Abstract
Background: The mechanism underlying a poor prognosis in patients with lower-extremity artery disease (LEAD) with heart failure is unknown. We examined the prognostic impact of the left ventricular ejection fraction (LVEF) in patients with LEAD who underwent endovascular therapy (EVT).
Methods and Results: From August 2014 to August 2016, 2,180 patients with LEAD (mean age, 73.2 years; male, 71.9%) underwent EVT and were stratified into low-LVEF (LVEF <40%; n=234, 10.7%) and not-low LVEF groups. In the low- vs. not-low LVEF groups, there was a higher prevalence of heart failure (i.e., history of heart failure hospitalization or New York Heart Association functional class III or IV symptoms) (44.0% vs. 8.3%, respectively), diabetes mellitus, chronic kidney disease, below-the-knee lesion, critical limb ischemia, and incidence of major cardiovascular and cerebrovascular events (MACCEs) and major adverse limb events (MALEs) (P<0.001, all). Low LVEF independently predicted MACCEs (hazard ratio: 2.23, 95% confidence interval: 1.63–3.03; P<0.001) and MALEs (hazard ratio: 1.85, 95% confidence interval: 1.15–2.96; P=0.011), regardless of heart failure (P value for interaction: MACCEs: 0.27; MALEs: 0.52).
Conclusions: Low LVEF, but not symptomatic heart failure, increased the incidence of MACCEs and MALEs. Intensive cardiac dysfunction management may improve LEAD prognosis after EVT.
The incidence of heart failure, as a major cause of death and progressive functional limitation, is increasing worldwide.1–5 Heart failure is a complex clinical syndrome caused by structural and functional impairment of ventricular filling or ejection, and can manifest as dyspnea, malaise, swelling, and/or decreased exercise capacity.6,7 The incidence of lower-extremity artery disease (LEAD) is also increasing,8 and it often manifests as polyvascular disease with an associated elevated risk of both functional deterioration and cardiovascular death,9–13 usually attributable to atherosclerosis. LEAD shares risk factors and pathophysiological features with cardiovascular disease, including heart failure,14–16 and these 2 conditions often coexist.17 Heart failure is recognized only when it becomes symptomatic, by definition; however, asymptomatic stages of structural heart disease exist, corresponding to Stage B (pre-heart failure: structural and functional abnormalities without symptoms) under the staging system of current major guidelines. Heart failure prevalence and mortality rates are high in patients with LEAD,16,18–20 and decreased patency after endovascular therapy (EVT)21 occurs in patients with both conditions. In most studies, patients with symptomatic heart failure (Stages C and D) are considered to have heart failure; however, whether heart failure itself contributes to the poor prognosis or whether other factors that promote heart failure development affect clinical outcomes is undetermined. Among the factors contributing to heart failure development, left ventricular dysfunction is the leading cause and the most important factor in determining the heart failure monitoring and treatment strategy.6,7,22–24 Current guidelines describe 3 heart failure categories: heart failure with reduced ejection fraction (HFrEF), heart failure with mildly reduced ejection fraction (HFmrEF), and heart failure with preserved ejection fraction (HFpEF) based on the left ventricular ejection fraction (LVEF).6,7,22–24 Early intervention for asymptomatic heart failure is recommended, especially if patients have structural heart disease with reduced LVEF.6,7 Therefore, in the present study, we evaluated LVEF and investigated its prognostic impact and the independent predictors of clinical outcomes in Japanese patients with LEAD undergoing EVT using data from an all-comer prospective registry cohort of Japanese patients with LEAD.
Methods
Study Design and Population
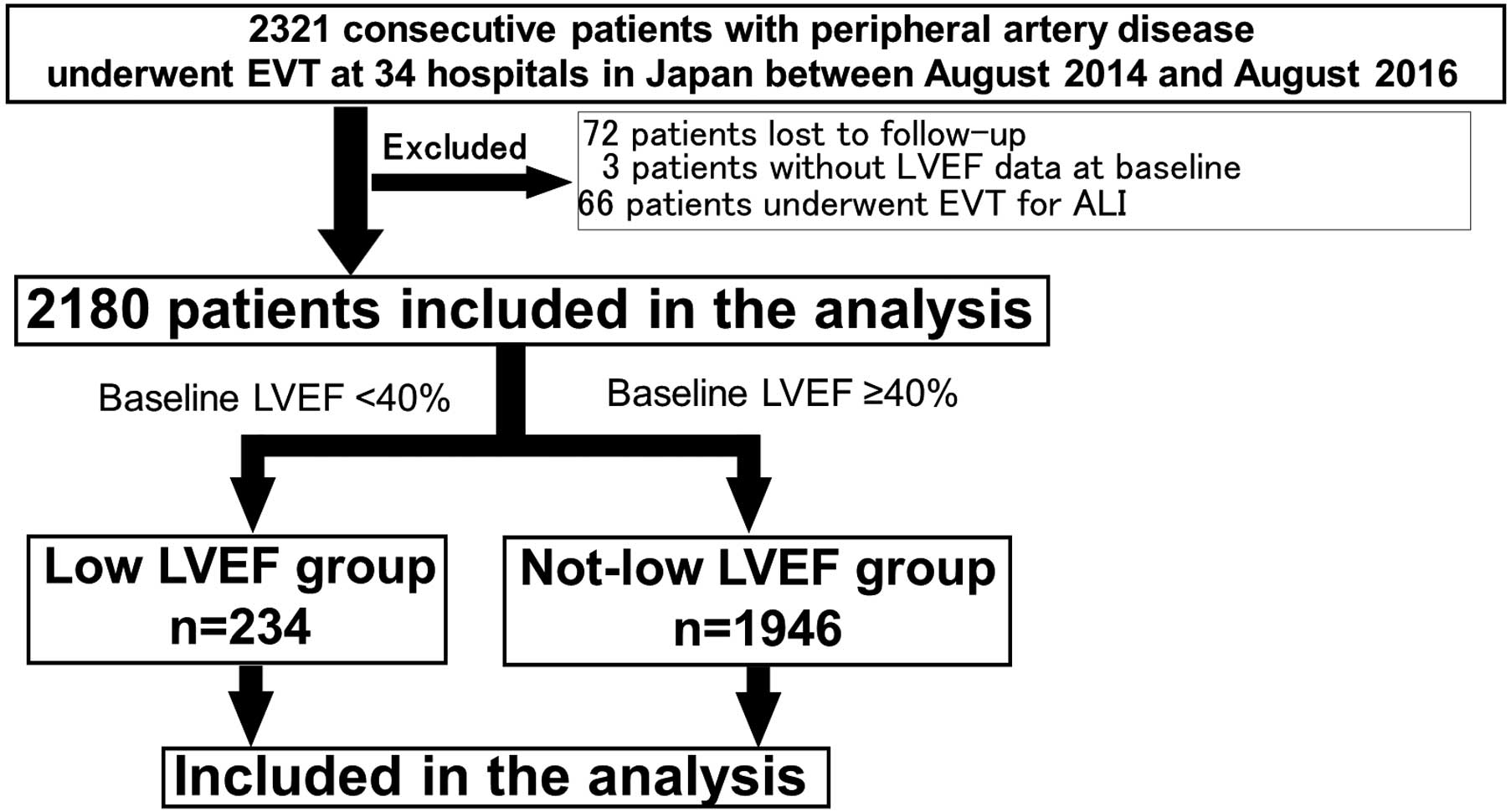
The design and primary results of the TOkyo taMA peripheral vascular intervention research COmraDE (Toma-Code) study, a Japanese prospective cohort study of consecutive patients with LEAD who underwent EVT for all indications from August 2014 to August 2016, have been published.25 From it we identified 2,180 patients who were eligible for inclusion in the present analysis (Figure 1). The mean age was 73.2 years (1,568 men [71.9%]). We divided the patients into 2 groups by LVEF on admission. Low LVEF was defined as LVEF <40%,13,14,22 and not-low LVEF was defined as LVEF ≥40% on echocardiography. The method of measuring LVEF was at the attending physician’s discretion. Data were collected as categorical data, not exact LVEF values, to categorize patients into the low-LVEF or not-low-LVEF group at registry enrollment.
