Abstract
Background: Takayasu arteritis, affecting primarily young women, damages large arteries and organs. We examined the impact of disease duration and sex on organ damage and quality of life using Japan’s Intractable Disease Registry.
Methods and Results: After refining data, 2,013 of 2,795 patients were included in the study. Longer disease duration was related to a lower prevalence of disease activity symptoms, a higher prevalence of organ damage, and a higher proportion of patients requiring nursing care. Compared with men, women tended to have an earlier onset age, exhibiting longer disease duration. A higher proportion of women had aortic regurgitation and required nursing care. The proportion of female patients in employment was lower than that of the general female population, whereas no difference was observed between male patients and the general male population. Logistic regression analysis revealed that age at surveillance, brain ischemia, visual impairment/loss, and ischemic heart disease were significant factors associated with high nursing care needs (Level ≥2, with daily activity limitations).
Conclusions: Early diagnosis and effective treatment, particularly to prevent brain ischemia, visual impairment, and ischemic heart disease, may improve the quality of life of patients with Takayasu arteritis, especially women.
Takayasu arteritis (TAK), a rare inflammatory disease, predominantly affects younger women.1,2 Abnormally activated immune cells disfigure the aorta and its main branches,3,4 resulting in aortic regurgitation (AR), aneurysms, or organ ischemia in the brain,5 eyes,6 heart,7,8 and kidneys.9 This organ damage leads to limitations in physical activity and worsens quality of life (QOL).10 Although several studies have reported associations between disease duration and organ damage in patients with TAK,6,8,9,11,12 no study has analyzed organ damage stratified by disease duration.
Editorial p 295
Most TAK patients are women. Men with TAK have been reported to exhibit more severe disease types, such as aortic and multiple vascular lesions,2,13,14 but this has not been verified. QOL is reduced in TAK patients compared with healthy people,15–19 but no study has investigated sex differences in QOL in TAK, probably due to the small number of male patients.
Investigating factors associated with poor QOL and prognosis is crucial for planning treatments and social support for TAK patients. The Ministry of Health, Labour and Welfare (MHLW), Japan, maintains a national Specified Intractable Disease Registry to help patients by subsidizing medical expenses. Under this system, attending physicians complete case report forms (CRFs) for new patients and annually thereafter. We previously reported the clinical phenotypes of 1,372 patients newly registered over 10 years.2 The present study analyzed data of 2,795 patients newly and continuously registered in the 2013 fiscal year. We investigated symptoms, treatments, organ damage, and QOL based on disease duration and sex. In addition, we examined factors associated with high nursing care needs.
Methods
Database
This study included 2,795 TAK patients, including 211 newly registered in the 2013 fiscal year and 2,584 previously registered continuing into the 2013fiscal year. All patients met the 2008 Japanese diagnostic criteria for TAK.20 CRFs were collected from 30 of 47 prefectures in Japan.
Data on the Japanese general population and employment rates stratified by age and sex in the 2013 fiscal year was downloaded from Japanese government websites.21,22
Ethics Approval and Consent to Participate
The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine (R1990). All adult patients and guardians of child patients provided written informed consent to being a part of the Registry.
Symptoms, Organ Damage, and Level of Nursing Care Required
Information in a CRF includes a basic profile, Hata’s classification23 (only available in newly registered patients), level of nursing care required, social situation, symptoms, organs damaged, physical findings, laboratory findings, imaging findings, medication, and surgical treatments (Supplementary Table 1). Levels of nursing care were categorized as follows: Level 1, patients with no limitations in activities of daily living (ADL); Level 2, patients with limitations in ADL but not receiving care; Level 3, patients receiving partial assistance; and Level 4, patients requiring full assistance. Organ damage was defined as intractable complications due to TAK, including brain ischemia, visual impairment, blindness, AR (assessed by echocardiography), aortic aneurysm, aortic dissection, ischemic heart disease (IHD), renal artery stenosis, and renal dysfunction. The severity of AR was not analyzed owing to a substantial amount of missing data. The medication description refers to drugs the patient was receiving at the time of surveillance. As for surgical treatments, the description includes the patient’s past history.
Data Refining and Subgrouping
Data cleaning was performed (Supplementary Figure 1) to exclude patients with missing or inconsistent data and newly registered patients with long disease duration considered re-enrolled after discontinuation of annual registration (Supplementary Figure 2A). Patients with an age of onset >60 years were excluded (Supplementary Figure 2B,C) because we aimed to assess organ damage and QOL in typical TAK patients who developed the disease while young or middle aged. Finally, 2,013 patients (76 newly registered, 1,937 continuously registered) were included in this study.
The continuously registered patients were stratified into 3 groups according to disease duration: ≤5 years (“early” patients); >5 and ≤20 years (“late” patients); and >20 years (“very late” patients). In some analyses, continuously registered patients were stratified into subgroups by disease duration divided into 5-year intervals.
Statistical Analysis
Categorical variables expressed in 2×2 matrices were analyzed by Chi-squared tests, whereas continuous variables, presented as the mean±SD, were compared between 2 groups using two-tailed Student’s t-tests. These statistical analyses were performed using Microsoft Excel 2021, with P<0.05 considered statistically significant.
Logistic regression analysis was performed to identify factors associated with high nursing care levels. Explanatory variables included sex, age at surveillance, disease duration, and organ damage. The analysis focused on continuously registered patients without missing data (n=1,609). Statistical analysis was performed using R software (R Foundation for Statistical Computing, Vienna, Austria).
Employment rates were compared between TAK patients and the general population of Japan using a Chi-squared test.
