%, respectively [P=0.0001]).
Logistic Regression Analysis for Each Outcome
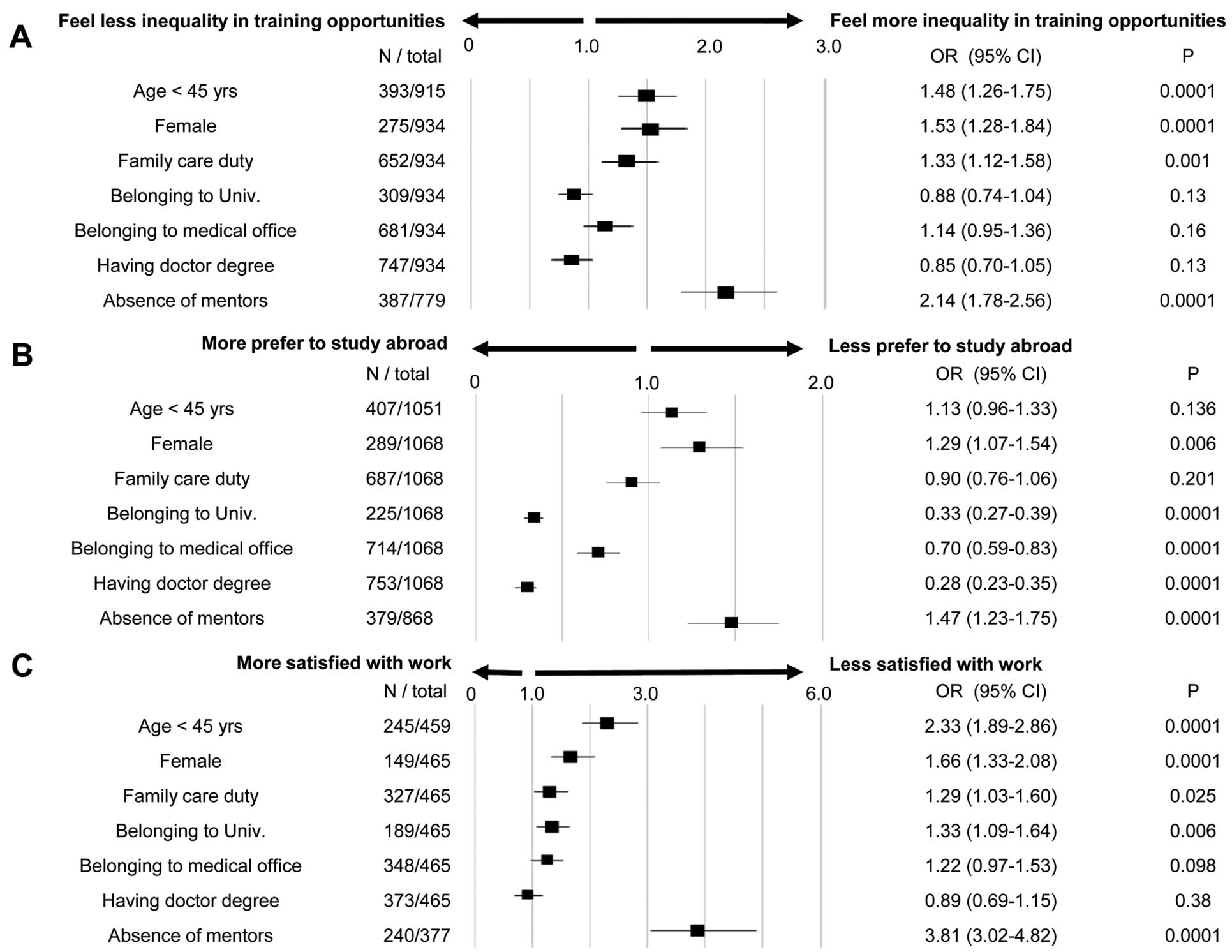
A logistic regression analysis of answers regarding inequality of opportunities revealed that younger (<45 years) cardiologists (odds ratio [OR] 1.48; 95% confidence interval [CI] 1.26–1.75; P<0.0001), female cardiologists (OR 1.53; 95% CI 1.28–1.84; P<0.0001), cardiologists with family care duties (OR 1.33; 95% CI 1.12–1.58; P=0.001), and cardiologists without mentors (OR 2.14; 95% CI 1.78–2.56; P<0.0001) felt significantly more inequality of opportunities (Figure 4A).