Data Collection, Follow-up, and Comorbidity Definitions
Clinical data were collected from the patients’ medical records or from the database by independent researchers using predetermined definitions. The study office collectively managed all data. The follow-up data were obtained from hospital charts or by contacting the patients or their family members via telephone at 1, 6, 12, 18, and 24 months after EVT.
Outcome Measures
The major outcome measures were major adverse cardiovascular and cerebrovascular events (MACCEs: composite of all-cause death, cardiovascular death, myocardial infarction, and stroke), and major adverse limb events (MALEs: composite of major amputation, acute limb ischemia, surgical intervention, and unscheduled EVT), based on the registry’s prespecified definitions.25 The rates of each component of MACCEs and MALEs were also analyzed.
Definitions
Heart failure was defined as a history of heart failure hospitalization or New York Heart Association (NYHA) functional class III or IV symptoms. Cardiovascular death was a composite of sudden death and death caused by myocardial infarction, stroke, vascular disease, aortic disease, arrhythmia, heart failure, and valvular disease. Heart failure death as part of cardiovascular death was recorded when the attending physician reported the cause of death as heart failure. Myocardial infarction was defined as significantly elevated serum biomarkers (troponin T >0.1 μg/L or creatinine kinase twice normal) or new Q waves on ECG. “Stroke” was a cerebral stroke persisting ≥24 h with neurological deficits. Major amputation was amputation above the ankle. Acute limb ischemia was a sudden decrease in limb perfusion that threatened limb viability and presented within 2 weeks after symptom onset. Surgical intervention was a composite of bypass grafting, thrombectomy, and endarterectomy. Unscheduled EVT comprised all unplanned EVT required on the basis of the patient’s condition, regardless of the treatment procedure. Definitions of other comorbidities are shown in Supplementary Table 1. Critical limb ischemia (CLI) was defined as the presence of ischemic rest pain and ischemic lesions or gangrene objectively attributable to arterial occlusive disease.26 Current guidelines use the term chronic limb-threatening ischemia (CLTI) to better reflect the natural history of lower-extremity disease. CLTI indicates a wider spectrum of the most severe LEAD, including CLI; however, we used the term CLI because the data were collected as CLI.
Statistical Analysis
Continuous data are presented as mean±standard deviation when normally distributed or as median (interquartile range) when non-normally distributed, unless otherwise stated. The normality of continuous variables was analyzed using the Kolmogorov-Smirnov test. The low-LVEF and not-low-LVEF groups were compared using an unpaired Student’s t-test. Categorical data are expressed as percentages and absolute values and were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate. MACCEs and MALEs probabilities during follow-up were estimated using the Kaplan-Meier method. Differences between groups were assessed using the log-rank test. Cox multivariate analysis was used to determine the independent predictors of MACCEs and MALEs. Predictive factors that were statistically significant in the univariate analysis were included in the multivariate analysis. All statistical analyses were performed using R software (version 4.1.2; “tableone” and “RcmdrPlugin. EZR” packages).27 All tests were two-tailed, and P<0.05 was considered statistically significant.
Ethical Considerations
The Toma-Code registry study was approved by the institutional review board of Sakakibara Heart Institute, the core center of this multicenter study (reference no. 14-023), and the committees of each participating facility. The study is registered in the University Hospital Medical Information Network-Clinical Trials Registry (UMIN-CTR No. 000015100). All patients provided written informed consent for participation.
Results
Patient and Lesion Characteristics and Differences Between the Low- and Not-Low-LVEF Groups
The patients’ baseline characteristics and the differences between the low- and not-low-LVEF groups are shown in Table 1. Among the 2,180 patients who underwent EVT, 234 (10.7%) were allocated to the low-LVEF group (LVEF <40%). The mean age was higher in the not-low vs. low-LVEF groups (73.3±9.2 vs. 71.8±9.1 years, respectively; P=0.03). The proportion of patients with difficulty walking was significantly higher in the low- vs. not-low-LVEF groups (P<0.001). Comparatively, the prevalence of diabetes mellitus (P<0.001), chronic kidney disease (P<0.001), dialysis (P<0.001), chronic obstructive pulmonary disease (P=0.01), and heart failure (P<0.001) was significantly higher in the low-LVEF group; hypertension was more frequent in the not-low-LVEF group (P=0.001). Coronary artery disease (P<0.001) and aortic valve stenosis (P=0.001) were also more prevalent in the low- vs. not-low-LVEF groups. Below-the-knee lesion intervention and CLI were significantly more frequent in the low- vs. not-low-LVEF groups, respectively (below-the-knee lesions: 36.3% vs. 22.3%, P<0.001; CLI: 61.5% vs. 44.1%, P<0.001). The prevalence of chronic total occlusion and lesion length did not differ significantly between the groups. The serum albumin concentration was significantly lower (P<0.001), and inflammatory markers, such as white blood cell count and C-reactive protein concentrations, were significantly higher in the low- vs. not-low-LVEF groups (white blood cell count: P=0.02; C-reactive protein concentration: P<0.001). Regarding the nutritional risk status evaluated by the geriatric nutritional risk index (GNRI), the prevalence of those at major nutritional risk was significantly higher in the low- vs. not-low-LVEF groups, respectively (GNRI: 95.2±13.6 vs. 99.6±12.6, P<0.001; prevalence: 15.0% vs. 7.0%, P<0.001).