Results
Patient Profiles
Figure 1 shows the profiles of the 2,013 patients included in this study. The female to male ratio was 9 : 1. The mean age of onset in the total population was 31.4±13.3 years (range 0–60, minimum−maximum), but tended to be younger in females than in males (31.2±13.1 vs. 33.1±14.9 years; P=0.062). In females, the age of onset was predominantly in the 20s, whereas the age of onset in males was evenly distributed (Figure 1C,D). The mean disease duration in the total population was 20.3±13.3 years (range 0–70 years), but was significantly longer in females than males (21.0±13.4 vs. 14.1±10.7 years; P<0.001; Supplementary Figure 3). The mean age at surveillance in the total population was 51.7±16.9 years (range 6–94 years), with females being significantly older than males (52.2±16.9 vs. 47.2±16.3 years; P<0.001; Supplementary Figure 4). Analysis of Hata’s classification showed that Types I (16%), IIa (21%), IIb (21%), and V (27%) were frequent (Supplementary Figure 5), consistent with previous findings.2

Symptoms, Laboratory Data, and Organ Damage
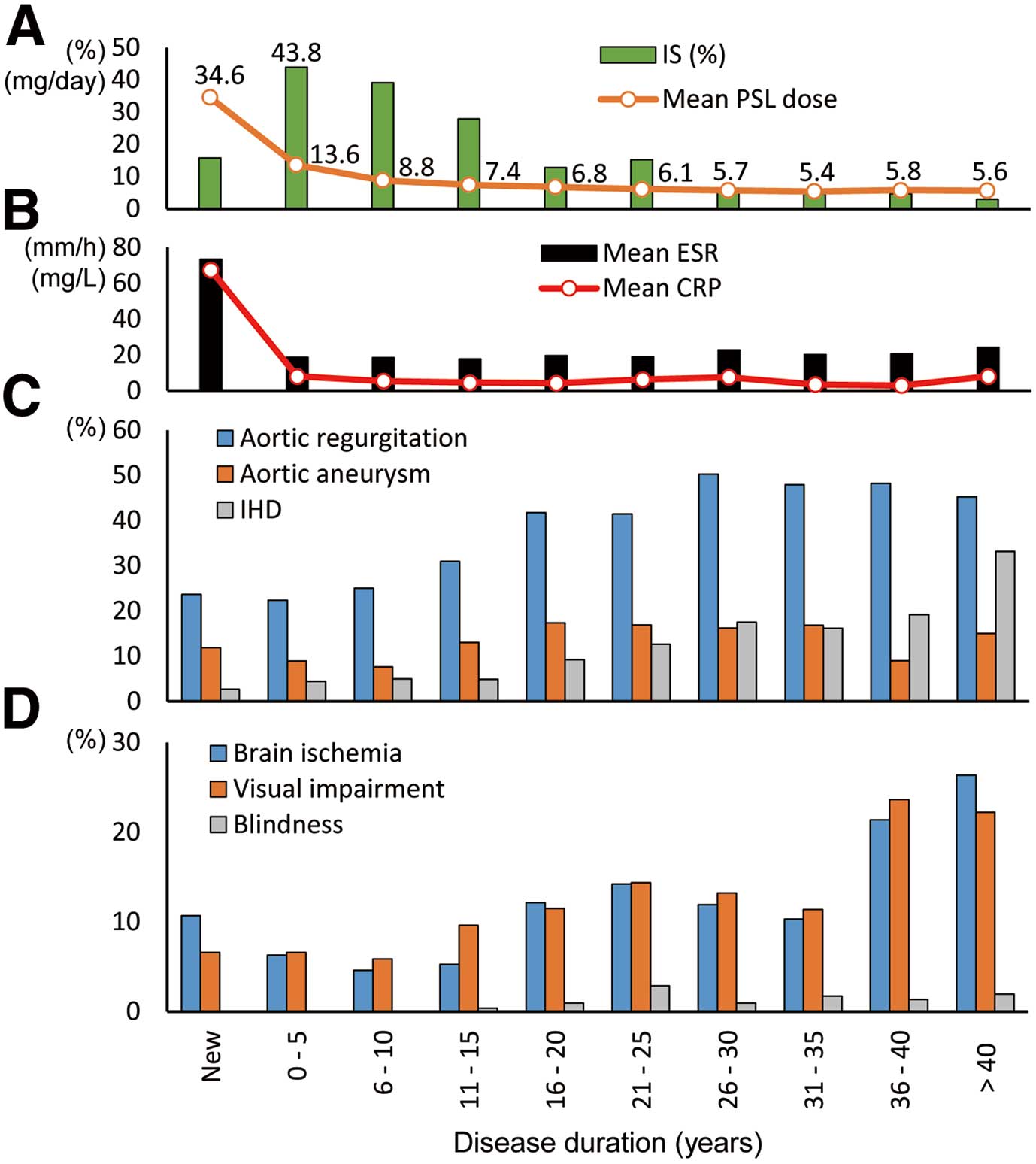
Patients were stratified into groups based on disease duration: new (n=76), early (n=273), late (n=766), and very late (n=898) patients (Figure 1E). Analysis of the prevalence of symptoms, organ damage, and levels of inflammatory markers stratified by disease duration revealed that longer disease duration was associated with a lower prevalence of fever and lower C-reactive protein (CRP) concentrations and erythrocyte sedimentation rates (ESR) (Table 1; Figure 2B). Longer disease duration was also associated with a higher prevalence of AR, brain ischemia, visual impairment, blindness, aortic aneurysm, IHD, and renal dysfunction (Table 1; Figure 2C,D).24 The prevalence of detailed symptoms and organ damage stratified by disease duration is detailed in Supplementary Table 2.
Table 1.
