Images in Cardiovascular Medicine
Multimodality Imaging for the Diagnosis of Primary Pericardial Angiosarcoma
2023 Volume 87 Issue 9 Pages 1250-

Details
2023 Volume 87 Issue 9 Pages 1250-
A 36-year-old woman presented with syncope, chest pain, and dyspnea. At a local hospital, 40 days before admission, transthoracic echocardiography (TTE) revealed massive pericardial effusion (Figure A) and 4 days before admission, she underwent percutaneous drainage of bloody pericardial fluid; however, her symptoms were not relieved. Culture and cytology of the pericardial fluid were negative. On admission, repeat TTE showed an irregular, hypoechoic, immobile mass (49×22 mm) in the right pericardium with effusion (Figure B). Contrast echocardiography indicated complete enhancement of contrast agent in the mass (Figure C), suggesting it was malignant. 18F-fluorodeoxy glucose-positron emission tomography (18F-FDG PET)/computed tomography (CT) revealed abnormal fluorodeoxyglucose activity in multiple areas, as well as in the right atrium (RA), aortic arch and aortic root, with maximum standardized uptake values of 5.2, 4.6, and 3.8 respectively (Figure D–H). Cardiac magnetic resonance imaging (MRI) confirmed soft tissue masses in the right pericardium attached to the RA, aortic arch and aortic root (Figure I,K). 18F-FDG PET/MRI also showed intense fluorodeoxyglucose uptake in these masses (Figure J,L). The combination of these imaging findings led to a high index of suspicion for primary pericardial angiosarcoma. Considering the absence of other organ metastasis, the patient underwent surgical excision of the tumor and reconstruction of the RA (Figure M). Histopathological examination showed fibrinous necrotic material containing epithelioid cells with nuclear hyperchromatism (Figure N) with positive immunohistochemistry for Ki-67 (Figure O), CD34 (Figure P), Erg (Figure Q), and F8 (Figure R), which confirmed angiosarcoma.
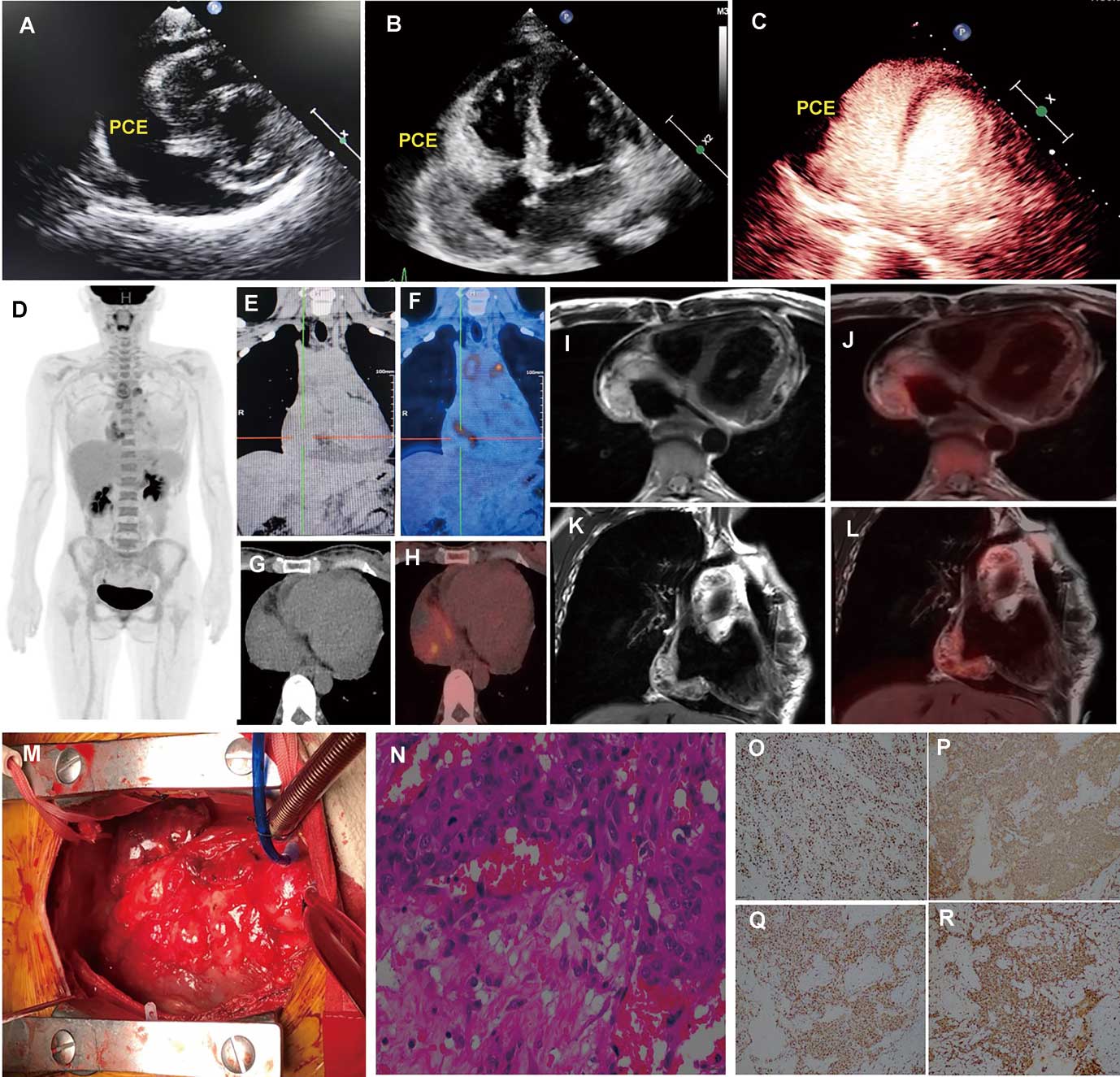
Transthoracic (A,B) and contrast echocardiography (C). MIP (D) and chest images (CT: E–G; fusion: F–H) of 18F-fluorodeoxy glucose (18F-FDG). 18F-FDG PET/MRI (I–L). Intraoperative image (M). Histopathology (H&E: N; immunohistochemistry: O–R). CT, computed tomography; MRI, magnetic resonance imaging; PCE, pericardial effusion; PET, positron emission tomography.
Primary pericardial angiosarcoma is extremely rare, but shows rapid progression. This case highlights the importance of multimodality imaging for accurate diagnosis and appropriate surgical planning.
We acknowledge assistance from the National Natural Science Foundation of China (82071933; 82260350), and the Science and Technology Committee Foundation of Shanghai (20JC1418400; 20Y11912000).