Table 1.
Baseline Characteristics of the Patients
| Variables |
Not-low LVEF
(n=1,946) |
Low LVEF
(n=234) |
P value |
| Age |
73.3±9.2 |
71.8±9.1 |
0.03 |
| Male sex |
1,379 (70.9) |
189 (80.8) |
0.002 |
| Body mass index (kg/m2) |
22.6±3.6 |
21.8±3.4 |
0.001 |
| Ankle-brachial index |
0.68±0.18 |
0.69±0.20 |
0.44 |
| Ambulation difficulty |
163 (8.4) |
42 (17.9) |
<0.001 |
| Lower-extremity symptoms (Rutherford category) |
|
|
<0.001 |
| Claudication (I–III) |
1,088 (55.9) |
90 (38.5) |
|
| Ischemic pain at rest (IV) |
317 (16.3) |
34 (14.5) |
|
| Minor tissue loss (V) |
445 (22.9) |
79 (33.8) |
|
| Major tissue loss (VI) |
94 (4.8) |
31 (13.2) |
|
| Smoking habit |
1,133 (58.2) |
146 (62.4) |
0.25 |
| Comorbidity |
| Diabetes mellitus |
1,085 (55.8) |
159 (67.9) |
<0.001 |
| Hypertension |
1,637 (84.2) |
177 (75.6) |
0.001 |
| Dyslipidemia |
1,134 (58.3) |
135 (57.7) |
0.92 |
| Chronic kidney disease |
827 (42.5) |
151 (64.5) |
<0.001 |
| Dialysis |
491 (25.2) |
107 (45.7) |
<0.001 |
| Chronic obstructive pulmonary disease |
71 (3.6) |
17 (7.3) |
0.01 |
| Heart failure |
161 (8.3) |
103 (44.0) |
<0.001 |
| Aortic valve stenosis |
36 (1.8) |
13 (5.6) |
0.001 |
| Coronary artery disease |
867 (44.6) |
185 (79.1) |
<0.001 |
| Cerebrovascular disease |
284 (14.6) |
37 (15.9) |
0.67 |
| Atrial fibrillation |
185 (9.5) |
34 (14.5) |
0.02 |
| Spinal canal stenosis |
102 (5.2) |
10 (4.3) |
0.63 |
| Inflammatory disease |
60 (3.1) |
3 (1.3) |
0.18 |
| History of lower-extremity intervention |
| History of major amputation |
59 (3.0) |
11 (4.7) |
0.24 |
| History of lower-extremity bypass surgery |
68 (3.5) |
13 (5.6) |
0.16 |
| History of lower-extremity EVT |
424 (21.8) |
59 (25.2) |
0.27 |
| Medication and treatment |
| Aspirin |
1,344 (69.3) |
185 (79.7) |
0.001 |
| Thienopyridine |
1,326 (68.4) |
165 (71.1) |
0.44 |
| Cilostazol |
773 (39.9) |
66 (28.4) |
0.001 |
| Eicosapentaenoic acid |
177 (9.1) |
15 (6.5) |
0.22 |
| Oral anticoagulants |
309 (15.9) |
43 (18.5) |
0.36 |
| ACEI or ARB |
1,063 (54.6) |
109 (46.6) |
0.02 |
| β-blocker |
535 (27.6) |
132 (56.9) |
<0.001 |
| Calcium-channel blocker |
1,037 (53.5) |
66 (28.4) |
<0.001 |
| Statin |
996 (51.4) |
132 (56.9) |
0.13 |
| Insulin |
357 (18.4) |
66 (28.2) |
<0.001 |
| Procedure-related variables |
| Stent implantation |
1,218 (62.6) |
123 (52.6) |
0.004 |
| Treated lesion |
| Bilateral lesion |
220 (11.3) |
23 (9.8) |
0.57 |
| Iliac |
716 (36.8) |
73 (31.2) |
0.11 |
| Femoropopliteal |
1,259 (64.7) |
142 (60.7) |
0.25 |
| Below-the-knee |
433 (22.3) |
85 (36.3) |
<0.001 |
| Graft |
6 (0.3) |
1 (0.4) |
1.00 |
| Disease and lesion characteristics |
| Critical limb ischemia |
858 (44.1) |
144 (61.5) |
<0.001 |
| Chronic total occlusion |
881 (45.3) |
111 (47.4) |
0.58 |
| Lesion length (mm) |
100 [40, 230] |
100 [45, 260] |
0.09 |
| Laboratory data |
| White blood cell count (109/L) |
7.07±2.69 |
7.54±3.92 |
0.02 |
| Hemoglobin (g/L) |
127±103 |
119±21 |
0.25 |
| Platelet count (109/L) |
22.6±11.0 |
20.2±6.8 |
0.001 |
| Albumin (g/L) |
39.0±6.0 |
37.0±7.0 |
<0.001 |
| Total cholesterol (mmol/L) |
4.47±1.01 |
4.22±1.19 |
<0.001 |
| Triglyceride (mmol/L) |
1.54±1.02 |
1.45±1.25 |
0.20 |
| Aspartate aminotransferase (IU/L) |
19 [15, 24] |
18 [14, 24] |
0.29 |
| Alanine aminotransferase (IU/L) |
14 [10, 20] |
12 [9, 20] |
0.03 |
| Lactate dehydrogenase (IU/L) |
200±53 |
204±71 |
0.33 |
| Creatine phosphokinase (IU/L) |
74 [50, 111] |
62.50 [40, 100] |
<0.001 |
| C-reactive protein (mg/L) |
2.5 [0.8, 8.7] |
6.9 [1.7, 21.7] |
<0.001 |
| Nutritional status and risk category |
| GNRI |
99.6±12.6 |
95.2±13.6 |
<0.001 |
| Nutritional risk category |
|
|
<0.001 |
| Major risk (GNRI <82) |
136 (7.0) |
35 (15.0) |
|
| Moderate risk (GNRI ≥82 to <92) |
274 (14.1) |
52 (22.2) |
|
| Low risk (GNRI ≥92 to <98) |
306 (15.7) |
35 (15.0) |
|
| No risk (GNRI ≥98) |
1,230 (63.2) |
112 (47.9) |
|
Data are presented as the mean±standard deviation (normally distributed continuous data), or the median [interquartile range] (non-normally distributed data), or n (%). Groups were compared using an unpaired Student’s t-test. Categorical data are expressed as percentages and absolute values and were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; EVT, endovascular therapy; GNRI, Geriatric Nutritional Risk Index; LVEF, left ventricular ejection fraction.