Symptoms, Treatments, and Organ Damage Stratified by Disease Duration
| |
Disease duration |
New
(n=76) |
Early
(n=273) |
Late
(n=766) |
Very late
(n=898) |
| Profiles and symptoms |
| No. females:males |
64:12 (5.3:1) |
232:41 (5.7:1) |
662:104 (6.4:1) |
853:45 (19.0:1) |
| Age at surveillance (years) |
34.0±15.4 |
34.9±15.4 |
45.9±14.9 |
61.8±11.9 |
| Fever |
51/76 (67.1) |
82/273 (30.0) |
83/766 (10.8) |
37/898 (4.1) |
| Arm claudication |
24/76 (31.6) |
88/273 (32.2) |
223/766 (29.1) |
248/898 (27.6) |
| Chest compression |
8/76 (10.5) |
26/273 (9.5) |
78/766 (10.2) |
153/898 (17.0) |
| CRP (mg/L) |
67.4±61.1 |
7.9±21.6 |
4.8±11.0 |
5.8±29.8 |
| ESR (mm/h) |
73.3±37.4 |
18.6±17.1 |
18.5±17.5 |
21.1±18.4 |
| Treatments |
| Glucocorticoids |
65/73 (89.0) |
244/267 (91.4) |
574/743 (77.3) |
434/855 (50.8) |
| PSL dose (mg/day) |
34.6±12.3 |
13.6±12.4 |
7.8±6.2 |
5.7±3.5 |
| Immunosuppressants |
11/70 (15.7) |
114/260 (43.8) |
201/713 (28.2) |
58/801 (7.2) |
| Antiplatelet agents |
33/72 (45.8) |
146/257 (56.8) |
453/724 (62.6) |
521/819 (63.6) |
| Anticoagulants |
11/70 (15.7) |
40/260 (15.4) |
155/716 (21.6) |
168/805 (20.9) |
| Endovascular treatments |
2/35 (5.7) |
13/150 (8.7) |
30/454 (6.6) |
34/501 (6.8) |
| Open cardiovascular surgery |
5/66 (7.6) |
18/256 (7.0) |
103/709 (14.5) |
118/837 (14.1) |
| Organ damage |
| Brain ischemia |
8/75 (10.7) |
17/271 (6.3) |
52/758 (6.9) |
142/882 (16.1) |
| Visual impairment |
5/76 (6.6) |
18/273 (6.6) |
66/766 (8.6) |
147/898 (16.4) |
| Blindness |
0/76 (0.0) |
0/273 (0.0) |
3/766 (0.4) |
16/898 (1.8) |
| Aortic regurgitation |
17/72 (23.6) |
59/264 (22.3) |
226/716 (31.6) |
392/843 (46.5) |
| Aortic aneurysm |
9/76 (11.8) |
24/271 (8.9) |
91/758 (12.0) |
132/877 (15.1) |
| Aortic dissection |
1/67 (1.5) |
5/232 (2.2) |
1/641 (0.2) |
16/757 (2.1) |
| Ischemic heart disease |
2/75 (2.7) |
12/271 (4.4) |
46/762 (6.0) |
168/886 (19.0) |
| Renal artery stenosis |
10/62 (16.1) |
23/221 (10.4) |
74/618 (12.0) |
101/692 (14.6) |
| Renal dysfunction |
4/76 (5.3) |
12/272 (4.4) |
68/761 (8.9) |
151/882 (17.1) |
| Nursing care level |
| Level 1 (no limitations in ADL) |
46/74 (62.2) |
161/265 (60.8) |
455/755 (60.3) |
367/872 (42.1) |
| Level 2 (ADL limitations but no assistance) |
23/74 (31.1) |
96/265 (36.2) |
277/755 (36.7) |
410/872 (47.0) |
| Level 3 (partial assistance) |
3/74 (4.1) |
5/265 (1.9) |
18/755 (2.4) |
80/872 (9.2) |
| Level 4 (fully assisted) |
2/74 (2.7) |
3/265 (1.1) |
5/755 (0.7) |
15/872 (1.7) |
Unless indicated otherwise, data are given as the mean±SD or n/N (%). Patients were stratified according to disease duration into four groups: new, early (≤5 years), late (5< and ≤20 years), and very late (>20 years). Denominators of some items are smaller than the number of patients due to missing data in the case report forms. ADL, activities of daily living; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; PSL, prednisolone.
Analysis of sex differences in clinical features (Table 2) revealed CRP concentrations (P<0.001) and the prevalence of fever (14.7% vs. 10.0%; P=0.041) were significantly higher in males than females. The prevalence of renal artery stenosis was higher in males, although the comparison was not reliable due to missing data for renal artery stenosis in the CRFs. In contrast, ESR (P=0.004) and the prevalence of AR (37.9% vs. 29.8%; P=0.032) were significantly higher in female than male patients.
Table 2.