The significant factors that reduced preferences for studying abroad were female sex (OR 1.29; 95% CI 1.07–1.54; P=0.006) and not having a mentor (OR 1.47; 95% CI 1.23–1.75; P<0.0001). Cardiologists belonging to university hospitals (OR 0.33; 95% CI 0.27–0.39; P<0.0001) or doctor’s offices (OR 0.70; 95% CI 0.59–0.83; P<0.0001), and having a doctor degree (OR 0.28; 95% CI 0.23–0.35; P<0.0001) tended to prefer to study abroad (Figure 4B).
With regard to overall satisfaction, younger (<45 years) age (OR 2.33; 95% CI 1.89–2.86; P<0.0001), female sex (OR 1.66; 95% CI 1.33–2.08; P<0.0001), having family care duties (OR 1.29; 95% CI 1.03–1.60; P=0.025), belonging to a university hospital (OR 1.33; 95% CI 1.09–1.64; P=0.006), and not having a mentor (OR 3.81; 95% CI 3.02–4.82, P<0.0001) were significantly correlated with less work satisfaction (Figure 4C).
Regional Analysis of Inequality in Training Opportunities, Studying Abroad, and Overall Satisfaction
The rate of respondents by region was almost the same as the rate of JCS members (Table 2).9 Of the respondents, female cardiologists felt more inequality of opportunities for their career progression than males (44.1% vs. 33.9%; P<0.0001). When analyzed by gender in each district, female cardiologists in Hokkaido District, Tohoku District, Tokyo City, Kanto District without Tokyo City, and Tokai District felt more inequality of opportunities than their male counterparts in each district (57.1% vs. 42.9% [P=0.048], 53.3% vs. 29.2% [P=0.034], 50.7% vs. 30.7% [P<0.0001], 52.1% vs. 47.9% [P=0.031], and 52.9% vs. 35.8% [P=0.041], respectively; Figure 5A). In Hokuriku District, inequality was significantly more prevalent among male than female cardiologists (45.8% vs. 14.3%; P=0.049).

Female cardiologists had a lower preference rate for studying abroad than male cardiologists in the overall analysis (53.7% vs. 59.9%; P=0.006). Female cardiologists in Tokyo City and Kyushu District, areas with a larger number of respondents, were less inclined to study abroad than their male counterparts (60.8% vs. 72.6% [P=0.013] and 42.5% vs. 59.7% [P=0.014]; respectively). There were no significant differences according to gender in other districts with regard to preferences for studying abroad (Figure 5B).
Female cardiologists were significantly less satisfied with their work than male cardiologists (71.3% vs. 80.8%; P<0.0001). This trend for a lower satisfaction rate among female than male cardiologists was particularly evident in Tokyo City (72.9% vs. 83.6%; P=0.013), Kinki District (71.3% vs. 82.2%; P=0.006), and Kyushu District (76.2% vs. 82.2%; P=0.021; Figure 5C).
Analysis by prefecture is presented in Supplementary Table 2. When survey responses were examined by prefecture population (Figure 6A), there were no differences in inequality, preferences for studying abroad, or work satisfaction among male cardiologists; however, the preference for studying abroad among female cardiologists tended to increase as the prefecture population increased (43.8% in the group with <1.5 million people, 49.5% in the group with 1.5–3 million people, and 58.8% in the group with >3 million people; P=0.002). When survey responses examined according to cardiologist density (Figure 6A), feelings of inequality tended to decrease among male cardiologists as the number of cardiologists per 100,000 population increased (36.1%, 35.4%, and 30.7% in the group with <20, 20–25, and >25 cardiologists per 100,000 population, respectively; P=0.030).

After analyzing the feelings of inequality, preferences for studying abroad, and satisfaction among cardiologists according to the ratio of female JCS members in each prefecture (Figure 6B), male cardiologists tended to feel less inequality of opportunities with an increase in the proportion of female cardiologists (37.2%, 34.0%, and 31.7% in the group with <11%, 11–14%, and >14% female JCS members, respectively; P=0.034). In addition, male cardiologists tended to prefer studying abroad as the proportion of female cardiologists increased (56.5%, 56.9%, and 63.9% in the group with <11%, 11–14%, and >14% female JCS members, respectively; P=0.004).