Clinical Outcomes
Incidence of Major Outcome Measures and Survival Analysis The 2-year cumulative incidences of MACCEs and MALEs were significantly higher in the low- vs. not-low-LVEF groups, respectively (MACCEs: 23.9% vs. 9.9%, P<0.001; MALEs: 9.8% vs. 4.8%, P<0.001). The freedom from MACCEs and MALEs survival rates are shown in Figure 2. The MACCEs- and MALEs-free survival rates were significantly lower in the low- vs. not-low-LVEF groups (P<0.001 for both). For both MACCEs and MALEs, the survival curves were significantly stratified by LVEF status throughout the observation period.
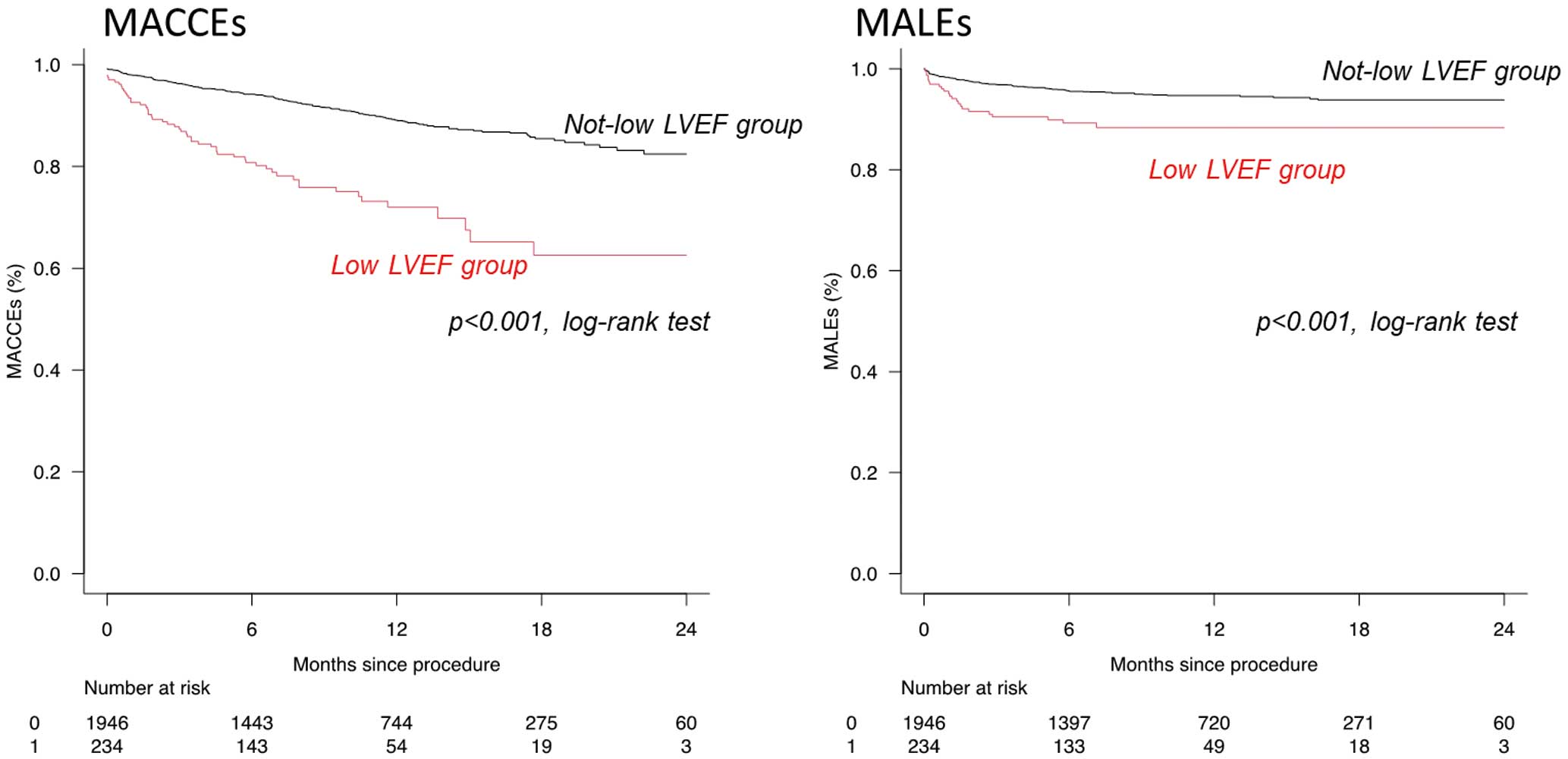
Table 2 shows the contribution of each component to the major outcome measures. Both all-cause death and cardiovascular death were significantly more frequent in the low- vs. not-low-LVEF groups (hazard ratio [HR]: 3.29, 95% confidence interval [CI]: 2.40–4.52, P<0.001; HR: 5.03, 95% CI: 2.98–8.50, P<0.001, respectively). Regarding cardiovascular death, the risk of heart failure death was significantly higher in the low- vs. not-low-LVEF groups (HR: 9.15, 95% CI: 4.34–19.3; P<0.001). Regarding MALEs, major amputation was significantly more frequent in the low- vs. not-low-LVEF groups (HR: 2.90, 95% CI: 1.63–5.17; P<0.001). The incidence of clinically driven target lesion revascularization was not significantly different between the groups; however, the risk of unscheduled EVT was almost 1.6-fold higher in the low- vs. not-low-LVEF groups (HR: 1.59, 95% CI: 1.10–2.29; P=0.014).