Symptoms, Treatments, and Organ Damage in Patients With Takayasu Arteritis Stratified by Sex
| |
Female
(n=1,747) |
Male
(n=190) |
P value |
| Profiles and symptoms |
| Age of onset (years) |
31.2±13.1 |
33.1±14.9 |
0.062 |
| Disease duration (years) |
21.0±13.4 |
14.1±10.7 |
<0.001A |
| Age at surveillance (years) |
52.2±16.9 |
47.2±16.3 |
<0.001A |
| Fever |
174/1,747 (10.0) |
28/190 (14.7) |
0.041B |
| Arm claudication |
513/1,747 (29.4) |
46/190 (24.2) |
0.136 |
| Chest compression |
230/1,747 (13.2) |
27/190 (14.2) |
0.687 |
| CRP (mg/L) |
5.0±19.8 |
11.8±41.0 |
<0.001A |
| ESR (mm/h) |
20.1±18.0 |
14.9±15.8 |
0.004A |
| Treatments |
| Glucocorticoids |
1,112/1,676 (66.3) |
140/189 (74.1) |
0.032B |
| PSL dose (mg/day) |
8.0±7.5 |
9.9±9.1 |
0.010A |
| Immunosuppressants |
312/1,599 (19.5) |
61/175 (34.9) |
<0.001B |
| Antiplatelet agents |
999/1,624 (61.5) |
121/176 (68.8) |
0.060 |
| Anticoagulants |
312/1,604 (19.5) |
51/177 (28.8) |
0.003B |
| Endovascular treatments |
64/998 (6.4) |
13/107 (12.1) |
0.027B |
| Open cardiovascular surgery |
208/1,626 (12.8) |
31/176 (17.6) |
0.073 |
| Organ damage |
| Brain ischemia |
196/1,722 (11.4) |
15/189 (7.9) |
0.151 |
| Visual impairment |
206/1,747 (11.8) |
25/190 (13.2) |
0.581 |
| Blindness |
18/1,747 (1.0) |
1/190 (0.5) |
0.503 |
| Aortic regurgitation |
623/1,642 (37.9) |
54/181 (29.8) |
0.032B |
| Aortic aneurysm |
219/1,717 (12.8) |
28/189 (14.8) |
0.424 |
| Aortic dissection |
21/1,471 (1.4) |
1/159 (0.6) |
0.407 |
| Ischemic heart disease |
201/1,729 (11.6) |
25/190 (13.2) |
0.534 |
| Renal artery stenosis |
169/1,377 (12.3) |
29/154 (18.8) |
0.021B |
| Renal dysfunction |
216/1,725 (12.5) |
15/190 (7.9) |
0.063 |
| Nursing care level |
| Level 1 (no limitations in ADL) |
873/1,707 (51.1) |
110/185 (59.5) |
0.032B |
| Level 2 (ADL limitations but no assistance) |
710/1,707 (41.6) |
73/185 (39.5) |
0.576 |
| Level 3 (partial assistance) |
101/1,707 (5.9) |
2/185 (1.1) |
0.006B |
| Level 4 (fully assisted) |
23/1,707 (1.3) |
0/185 (0.0) |
0.112 |
Unless indicated otherwise, data are given as the mean±SD or n/N (%). AP<0.05, Student’s t-test. BP<0.05, Chi-squared test. Continuously registered patients were analyzed. Denominators of several items are smaller than the number of patients due to missing data in case report forms. ADL, activities of daily living; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; PSL, prednisolone.
Disease duration was significantly longer in females than males (Table 2). Notably, the female to male ratio was approximately 6 : 1 in the new, early, and late patient groups, but 19 : 1 in the very late group (Table 1). Although we intended to compare organ damage and QOL by sex, inclusion of the very late group, comprising patients with disease duration >20 years, raised concerns that organ damage and limited QOL would be overestimated in females due to the effects of aging. Therefore, sex differences were analyzed in patients with disease duration ≤20 years (i.e., the new, early, and late groups; Supplementary Table 3). Comparisons in these groups found no significant sex differences in disease duration, age at surveillance, prevalence of fever, or organ damage. However, the prevalence of arm claudication was significantly higher in females than males (31.2% vs. 22.1%; P=0.026). Even under these conditions, CRP concentrations were higher in males (P<0.001), whereas ESR was higher in females (P=0.018).
Treatments
Patient treatments stratified by disease duration are presented in Table 1 and Figure 2A. Longer disease duration was associated with a lower proportion of patients treated with glucocorticoids (GC) and lower mean dose of prednisolone (PSL). Approximately 90% of new patients were administered GC and received a mean dose of 34.6 mg/day PSL. The mean PSL dose in very late patients was 5.7 mg/day, with approximately half of very late patients being GC-free. Longer disease duration was associated with a lower proportion of patients treated with immunosuppressants, a higher proportion treated with antiplatelet and anticoagulant agents, and a higher proportion with a history of open cardiovascular surgery. Paradoxically, the proportion of patients with a history of endovascular treatments (EVT) was higher in the early than the late and very late groups, although reliable comparison was not feasible due to missing data for EVT in the CRFs.
Analysis of sex differences in treatments (Table 2) revealed that a significantly higher proportion of males than females received GC, immunosuppressants, and anticoagulants, and that the doses of GC were higher in males. When limited to patients with disease duration ≤20 years, the proportion of males receiving immunosuppressants and anticoagulants remained significantly higher than that of females (Supplementary Table 3).
Of the 2,013 patients in this study, data on whether they had undergone EVT was available for 1,140. Of these 1,140 patients, 79 had undergone EVT. There was no available information about the vessel sites. Similarly, details were available for 1,868 patients regarding open cardiovascular surgery. Of these 1,868 patients, 244 had undergone the surgery and descriptions of the procedures were available for 178. In all, 181 surgeries were described, because 3 patients had 2 surgeries each (Table 3). The surgeries were categorized as cardiac (38.7%), aortic (34.3%), peripheral artery (24.3%), and other (2.8%).
Table 3.