Discussion
In this study, a nationwide survey questionnaire of cardiologists by the JCS revealed that cardiologist without mentors, female cardiologists, younger cardiologists, and cardiologists with family care duties perceived greater inequality in training opportunities. Cardiologists without mentors and female cardiologists were less likely to study abroad. Cardiologists without mentors, younger cardiologists, female cardiologists, cardiologists with family care duties, or cardiologists belonging to university hospitals were less satisfied with work. The absence of mentors had the most negative impact on perceptions of inequality, preferences for studying abroad, and work satisfaction.
Background and Subspecialities of Survey Respondents
Subspeciality examination revealed that women were underrepresented in ischemia, cardiac surgery, and emergency medicine, which is comparable to reports from other countries.3,10 In the field of interventional cardiology, low work flexibility, heavy responsibilities, radiation exposure during pregnancy, and the absence of female role models and mentors were reported to influence subspecialty choice.3 It has also been reported that Japanese female surgeons have fewer surgical opportunities than male surgeons in the field of gastroenterological surgery,11 and these reasons may influence gender differences in subspeciality selection. Moreover, in the present study, there were lower mean rates of younger (<45 years) cardiologists in hypertension/vascular disease, medical checkup, emergency medicine, pediatrics/congenital heart disease, cardiac rehabilitation, and ischemia. From the meta-analysis, the main factors cited for subspeciality choice among medical students were academic interests, competencies, controllable lifestyles or flexible work schedules, patient service orientation, medical teachers or mentors, career opportunities, workload or working hours, income, length of training, and prestige, among others.12 However, because there have been few studies on trends and reasons for subspeciality choice among Japanese cardiologists, further studies are warranted.
Factors Influencing Inequality of Training Opportunities and Overall Satisfaction
Overall, cardiologists with family care duties were more likely to feel inequality. Analysis by gender revealed that male cardiologists with family care duties felt more inequality than those without such duties, whereas there was no difference in perceptions of inequality between female cardiologists who had family care duties and those who did not. Women have reported having wage disparities and prejudice, lack of organizational support, lack of role models, and inadequate workplace support during pregnancy and childcare compared with men,13 and therefore it is possible that they often feel inequality regardless of whether they have family care duties. In contrast, work satisfaction was lower for male cardiologists without than with family care duties, although work satisfaction was similar for female cardiologists with and without family care duties. Some studies have reported that women have more household responsibilities and housework, which may have traditionally limited their career development in Japan,14,15 suggesting that differences in environment and roles by gender may influence work satisfaction. Working in a setting that offers more flexible hours, such as part-time work or job sharing, may improve cardiologists’ work-life balance and support their child-rearing.
Other notable findings of this study were that younger cardiologists had less work satisfaction. Kohlfurst et al reported lower job satisfaction among younger pediatricians,16 because early career doctors assume substantial responsibility with a short period of experience and have long working hours, psychological stress, and rapid changes in living environment. Although the present study did not examine cardiologists’ working styles and the stresses they face, similar reasons could be behind the lower work satisfaction among younger cardiologists. In addition, this study revealed a sense of inequality in training opportunities among younger cardiologists. In a review of medical researchers considering Japanese cultural characteristics, Japanese organizations have been reported as hierarchical, and mentoring relationships are primarily centered around mentors, who often show mentees the path they should take.17 This mentor-driven environment may lead to higher inequality of training among younger cardiologist. Other factors included lower levels of work satisfaction among those affiliated with universities. This could be because university work is more complex, where teaching and research are required in addition to clinical work.6 In contrast, the desire to study abroad was higher among those affiliated with university hospitals. This is likely due to their exposure to the research environment. In addition, female cardiologists are less likely to study abroad because lifestyle changes may affect the way they work and they have less opportunity to study abroad.18,19
Regional Analysis of Inequality of Training Opportunities and Preferences for Studying Abroad
An analysis regarding the proportion of female members of the JCS in each prefecture revealed that the more female cardiologists in the same prefecture, the less male feelings of inequality decreased. Furthermore, the more female cardiologists, the more male cardiologists expressed a preference for studying abroad. There were 10 recommendations for the employment and career development of female cardiologists issued in 2019,5 which included “equality of opportunity by gender”, “establish systems and mentoring programs that support career flexibility”, and “eliminate implicit biases”. It is suggested that these efforts to increase the number of female cardiologists will eventually lead to reduced inequality between male and female cardiologists. In addition, it has been reported that the acceptance rate of chairperson designations increases among male cardiologists when there are more female cardiologists at their institutions.18 Diverse workplaces with a high proportion of female employees may reflect situations that foster opportunities and encouragement for career advancement. In Japan, the distribution of female cardiologists is concentrated in Tokyo, and is higher in western Japan and lower in eastern Japan for all cardiologists. Analysis by the number of cardiologists per population in each prefecture shows that both men and women have no differences in their preferences for studying abroad. It is estimated that the high percentage of female cardiologists contributes to the enhancement of career development among cardiologists, generally. However, in rural areas with small populations, female cardiologists are less likely to prefer studying abroad. It is not clear why, although one possible reason is that few female cardiologists around them have studied abroad.