Table 2.
Contribution of Each Component to MACCEs and MALEs
| Population |
No. of patients (%) |
Not-low LVEF
vs. low LVEF
HR (95% CI) |
P value |
Not-low LVEF
(n=1,946) |
Low LVEF
(n=234) |
| MACCEs |
193 (9.9) |
56 (23.9) |
2.98 (2.21–4.02) |
<0.001 |
| All-cause death |
161 (8.3) |
51 (21.8) |
3.29 (2.40–4.52) |
<0.001 |
| Bleeding death |
5 (0.3) |
1 (0.4) |
1.81 (0.21–15.5) |
0.588 |
| Cardiovascular death |
43 (2.2) |
21 (9.0) |
5.03 (2.98–8.50) |
<0.001 |
| Heart failure death |
15 (0.8) |
13 (5.6) |
9.15 (4.34–19.3) |
<0.001 |
| Non-fatal MI |
17 (0.9) |
3 (1.3) |
1.80 (0.53–6.15) |
0.349 |
| Non-fatal stroke |
31 (1.6) |
4 (1.7) |
1.29 (0.46–3.66) |
0.631 |
| MALEs |
93 (4.8) |
23 (9.8) |
2.38 (1.51–3.76) |
<0.001 |
| Major amputation |
50 (2.6) |
15 (6.4) |
2.90 (1.63–5.17) |
<0.001 |
| Acute limb ischemia |
16 (0.8) |
1 (0.4) |
0.61 (0.08–4.60) |
0.631 |
| Clinically driven TLR |
349 (17.9) |
43 (18.4) |
1.30 (0.94–1.78) |
0.108 |
| Surgical reintervention |
38 (2.0) |
8 (3.4) |
2.03 (0.94–4.35) |
0.070 |
| Unscheduled EVT |
216 (11.1) |
33 (14.1) |
1.59 (1.10–2.29) |
0.014 |
CI, confidence interval; EVT, endovascular therapy; HR, hazard ratio; LVEF, left ventricular ejection fraction; MACCEs, major adverse cardiovascular and cerebrovascular events; MALEs, major adverse limb events; MI, myocardial infarction; TLR, target lesion revascularization.
Predictors of MACCEs and MALEs
Table 3 shows the results of the multivariate Cox proportional hazards analysis of MACCEs and MALEs. Low LVEF was an independent predictor of both MACCEs and MALEs, even after covariate adjustment (MACCEs: HR: 2.23, 95% CI: 1.63–3.03, P<0.001; MALEs: HR: 1.85, 95% CI: 1.15–2.96, P=0.011). CLI was also significantly associated with both MACCEs and MALEs. Diabetes mellitus, atrial fibrillation, and chronic kidney disease were significantly associated with MACCEs, but not with MALEs.
Table 3.
Multivariate Cox Proportional Hazards Regression Analysis of MACCEs and MALEs
| Variables |
Univariate |
Multivariate |
| HR |
95% CI |
P value |
HR |
95% CI |
P value |
| MACCEs |
| Low LVEF |
2.98 |
2.21–4.02 |
<0.001 |
2.23 |
1.63–3.03 |
<0.001 |
| Male sex |
0.74 |
0.57–0.97 |
0.026 |
0.96 |
0.73–1.26 |
0.743 |
| Diabetes mellitus |
1.42 |
1.10–1.85 |
0.008 |
1.38 |
1.04–1.82 |
0.025 |
| Hypertension |
0.65 |
0.48–0.88 |
0.005 |
0.83 |
0.61–1.13 |
0.233 |
| Body mass index |
0.87 |
0.84–0.90 |
<0.001 |
0.90 |
0.87–0.94 |
<0.001 |
| Stent implantation |
0.59 |
0.46–0.76 |
<0.001 |
0.88 |
0.68–1.14 |
0.327 |
| Atrial fibrillation |
2.00 |
1.43–2.78 |
<0.001 |
1.56 |
1.11–2.19 |
0.011 |
| Age per 5-year age group |
1.17 |
1.09–1.26 |
<0.001 |
1.14 |
1.06–1.23 |
<0.001 |
| Chronic kidney disease |
3.15 |
2.40–4.12 |
<0.001 |
2.15 |
1.62–2.85 |
<0.001 |
| Critical limb ischemia |
4.53 |
3.37–6.08 |
<0.001 |
2.77 |
2.02–3.80 |
<0.001 |
| MALEs |
| Low LVEF |
2.38 |
1.51–3.76 |
<0.001 |
1.85 |
1.15–2.96 |
0.011 |
| Male sex |
0.59 |
0.41–0.86 |
0.006 |
0.63 |
0.43–0.93 |
0.019 |
| Diabetes mellitus |
1.57 |
1.06–2.31 |
0.023 |
1.16 |
0.77–1.75 |
0.483 |
| Hypertension |
0.59 |
0.39–0.90 |
0.015 |
0.89 |
0.57–1.39 |
0.609 |
| Body mass index |
0.91 |
0.86–0.96 |
0.001 |
0.93 |
0.88–0.98 |
0.006 |
| Stent implantation |
0.47 |
0.32–0.67 |
<0.001 |
0.72 |
0.49–1.06 |
0.099 |
| Atrial fibrillation |
1.63 |
0.98–2.73 |
0.062 |
|
|
|
| Age per 5-year age group |
0.85 |
0.78–0.93 |
<0.001 |
0.84 |
0.77–0.92 |
<0.001 |
| Chronic kidney disease |
2.27 |
1.56–3.31 |
<0.001 |
1.34 |
0.90–2.00 |
0.153 |
| Critical limb ischemia |
5.63 |
3.54–8.96 |
<0.001 |
3.92 |
2.39–6.42 |
<0.001 |
Estimated hazard ratios and associated confidence intervals were obtained using a Cox proportional hazards regression model for an interaction between the low LVEF group and the not-low LVEF group. Abbreviations as in Table 2.