Open Cardiovascular Surgery Procedures in Patients With Takayasu Arteritis
| Open cardiovascular surgery procedures |
n (%) |
| 1. Cardiac surgery |
70 (38.7) |
| 1-1. AVR |
44 (24.3) |
| 1-2. CABG |
14 (7.7) |
| 1-3. AVR+CABG |
5 (2.8) |
| 1-4. Multiple valve surgery |
4 (2.2) |
| 1-5. Surgical coronary angioplasty |
2 (1.1) |
| 1-6. Pericardiotomy |
1 (0.6) |
| 2. Aortic surgery |
62 (34.3) |
| 2-1. Aortic aneurysm surgery (aortic root)A |
32 (17.7) |
| 2-1-1. Aortic root replacement |
23 (12.7) |
| 2-1-2. Aortic root replacement+CABG |
2 (1.1) |
| 2-1-3. Aortic root+hemiarch replacement |
3 (1.7) |
| 2-1-4. Aortic root+arch replacement |
4 (2.2) |
| 2-2. Aortic aneurysm surgery (other) |
21 (11.6) |
| 2-2-1. Ascending |
3 (1.7) |
| 2-2-2. Ascending+arch |
9 (5.0) |
| 2-2-3. Arch+thoracic descending |
1 (0.6) |
| 2-2-4. Thoracic descending |
4 (2.2) |
| 2-2-5. Thoracic descending+abdominal |
2 (1.1) |
| 2-2-6. Abdominal |
1 (0.6) |
| 2-2-7. Position not described |
1 (0.6) |
| 2-3. Aorto-aortic bypass surgery |
9 (5.0) |
| 3. Peripheral artery surgery |
44 (24.3) |
| 3-1. Bypass surgery |
39 (21.5) |
| 3-1-1. Aorto-subclavian |
7 (3.9) |
| 3-1-2. Subclavian-carotid |
4 (2.2) |
| 3-1-3. Femoro-popliteal |
4 (2.2) |
| 3-1-4. Aorto-renal |
3 (1.7) |
| 3-1-5. Axillo-femoral |
3 (1.7) |
| 3-1-6. Aorto-carotid |
2 (1.1) |
| 3-1-7. Carotid-axillary |
2 (1.1) |
| 3-1-8. Carotid-subclavian |
2 (1.1) |
| 3-1-9. Aorto-axillary |
1 (0.6) |
| 3-1-10. Aorto-femoral |
1 (0.6) |
| 3-1-11. Aorto-iliac |
1 (0.6) |
| 3-1-12. Carotid-carotid |
1 (0.6) |
| 3-1-13. Ilio-axillaryB |
1 (0.6) |
| 3-1-14. Ilio-femoral |
1 (0.6) |
| 3-1-15. Subclavian-subclavian |
1 (0.6) |
| 3-1-16. Position not described |
3 (1.7) |
| 3-1-17. Multiple bypass surgery |
2 (1.1) |
| 3-2. Peripheral artery aneurysm surgery |
5 (2.8) |
| 3-2-1. Carotid replacement |
3 (1.7) |
| 3-2-2. Femoral replacement |
1 (0.6) |
| 3-2-3. Carotid artery aneurysm resection |
1 (0.6) |
| 4. Other |
5 (2.8) |
| 4-1. Renal autotransplantation |
3 (1.7) |
| 4-2. Cerebral aneurysm clipping |
2 (1.1) |
| Total |
181 (100.0) |
In all, 181 open cardiovascular surgeries were performed in 178 patients: 3 patients each underwent 2 surgeries. Endovascular treatments are not included in the table. The listed numbers are used to categorize the various types of surgeries for TAK. AAortic root replacement included valve replacement and valve-sparing operation. BIlio-axillary bypass was written as it was in the case report form. AVR, aortic valve replacement; CABG, coronary artery bypass grafting.
Level of Nursing Care
Associations between nursing care level and disease duration are presented in Table 1. Longer disease duration was associated with a smaller proportion of patients categorized as being without limitations in ADL (Level 1) and a larger proportion of patients categorized as having limitation in ADL but not receiving care (Level 2) and receiving partial assistance (Level 3). Similar trends were observed when patients were stratified into small subgroups divided by 5-year increments of disease duration (Supplementary Figure 6A).
Analysis of sex differences in the proportion of patients receiving different levels of nursing care (Table 2) revealed the proportion receiving Level 3 care was significantly higher among females than males (5.9% vs 1.1%; P=0.006), whereas the proportion without limitations in ADL (Level 1) was significantly higher among males. When limited to disease duration ≤20 years, there were no significant sex differences in the proportion of patients receiving different levels of nursing care (Supplementary Table 3).
Logistic regression analysis identified factors associated with high nursing care levels (Level ≥2, with limitations in ADL) as age at surveillance, brain ischemia, visual impairment/loss, and IHD (Figure 3; Supplementary Table 4). Consistently, patients with brain ischemia, visual impairment/loss, and IHD tended to require higher nursing care levels than patients without these respective conditions (Supplementary Figure 7).
Hata’s Classification and Organ Damage
Although information of Hata’s classification was only available for newly registered patients and the number of patients was limited, newly registered patients were stratified according to Hata’s classification to analyze the prevalence of organ damage and levels of nursing care (Supplementary Figure 8). Of the 73 newly registered patients, 5 had high nursing care requirements (Level 3 or 4) and they were classified as Types IIa, IIb, III, or V in Hata’s classification (Supplementary Figure 8B). Investigation of these 5 patients revealed no visual impairment/loss, but 3 had cerebral ischemia and 2 had IHD.
Employment and School Attendance
Analysis of social situations in patients stratified by disease duration (Supplementary Figure 6B) revealed that approximately 20% of newly registered patients were admitted to hospital, whereas a higher proportion of those with longer disease duration were receiving home therapy. Comparisons of female and male patients stratified by age at surveillance (Figure 4) revealed that a higher proportion of male than female patients were workers and students, whereas the proportion identified as housekeepers was higher among female patients.
Considering potential cultural and social influences on sex differences in social situations in Japan, we compared the employment rates of female and male TAK patients to the respective employment rates in the Japanese population in the 2013 fiscal year (Figure 5). A highly significant difference in employment rates was observed among women (P=4.25×10−38), but not among men (P=0.217; Supplementary Table 5).
To determine whether organ damage found in the above multivariate analysis was also associated with limitations in ADL in female patients, we performed a multivariate analysis restricted to female patients (Supplementary Figure 9; Supplementary Table 6). The analysis similarly identified age at surveillance, brain ischemia, visual impairment/loss, and IHD as factors associated with high levels of nursing care.