Importance of Mentors
Those who did not have mentors were more likely to feel inequality and less likely to be satisfied with their work or have a preference for studying abroad. These results are striking and suggest that the presence of mentors is important. Mentors are reportedly associated with positive outcomes regarding behavior, attitudes, health-related effects, and career development in a variety of settings, including educational settings and the workplace,20 and promoting and maintaining a sense of fulfillment in medical settings.21
Two major aspects of a mentor’s role have been described: the career and psychosocial aspect.22 The career role includes sponsorship, coaching, protection, and providing challenging assignments. The presence of a mentor exposes one to educational and social opportunities, develops new relationships, and increases the willingness to seek new experiences by opening one’s eyes to various possibilities. This may be the reason why those who have a mentor expressed a preference for studying abroad. Regarding the psychosocial role of a mentor, the mentor may listen to the mentee in times of stress, offer advice, and provide counseling on personal and work issues, which may play a crucial role in reducing inequality and increasing work satisfaction. In recent years, with the COVID-19 pandemic, face-to-face connections and opportunities for daily social interactions in the workplace have diminished,23 and deep and candid interactions, such as a good mentor-mentee relationship, are more desired than before. To find mentors for young cardiologists, the construction of network systems, such as mentor–mentee matching on a large scale is awaited.
Study Limitations
Those who responded to the questionnaire may have had a greater interest in a cardiologist’s career development than those who did not, which may differ from the usual population within an academic society. Awareness of inequality in career development was a perception of the cardiologists, and may not indicate the actual inequality in the working environment. A prospective study of a cardiologist’s desired plan and career change in cardiology may be required to research the actual inequality in the environment.
Conclusions
Female and younger cardiologists felt more inequality with regard to training opportunities and lower work satisfaction. A perception of inequality was higher among those with family care duties and those without a mentor. Male cardiologists perceived less inequality of opportunities as the number of female cardiologists increased, indicating that workplace diversity may lead to equality in training opportunities. In addition, increasing the number of mentors may be the most important thing for both female and male doctors in Japan to find happiness and ambition in their work.
Acknowledgments
The authors acknowledge the members of the JCS who cooperated with this survey, members of the Committee for Diversity Promotion of the JCS, and the JCS-JJC Subcommittee. The authors express their heartfelt gratitude to the JCS office for the administrative work performed to undertake this survey. Finally, the authors gratefully acknowledge the significant contributions of all cardiologists who have been dedicated to promoting diversity from the past to the present, globally.
Disclosures
T.I., H.I., and Y.K. are members of Circulation Journal’s Editorial Team. M.S. belongs to a department endowed by HIMEDIC Inc. and Siemens Healthcare K.K.; however, this status has no bearing on the contents of the paper.
IRB Information
The present study was approved by the JCS Ethics Committee (Reference no. 15).
Data Availability
The deidentified participant data will not be shared.
Supplementary Files
Please find supplementary file(s);
https://doi.org/10.1253/circj.CJ-23-0063
References
- 1.
Ministry of Health, Labor and Welfare, Japan. 2020 Statistics of physicians, dentists and pharmacists [in Japanese]. https://www.mhlw.go.jp/toukei/saikin/hw/ishi/20/dl/R02_kekka-1.pdf (accessed November 19, 2022).
- 2.
Mehta LS, Fisher K, Rzeszut AK, Lipner R, Mitchell S, Dill M, et al. Current demographic status of cardiologists in the United States. JAMA Cardiol 2019; 4: 1029–1033.
- 3.
Yong CM, Abnousi F, Rzeszut AK, Douglas PS, Harrington RA, Mehran R, et al. Sex differences in the pursuit of interventional cardiology as a subspecialty among cardiovascular Fellows-in-training. JACC Cardiovasc Interv 2019; 12: 219–228.