To adjust the baseline imbalance between the groups, we used inverse probability of treatment weighting (IPTW). Propensity scores were calculated using factors with significant differences between the groups, excluding factors that correlated with each other and factors that could contain extreme outliers, in accordance with the characteristics of this method. The selected factors are shown in Supplementary Table 2A. Low LVEF was significantly associated with MALEs (HR: 2.29, 95% CI: 1.17–4.49; P=0.016), and the same tendency was observed with MACCEs (HR: 1.51, 95% CI: 0.94–2.39; P=0.082). Supplementary Figure shows the weighted survival estimates for event-free survival and Supplementary Table 2B shows the Cox proportional hazards analysis of each component.
Potential Modification of the Association Between LVEF Status and Outcome Measures by Demographics and Comorbidities
To explore the potential modification by demographics and comorbidities, the associations between low LVEF and MACCEs (Figure 3A) and MALEs (Figure 3B) were analyzed in patient subgroups divided by comorbidities, including heart failure. Only oral anticoagulant intake significantly modified the association between low LVEF and MACCEs. In contrast, the association between low LVEF and MALEs was significantly modified by the presence of diabetes mellitus and chronic kidney disease. Low LVEF was more strongly associated with MALEs in patients with vs. without diabetes mellitus (HR: 3.21, 95% CI: 1.96–5.27 vs. HR: 0.34, 95% CI: 0.05–2.45, respectively; P for interaction=0.03). Patients with vs. without chronic kidney disease tended to have a stronger association between low LVEF and MALEs (HR: 2.72, 95% CI: 1.64–4.53 vs. HR: 0.67, 95% CI: 0.16–2.78, respectively; P for interaction=0.07). However, the presence of heart failure did not affect the association between low LVEF and MALEs (P for interaction=0.52). GNRI status did not modify the association between low LVEF and MACCEs or MALEs (P for interaction, MACCEs: 0.12; MALES: 0.62).

Discussion
In this study of patients with LEAD who underwent EVT, low LVEF significantly increased the risk of MACCEs and MALEs, regardless of the presence of symptomatic heart failure. Our results indicate that low LVEF affects the clinical outcomes of patients with LEAD after EVT, which suggests a potential role of the hemodynamic changes caused by left ventricular dysfunction, independent of heart failure symptoms, in LEAD development and progression.
LEAD often coexists with heart failure, which increases the risk of death.28–32 In our study, 10.7% of the patients had low LVEF and were more likely to have coronary artery disease, diabetes mellitus, chronic kidney disease, and atrial fibrillation, which are common and major risk factors for heart failure and atherosclerosis; each condition has a different effect on the incidence of cardiovascular and limb events. Diabetes mellitus, atrial fibrillation, and chronic kidney disease were independent predictors of MACCEs, but not MALEs. However, these findings may suggest that the presence of factors that modify the influence of the atherosclerotic burden on each vascular bed, and more complicated mechanisms other than atherosclerosis should be considered to understand LEAD progression.
Heart failure did not affect the association between low LVEF and MACCEs (P for interaction: 0.27) or MALEs (P for interaction: 0.52). Previous studies have reported an association between heart failure and reduced primary patency or an increased risk of amputation after EVT.33,34 However, a recent study suggested that heart failure is associated with higher mortality and cardiovascular event rates in the LEAD population, but not with limb event rates, despite the higher prevalence of severe LEAD in patients with vs. without heart failure.20 Furthermore, different types of heart failure may have different effects on limb events.19,21 Considering our results showing that low LVEF was associated with an increased incidence of MALEs, regardless of the presence of symptomatic heart failure, LVEF, rather than the heart failure itself, may be responsible for limb events after EVT. The definition of heart failure used in our study, which excluded those with NYHA class ≤II symptoms, was more severe than that used in previous reports.18,20,21 Nonetheless, our study failed to demonstrate an interaction of heart failure with the association between low LVEF and MALEs. This may suggest that limb patency after EVT is determined by the atherosclerotic burden as well as a complex combination of factors possibly resulting from left ventricular dysfunction. A previous report suggested that the association between heart failure and poor EVT durability is complex, and the poor prognosis of patients with heart failure after EVT may reflect the results of the subgroup of patients with systolic dysfunction.21 Our results may support this hypothesis, suggesting that the association between heart failure and limb events may be attributable to HFrEF.
In our population, low LVEF independently predicted MALEs, regardless of the presence of symptomatic heart failure. Changes in cardiac output in patients with heart failure provoke hemodynamic changes in the peripheral arteries and affect end-organ function.35 These findings suggest that ventricular dysfunction in heart failure, not heart failure itself, contributes to disease progression and increased limb events in patients with LEAD with heart failure. Our results suggest that hemodynamic changes caused by left ventricular dysfunction play a substantial role in the prognosis of patients with LEAD after EVT. Further studies of patients with LEAD stratified by LVEF with or without heart failure are needed.
Major guidelines have recommended treatment with the maximum tolerable dose of angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) alongside β-blockers as standard therapy for HFrEF because these agents improve the clinical outcomes of HFrEF.22–24 However, only 46.6% and 56.9% of the patients in our low-LVEF group were taking renin-angiotensin system inhibitors (ACEIs or ARBs) and β-blockers, respectively (Table 1). Although various issues may hinder the introduction of standard therapy for patients with heart failure, our results show that left ventricular dysfunction may be inadequately managed in patients with LEAD. This may be because LEAD and heart failure can mask the symptoms of each condition because of limited mobility, a common feature in heart failure and LEAD, leading to the under-recognition of both conditions.36 Historically, the management of coronary artery disease in patients with LEAD and concomitant coronary artery disease has been less intensive compared with that in patients with coronary artery disease only.37 Our results suggest that poor clinical outcomes in patients with LEAD with low LVEF may be partly attributable to suboptimal management of cardiovascular risk factors, including left ventricular dysfunction. Recently, there has been a paradigm shift in heart failure treatment based on the results of large-scale clinical trials, and guideline-directed medical therapy (GDMT) for heart failure has also changed.6,7,38 Evidence has emerged to support the use of new cardioprotective drugs. For example, angiotensin receptor-neprilysin inhibitors (ARNI) have shown survival-improving effects exceeding those of enalapril,39 and sodium-glucose cotransporter 2 (SGLT2) inhibitors lower the risk of cardiovascular death and heart failure hospitalization, regardless of the presence of diabetes mellitus.40–43 These drugs are included in the current GDMT, with β-blockers, mineralocorticoid receptor antagonists, and renin-angiotensin system inhibitors, traditionally ACEIs or ARBs, and now, ARNI, if tolerated.6,7,38 If the current GDMT had been introduced during our study, our results would have been different. However, more than half of the patients with reduced LVEF were not undergoing standard HFrEF treatment (Table 1). Insufficient implementation and early discontinuation of GDMT for heart failure have been reported,37,44–47 which should be overcome clinically.37,48 Although our data were collected in mid-2010 when ARNI and SGLT2 inhibitors were still not a Class I recommendation in major guidelines, published studies show that under-treatment, as noted in our study, remains a clinical issue. Reflecting the fact that low LVEF is a multifactorial condition, IPTW showed a non-significant P value (0.082) for the association between low LVEF and MACCEs. Therefore, our data may support the implementation of more intensive interventions for concomitant left ventricular dysfunction with multifactorial approaches to comorbidities in patients with LEAD, which may improve survival, cardiovascular outcomes, and limb-related outcomes after EVT.