Discussion
The present study surveyed the MHLW registry of TAK patients. The cohort included patients who varied in disease duration, from newly registered to those with disease duration >20 years. Longer disease duration was associated with a lower prevalence of symptoms related to disease activity, such as fever and general malaise, as well as lower CRP concentrations and ESR. In contrast, longer disease duration was associated with a higher prevalence of organ damage. Disease duration has been reported to be significantly longer in patients with than without coronary artery lesions,7 cardiac involvement,8 and retinopathy.6 Moreover, longer disease duration was found to be a significant risk factor for decreased renal function,9 aneurysms,11 and pulmonary artery involvement,12 and to be significantly correlated with the TAK damage score.25,26
Analysis of sex differences revealed that females tended to be younger at disease onset, with a significantly longer disease duration. Analysis of the TAK patient population showed that the prevalence of AR was significantly higher in females, whereas that of fever was significantly higher in males. Among the cohort with disease duration ≤20 years, there were no significant sex differences in fever or AR, but the prevalence of arm claudication was significantly higher in female patients. The higher prevalence of AR and arm claudication in female patients is consistent with our previous findings2 and previous reports.27–29
The present study also found that CRP concentrations were higher in males and that the ESR was higher in females. Previous studies reported inflammatory markers were higher in female patients.29,30 For example, one study reported that a higher proportion of females had elevated ESR, but that study did not measure CRP.30 Another study found CRP concentrations were similar in both sexes, whereas ESR was significantly higher in female patients.29 The higher ESR observed in female patients in the present study may reflect the general phenomenon of ESR being higher in women than in men, and may not be specific to TAK.
Curiously, our study found that a significantly higher proportion of males than females were receiving immunosuppressive drugs . First, the higher CRP concentrations in male than female patients suggests that disease activity may be higher in males. Second, because female patients had a younger age at onset of TAK, they may have received less potent treatments to preserve their fertility.
In the present study, open cardiovascular surgery in TAK was characterized by procedures associated with AR, replacement for aortic aneurysm, and bypass grafting for vascular stenosis. Regarding EVT, there was no information about the vessel sites targeted. A study of 2,450 cases of EVT reported the target vessel sites included the subclavian or axillary artery (26%), renal artery (24%), the aorta (19%), and carotid artery (14%).31 In our cohort, EVT may have been performed not only on peripheral arteries and the aorta, but also on coronary arteries.
Compared with healthy individuals, scores on the Short Form-36 QOL index have been reported to be significantly worse for TAK patients,15,16,18,19 as have scores on the Health Assessment Questionnaire.17 Using logistic regression analysis, we found age at surveillance, brain ischemia, visual impairment/loss, and IHD were significant factors associated with high nursing care levels. Although ADL inevitably decline with age, there is the potential to improve ADL by preventing brain ischemia, visual impairment, and IHD through early treatment. In the present study, we could not analyze the relationship between Hata’s classification and long-term nursing care levels due to insufficient data. However, brain ischemia, visual impairment/loss, and IHD may contribute to high nursing care levels, not only in new patients, but also in those with a longer disease duration. Specifically, patients classified as Types IIa, IIb, and V on Hata’s classification (involving both the head/neck branches and the ascending aorta [coronary artery branches]) may require particularly careful treatments to preserve their QOL.
Paradoxically, analysis stratified by 5-year intervals of disease duration revealed a low prevalence of aortic aneurysm in patients with a disease duration of 36–40 years and a high prevalence in new patients (Figure 2C). The prevalence of brain ischemia and visual impairment showed a declining trend over a disease duration of 26–35 years, and the prevalence of brain ischemia was high in new patients (Figure 2D). We believe the absence of cumulative increases with disease duration was due to the cross-sectional nature of this study.
The employment rate of male patients was the same as that for the general male population in Japan. In contrast, the employment rate of female patients was lower than that of the general female population. First, disease activity may be associated with employment. For example, the Work Productivity and Activity Impairment score in TAK patients was reported to be significantly correlated with disease activity.32 However, in the present study, males seemed to have more active disease. Second, because females tended to be younger at disease onset, they may have missed opportunities for education and job training due the burden of illness and the side effects of GC. Third, brain ischemia, visual impairment/loss, and IHD were extracted as factors associated with high levels of nursing care also in female patients (Supplementary Figure 9). Early diagnosis and more effective treatments may control this organ damage, and hence improve the low employment rate. In addition, employment support may be required, especially for female patients.
Unfortunately, the CRFs do not include any details about treatment with biologics. At the time of surveillance, biologics were not covered by Japan health insurance. Several studies have reported that infliximab and tocilizumab improved Short Form-36 scores.33,34 These agents may prevent the accumulation of organ damage, improve QOL, and enhance the social participation of these patients.
The present study had some limitations. First, data from the MHLW registry for TAK were retrospective because they relied on CRFs written by attending physicians. Many CRFs had missing data, especially for aortic dissection, renal artery stenosis, and EVT. Accordingly, the prevalence rates of these items could not be reliably compared between the sexes or according to other variables, such as disease duration. Second, this was a cross-sectional study. Due to their past onset of TAK, patients with long disease duration may have received inadequate treatment compared with more recently diagnosed patients, leading to more severe damage. In addition, the prevalence of complications may not cumulatively increase with a longer disease duration. Third, because the registry is for medical expense subsidies that stop when the patient dies, the registry does not contain any information on the date or cause of death. Fourth, we could not analyze the association between AR severity and nursing care levels due to a substantial amount of missing data. Fifth, the CRFs we surveyed did not include information on blood pressure, HbA1c, antihypertensive medications, and antidiabetic drugs, which is important for the assessment of the prognosis of vascular lesions. Sixth, the CRFs we surveyed did not include information regarding postoperative pseudoaneurysms, restenosis, and retreatment intervention in patients who underwent surgery.
In conclusion, a national registry data of TAK patients was analyzed to examine factors associated with organ damage and QOL. Longer disease duration was found to be associated with a higher prevalence of organ damage and a higher proportion of patients needing nursing care. Female patients exhibited earlier onset age and longer disease duration. A higher proportion of female than male patients showed AR and required nursing care, and female patients had lower employment rates compared with the general population. Age at surveillance, brain ischemia, visual impairment/loss, and IHD were significant factors associated with high nursing care levels. Early diagnosis and treatment preventing this organ damage may improve QOL in TAK patients, especially females.
Acknowledgments
The authors thank Dr. Kazuhiro Yamazaki (Department of Cardiovascular Surgery, Kyoto University Hospital) for supervising the classification of surgical procedures. The authors express their gratitude to Professor Akiyoshi Nakakura (Kyoto University) for providing valuable advice on statistical analysis. The authors thank David Price of English Services for Scientists for English language proofreading.