- 4.
About the Japanese Circulation Society [in Japanese]. https://www.j-circ.or.jp/about/ (accessed November 19, 2022).
- 5.
Sharma G, Sarma AA, Walsh MN, Hayes SN, Sahni S, Brown SA, et al. 10 recommendations to enhance recruitment, retention, and career advancement of women cardiologists. J Am Coll Cardiol 2019; 74: 1839–1842.
- 6.
Otaki J. Considering primary care in Japan. Acad Med 1998; 73: 662–668.
- 7.
Population by age group in the Basic Resident Register as of January 1, 2022 (by prefecture) [in Japanese]. https://www.soumu.go.jp/main_sosiki/jichi_gyousei/daityo/jinkou_jinkoudoutai-setaisuu.html (accessed December 5, 2022).
- 8.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48: 452–458.
- 9.
Distribution of members in Japan Circulation Society [in Japanese]. https://www.j-circ.or.jp/senmoni_kensaku/ (accessed December 13, 2022).
- 10.
Khan MS, Mahmood S, Khan SU, Fatima K, Khosa F, Sharma G, et al. Women training in cardiology and its subspecialties in the United States: A decade of little progress in representation. Circulation 2020; 141: 609–611.
- 11.
Kono E, Isozumi U, Nomura S, Okoshi K, Yamamoto H, Miyata H, et al. Surgical experience disparity between male and female surgeons in Japan. JAMA Surg 2022; 157: e222938, doi:10.1001/jamasurg.2022.2938.
- 12.
Yang Y, Li J, Wu X, Wang J, Li W, Zhu Y, et al. Factors influencing subspecialty choice among medical students: A systematic review and meta-analysis. BMJ Open 2019; 9: e022097.
- 13.
Reza N, Krishnan S, Adusumalli S. A Model for the Career Advancement of Women Fellows and cardiologists. J Am Coll Cardiol 2020; 76: 996–1000.
- 14.
Rampersad PP, Capdeville M. Who decided cardiology was a man’s job?: The future of cardiovascular medicine and why women are key. J Cardiothorac Vasc Anesth 2020; 34: 575–581.
- 15.
Tsukada YT, Tokita M, Kato K, Kato Y, Miyauchi M, Ono I, et al. Solutions for retention of female cardiologists: From the survey of gender differences in the work and life of cardiologists. Circ J 2009; 73: 2076–2083.
- 16.
Kohlfurst DS, Zoggeler T, Karall D, Kerbl R. Workload and job satisfaction among Austrian pediatricians: Gender and generational aspects. Wien Klin Wochenschr 2022; 134: 516–521.
- 17.
Obara H, Saiki T, Imafuku R, Fujisaki K, Suzuki Y. Influence of national culture on mentoring relationship: A qualitative study of Japanese physician-scientists. BMC Med Educ 2021; 21: 300.
- 18.
Nakayama A, Kamiya CA, Kanki S, Ide T, Bando YK, Uemura Y, et al. Awareness and feasibility of women chairing cardiology sessions in scientific meetings: A nationwide survey by the Japanese Circulation Society. Front Cardiovasc Med 2022; 9: 871546.
- 19.
Nomura K, Gohchi K. Impact of gender-based career obstacles on the working status of women physicians in Japan. Soc Sci Med 2012; 75: 1612–1616.
- 20.
Eby LT, Allen TD, Evans SC, Ng T, DuBois D. Does mentoring matter? A multidisciplinary meta-analysis comparing mentored and non-mentored individuals. J Vocat Behav 2008; 72: 254–267.
- 21.
Darves B. Physician mentorship: Why it’s important, and how to find and sustain relationships. NEJM Career Center; 2018. https://resources.nejmcareercenter.org/article/physician-mentorship-why-its-important-and-how-to-find-and-sustain-relationships/ (accessed December 13, 2022).
- 22.
Day R, Allen TD. The relationship between career motivation and self-efficacy with protégé career success. J Vocat Behav 2004; 64: 72–91.
- 23.
Both LM, Zoratto G, Calegaro VC, Ramos-Lima LF, Negretto BL, Hauck S, et al. COVID-19 pandemic and social distancing: Economic, psychological, family, and technological effects. Trends Psychiatry Psychother 2021; 43: 85–91.