Study Limitations
This study has several limitations. First, the data were collected between 2014 and 2016. Treatment guidelines for both LEAD and heart failure have since changed. GDMT for heart failure has markedly changed; therefore, if the patients had undergone current GDMT for concomitant heart failure, our results would have been different. Similarly, the concept of severe LEAD has changed from CLI to CLTI; however, our data were collected according to the conventional definition of CLI, which focuses on only lower-limb ischemic status. Therefore, our results may not fully apply to patients with CLTI according to the current definition. Second, this study involved only Japanese patients, and therefore the results may not be applicable to other ethnicities. Third, because of the definition of heart failure, patients with NYHA functional class ≤II symptoms, including asymptomatic patients corresponding to Stage B under current guidelines, were considered not to have heart failure. Fourth, the method of measuring LVEF was at the attending physician’s discretion, and data were collected as categorical data, not as actual LVEF values, to categorize patients into the low- and not-low-LVEF groups (those with an LVEF of 40–50% [HFmrEF] were allocated to the not-low-LVEF group). This might have affected the results. Fifth, this study was a subanalysis of a previously reported registry study, and data for the etiology of low LVEF and time-dependent changes in LVEF were unavailable. Finally, it was difficult to collect treatment strategy information for patients with LEAD, which may have differed among the participating facilities.
Conclusions
The presence of low LVEF (LVEF <40%) significantly increased the risk of MACCEs and MALEs in patients with LEAD who underwent EVT, regardless of the presence of symptomatic heart failure. More intensive and integrated management with GDMT for concomitant cardiac dysfunction, together with multifactorial approaches to comorbidities, may improve the cardiac and limb prognoses of patients with LEAD. Further studies are warranted to evaluate the association between cardiac output and functional prognosis in patients with LEAD.
Acknowledgment
This work was supported by the Vascular Disease Research Project of the Japan Research Promotion Society for Cardiovascular Disease, Tokyo, Japan.
Disclosures
The authors declare they have no conflicts of interest.
IRB Information
This study was approved by the institutional review board of Sakakibara Heart Institute, the core center of this multicenter study (reference no. 14-023), and the committees of each participating facility.
Data Availability
The deidentified participants’ data will not be shared as data sharing was not included in the IRB approval.
Supplementary Files
Please find supplementary file(s);
https://doi.org/10.1253/circj.CJ-23-0215
References
- 1.
Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, et al. The global health and economic burden of hospitalization for heart failure: Lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133.
- 2.
Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, et al. Framingham Heart Study: Lifetime risk for developing congestive heart failure: The Framingham Heart Study. Circulation 2002; 106: 3068–3072.
- 3.
Miura M, Sakata Y, Nochioka K, Takada T, Tadaki S, Ushigome R, et al. Prevalence, predictors and prognosis of patients with heart failure requiring nursing care. Circ J 2014; 78: 2276–2283.
- 4.
Shimokawa H, Miura M, Nochioka K, Sakata Y. Heart failure as a general pandemic in Asia. Eur J Heart Fail 2015; 17: 884–892.
- 5.
Clark AL, Poole-Wilson PA, Coats AJ. Exercise limitation in chronic heart failure: Central role of the periphery. J Am Coll Cardiol 1996; 28: 1092–1102.
- 6.
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022; 79: e263–e421.
- 7.
Tsutsui H, Ide T, Ito H, Kihara Y, Kinugawa K, Kinugawa S, et al. JCS/JHFS 2021 guideline focused update on diagnosis and treatment of acute and chronic heart failure. Circ J 2021; 85: 2252–2291.
- 8.
Fowkers FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013; 382: 1329–1340.
- 9.
Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res 2015; 116: 1509–1526.
- 10.
Steg PG, Bhatt DL, Wilson PW, D’Agostino R Sr, Ohman EM, Röther J, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007; 297: 1197–1206.
- 11.
Gerhard-Herman MD, Gornik HL, Barret C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017; 135: e686–e725.
- 12.
Aboyans V, Ricco JB, Bartelink MEL, Björck M, Brodmann M, Cohnert T, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society of Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries endorsed by the European Stroke Organization (ESO) The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J 2018; 39: 763–816.
- 13.
Fowkes FGR, Aboyans V, Fowkes FJ, McDermott MM, Sampson UKA, Criqui MH. Peripheral artery disease: Epidemiology and global perspectives. Nat Rev Cardiol 2017; 14: 156–170.
- 14.
Bhatt DL, Steg OG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 2006; 295: 180–189.
- 15.
Tromp J, Paniagua SMA, Lau ES, Allen NB, Blaha MJ, Gansevoort RT, et al. Age dependent risk factors of heart failure: Pooled population based cohort study. BMJ 2021; 372: N461.
- 16.
Anand RG, Ventura HO, Mehra MR. Is heart failure more prevalent in patients with peripheral arterial disease?: A meta-analysis. Congest Heart Fail 2007; 13: 319–322.
- 17.
Hebert K, Lopez B, Michael C, Franco E, Dias A, Trahan P, et al. The prevalence of peripheral artery disease in patients with heart failure by race and ethnicity. Congest Heart Fail 2010; 16: 118–121.
- 18.
Gupta DK, Skali H, Claggett B, Kasabov R, Cheng S, Shah AM, et al. Heart failure risk across the spectrum of ankle-brachial index: The ARIC study (Atherosclerosis Risk in Communities). JACC Heart Fail 2014; 2: 447–454.