Sources of Funding
This work was supported by a Grant-in-Aid for Intractable Vasculitis from the Ministry of Health, Labour and Welfare, Japan (Ippan-018, 20FC1044, and 23FC1019).
Disclosures
H.Y. has received advisory and lecture fees from Janssen Pharmaceuticals and lecture fees from Chugai Pharmaceutical Co., Ltd. Y.N. has received research grants from Bayer Yakuhin, Ltd; and consulting and/or lecture fees and/or research grants from Chugai, AbbVie, Astellas, Takeda, Daiichi Sankyo, Actelion, and Japan Blood Products Organization. H.A.U. belongs to the Department of Chronic Kidney Disease and Cardiovascular Disease, which is endowed by Olba Healthcare Holdings, Chugai, Boehringer Ingelheim, and Terumo Corporation. T.S. has received research grants and/or honoraria from AbbVie, AsahiKASEI, Astellas, Ayumi, Bristol-Myers Squibb K.K., Chugai, Daiichi Sankyo, Eli Lilly Japan K.K., Mitsubishi-Tanabe, Ono, Pfizer, Takeda, and UCB Japan Co. Ltd. M.I. has received honoraria from Chugai, Daiichi Sankyo, and Pfizer. M.H. has received fees for research and/or consultancy from AbbVie Japan GK, Asahi Kasei, Astellas, Ayumi, Bayer Yakuhin, Boehringer Ingelheim, Bristol-Myers Squibb K.K., Chugai, Daiichi Sankyo, Eli Lilly Japan K.K., Kaken, Kissei, Mitsubishi Tanabe, Mochida, Nippon Kayaku, Nippon Shinyaku, Taisho, Teijin, UCB Japan, and Viatris Japan. Y.W, and S.F. have no conflicts of interest to disclose.
IRB Information
This study was approved by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine (R1990).
Supplementary Files
Please find supplementary file(s);
https://doi.org/10.1253/circj.CJ-23-0656
References
- 1.
Isobe M, Amano K, Arimura Y, Ishizu A, Ito S, Kaname S, et al. JCS 2017 guideline on management of vasculitis syndrome: Digest version. Circ J 2020; 84: 299–359, doi:10.1253/circj.CJ-19-0773.
- 2.
Watanabe Y, Miyata T, Tanemoto K. Current clinical features of new patients with Takayasu arteritis observed from cross-country research in Japan: Age and sex specificity. Circulation 2015; 132: 1701–1709, doi:10.1161/circulationaha.114.012547.
- 3.
Yoshifuji H. Pathophysiology of large vessel vasculitis and utility of interleukin-6 inhibition therapy. Mod Rheumatol 2019; 29: 287–293, doi:10.1080/14397595.2018.1546358.
- 4.
Yoshifuji H, Terao C. Roles of cytotoxic lymphocytes and MIC/LILR families in pathophysiology of Takayasu arteritis. Inflamm Regen 2020; 40: 9, doi:10.1186/s41232-020-00119-6.
- 5.
Kong F, Huang X, Su L, Liao Q, Wang C, Zhao Y. Risk factors for cerebral infarction in Takayasu arteritis: A single-centre case-control study. Rheumatology (Oxford) 2021; 61: 281–290, doi:10.1093/rheumatology/keab308.
- 6.
Esen F, Ergelen R, Alibaz-Öner F, Çelik G, Direskeneli H, Kazokoğlu H. Ocular findings and blood flow in patients with Takayasu arteritis: A cross-sectional study. Br J Ophthalmol 2019; 103: 928–932, doi:10.1136/bjophthalmol-2018-312580.
- 7.
Soto ME, Meléndez-Ramírez G, Kimura-Hayama E, Meave-Gonzalez A, Achenbach S, Herrera MC, et al. Coronary CT angiography in Takayasu arteritis. JACC Cardiovasc Imaging 2011; 4: 958–966, doi:10.1016/j.jcmg.2011.04.019.
- 8.
Li J, Li H, Sun F, Chen Z, Yang Y, Zhao J, et al. Clinical characteristics of heart involvement in Chinese patients with Takayasu arteritis. J Rheumatol 2017; 44: 1867–1874, doi:10.3899/jrheum.161514.
- 9.
Chen Z, Li J, Yang Y, Li H, Zhao J, Sun F, et al. The renal artery is involved in Chinese Takayasu’s arteritis patients. Kidney Int 2018; 93: 245–251, doi:10.1016/j.kint.2017.06.027.
- 10.
Luna-Vargas L, Hinojosa CA, Contreras-Yanez I, Anaya-Ayala JE, Hinojosa-Azaola A. Takayasu’s arteritis from the patients’ perspectives: Measuring the pulse to the patient-reported outcomes. Ann Vasc Surg 2021; 73: 314–320, doi:10.1016/j.avsg.2020.10.026.
- 11.
Pan L, Du J, Chen D, Zhao Y, Guo X, Qi G, et al. Takayasu arteritis with dyslipidemia increases risk of aneurysm. Sci Rep 2019; 9: 14083, doi:10.1038/s41598-019-50527-z.
- 12.
Xi X, Du J, Liu J, Zhu G, Qi G, Pan L. Pulmonary artery involvement in Takayasu arteritis: A retrospective study in Chinese population. Clin Rheumatol 2021; 40: 635–644, doi:10.1007/s10067-020-05271-5.
- 13.
Mont’Alverne AR, Paula LE, Shinjo SK. Features of the onset of Takayasu’s arteritis according to gender. Arq Bras Cardiol 2013; 101: 359–363, doi:10.5935/abc.20130180.
- 14.