- 19.
Chunawala Z, Chang PP, DeFilippis AP, Hall ME, Matsushita K, Caughey MC. Recurrent admission for acute decompensated heart failure among patients with and without peripheral artery disease: The ARIC study. J Am Heart Assoc 2020; 9: e017174.
- 20.
Samsky MD, Hellkamp A, Hiatt WR, Fowkes FGR, Baumgartner I, Berger JS, et al. Association of heart failure with outcomes among patients with peripheral artery disease: Insights from EUCLID. J Am Heart Assoc 2021; 10: e018684.
- 21.
Meltzer AJ, Shrikhande G, Gallagher KA, Aiello FA, Kahn S, Connolly P, et al. Heart failure is associated with reduced patency after endovascular intervention for symptomatic peripheral arterial disease. J Vasc Surg 2012; 55: 353–362.
- 22.
Tsutsui H, Isobe M, Ito H, Ito H, Okumura K, Ono M, et al. JCS 2017/JHFS 2017 guideline on diagnosis and treatment of acute and chronic heart failure: Digest version. Circ J 2019; 83: 2084–2184.
- 23.
Writing Committee Members; Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128: e240–e327.
- 24.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18: 891–975.
- 25.
Higashitani M, Uemura Y, Mizuno A, Utsunomiya M, Yamaguchi T, Matsui A, et al. Cardiovascular outcome and mortality in patients undergoing endovascular treatment for symptomatic peripheral artery disease: Short-term results of the Toma-Code registry. Circ J 2018; 82: 1917–1925.
- 26.
European Stroke Organization; Tendera M, Aboyans V, Bartelink ML, Baumgartner I, Clement D, Collet JP, et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: The Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J 2011; 32: 2851–2906.
- 27.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48: 452–458.
- 28.
Bonaca MP, Bhatt DL, Storey RF, Steg PG, Cohen M, Kuder J, et al. Ticagrelor for prevention of ischemic events after myocardial infarction in patients with peripheral artery disease. J Am Coll Cardiol 2016; 67: 2719–2728.
- 29.
Eikelboom JW, Connolly SJ, Bosch J, Dagenais GR, Hart RG, Shestakovska O, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017; 377: 1319–1330.
- 30.
Jones WS, Clare R, Ellis SJ, Mills JS, Fischman DL, Kraus WE, et al. Effect of peripheral arterial disease on functional and clinical outcomes in patients with heart failure (from HF-ACTION). Am J Cardiol 2011; 108: 380–384.
- 31.
Ahmed MI, Aronow WS, Croqui MH, Aban I, Love TE, Eichhorn EJ, et al. Effects of peripheral arterial disease on outcomes in advanced chronic systolic heart failure: A propensity-matched study. Circ Heart Fail 2010; 3: 118–124.
- 32.
Conrad MF, Cambria RP, Stone DH, Brewster DC, Kwolek CJ, Watkins MT, et al. Intermediate results of percutaneous endovascular therapy of femoropopliteal occlusive disease: A contemporary series. J Vasc Surg 2006; 44: 762–769.
- 33.
Bakken AM, Protack CD, Saad WE, Hart JP, Rhodes JM, Waldman DL, et al. Impact of chronic kidney disease on outcomes of superficial femoral artery endoluminal interventions. Ann Vasc Surg 2009; 23: 560–568.
- 34.
Simpson J, Jhund PS, Lund LH, Padmanabhan S, Claggett BL, Shen L, et al. Prognostic models derived in PARADIGM-HF and validated in ATMOSPHERE and the Swedish Heart Failure registry to predict mortality and morbidity in chronic heart failure. JAMA Cardiol 2011; 5: 432–441.
- 35.
Verbrruge FH, Guazzi M, Testani JM, Borlaug BA. Altered hemodynamics and end-organ damage in heart failure: Impact on the lung and kidney. Circulation 2020; 142: 998–1012.
- 36.
Ingis SC, Hermis A, Shehab S, Newton PJ, Lal S, Davidson PM. Peripheral arterial disease and chronic heart failure: A dangerous mix. Heart Fail Rev 2013; 18: 457–464.
- 37.
McDermott MM, Mehta S, Ahn H, Newton PJ, Lal S, Davidson PM. Atherosclerotic risk factors are less intensively treated in patients with peripheral artery disease than in patients with coronary artery disease. J Gen Intern Med 1997; 12: 209–215.
- 38.
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021; 42: 3599–3726.
- 39.
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371: 993–1004.
- 40.
McMuray JJ, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019; 381: 1995–2008.
- 41.
Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlavek J, et al. Effect of dapagliflozin on worsening heart failure and cardiovascular death in patients with heart failure with and without diabetes. JAMA 2020; 323: 1353–1368.
- 42.
Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med 2020; 383: 1413–1424.
- 43.
Zannad F, Ferreira JP, Pocock SJ, Anker SD, Butler J, Filippatos G, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020; 396: 819–829.
- 44.
Greene SJ, Butler J, Albert NM, DeVore AD, Sharma PP, Duffy CI, et al. Medical therapy for heart failure with reduced ejection fraction: The CHAMP-HF Registry. J Am Coll Cardiol 2018; 72: 351–366.
- 45.
Ødegaard KM, Lirhus SS, Melberg HO, Hallén J, Halvorsen S. Adherence and persistence to pharmacotherapy in patients with heart failure: A nationwide cohort study, 2014–2020. ESC Heart Fail 2023; 10: 405–415.
- 46.
Greene SJ, Fonarow GC, DeVore AD, Sharma PP, Vaduganathan M, Albert NM, et al. Titration of medical therapy for heart failure with reduced ejection fraction. J Am Coll Cardiol 2019; 73: 2365–2383.
- 47.
Savarese G, Bodegard J, Norhammar A, Sartipy P, Thuresson M, Cowie MR, et al. Heart failure drug titration, discontinuation, mortality and heart failure hospitalization risk: A multinational observational study (US, UK and Sweden). Eur J Heart Fail 2021; 23: 1499–1511.
- 48.
Rosano GMC, Moura B, Metra M, Böhm M, Bauersachs J, Ben Gal T, et al. Patient profiling in heart failure for tailoring medical therapy: A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2021; 6: 872–881.