Wan J, Qi S, Liao H, Ci W, Guo Y, Wang T. Comparison of clinical features at the onset of Takayasu’s arteritis according to age and sex. Curr Vasc Pharmacol 2020; 18: 80–86, doi:10.2174/1570161117666190621152506.
- 15.
Akar S, Can G, Binicier O, Aksu K, Akinci B, Solmaz D, et al. Quality of life in patients with Takayasu’s arteritis is impaired and comparable with rheumatoid arthritis and ankylosing spondylitis patients. Clin Rheumatol 2008; 27: 859–865, doi:10.1007/s10067-007-0813-9.
- 16.
Abularrage CJ, Slidell MB, Sidawy AN, Kreishman P, Amdur RL, Arora S. Quality of life of patients with Takayasu’s arteritis. J Vasc Surg 2008; 47: 131–136, doi:10.1016/j.jvs.2007.09.044.
- 17.
Yilmaz N, Can M, Oner FA, Kalfa M, Emmungil H, Karadag O, et al. Impaired quality of life, disability and mental health in Takayasu’s arteritis. Rheumatology (Oxford) 2013; 52: 1898–1904, doi:10.1093/rheumatology/ket238.
- 18.
Omma A, Erer B, Karadag O, Yilmaz N, Alibaz-Oner F, Yildiz F, et al. Remarkable damage along with poor quality of life in Takayasu arteritis: Cross-sectional results of a long-term followed-up multicentre cohort. Clin Exp Rheumatol 2017; 35(Suppl 103): 77–82.
- 19.
Misra DP, Rathore U, Patro P, Agarwal V, Sharma A. Patient-reported outcome measures in Takayasu arteritis: A systematic review and meta-analysis. Rheumatol Ther 2021; 8: 1073–1093, doi:10.1007/s40744-021-00355-3.
- 20.
JCS Joint Working Group. Guideline for management of vasculitis syndrome (JCS 2008). Circ J 2011; 75: 474–503, doi:10.1253/circj.CJ-88-0007.
- 21.
Statistics of Japan. Population and percentage distribution by age (5-year age group) and sex – total population, October 1, each year. e-Stat. https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=datalist&toukei=00200524&tstat=000000090001&cycle=7&year=20130&month=0&tclass1=000001011679&tclass2val=0 (accessed January 1, 2022).
- 22.
Statistics Bureau, Ministry of Internal Affairs and Communications, Japan. Labor force survey (basic tabulation) summary of average (preliminary) results 2013 [in Japanese]. https://www.stat.go.jp/data/roudou/rireki/nen/ft/pdf/2013.pdf (accessed January 1, 2022).
- 23.
Hata A, Noda M, Moriwaki R, Numano F. Angiographic findings of Takayasu arteritis: New classification. Int J Cardiol 1996; 54(Suppl): S155–S163, doi:10.1016/s0167-5273(96)02813-6.
- 24.
Ogino H, Iida O, Akutsu K, Chiba Y, Hayashi H, Ishibashi-Ueda H, et al. JCS/JSCVS/JATS/JSVS 2020 guideline on diagnosis and treatment of aortic aneurysm and aortic dissection. Circ J 2023; 87: 1410–1621, doi:10.1253/circj.CJ-22-0794.
- 25.
Kaymaz-Tahra S, Alibaz-Oner F, Direskeneli H. Assessment of damage in Takayasu’s arteritis. Semin Arthritis Rheum 2020; 50: 586–591, doi:10.1016/j.semarthrit.2020.04.003.
- 26.
Danda D, Goel R, Joseph G, Kumar ST, Nair A, Ravindran R, et al. Clinical course of 602 patients with Takayasu’s arteritis: Comparison between childhood-onset versus adult onset disease. Rheumatology (Oxford) 2021; 60: 2246–2255, doi:10.1093/rheumatology/keaa569.
- 27.
Tomelleri A, Campochiaro C, Sartorelli S, Cavalli G, De Luca G, Baldissera E, et al. Gender differences in clinical presentation and vascular pattern in patients with Takayasu arteritis. Scand J Rheumatol 2019; 48: 482–490, doi:10.1080/03009742.2019.1581838.
- 28.
Zhang Z, Wang W, Zhou M, Lu PYJ, Li Y, Chen Y. An observational study of sex differences in Takayasu arteritis in China: Implications for worldwide regional differences. Ann Vasc Surg 2020; 66: 309–317, doi:10.1016/j.avsg.2019.12.007.
- 29.
Lim AY, Lee GY, Jang SY, Gwag HB, Choi SH, Jeon ES, et al. Gender differences in clinical and angiographic findings of patients with Takayasu arteritis. Clin Exp Rheumatol 2015; 33(Suppl 89): S-132–S-137.
- 30.
Sharma BK, Jain S. A possible role of sex in determining distribution of lesions in Takayasu Arteritis. Int J Cardiol 1998; 66(Suppl 1): S81–S84, doi:10.1016/s0167-5273(98)00154-5.
- 31.
Joseph G, Thomson VS, Attumalil TV, Mathen PG, Anandaraj AM, George OK, et al. Outcomes of percutaneous intervention in patients with Takayasu arteritis. J Am Coll Cardiol 2023; 81: 49–64, doi:10.1016/j.jacc.2022.10.024.
- 32.
Erdal S, Nalbantoğlu B, Gür MB, Yıldırım M, Kılıçarslan A, Kaymaz-Tahra S, et al. HADS-depression score is a mediator for illness perception and daily life impairment in Takayasu’s arteritis. Clin Rheumatol 2021; 40: 4109–4116, doi:10.1007/s10067-021-05719-2.
- 33.
Quartuccio L, Schiavon F, Zuliani F, Carraro V, Catarsi E, Tavoni AG, et al. Long-term efficacy and improvement of health-related quality of life in patients with Takayasu’s arteritis treated with infliximab. Clin Exp Rheumatol 2012; 30: 922–928.
- 34.
Nakaoka Y, Isobe M, Tanaka Y, Ishii T, Ooka S, Niiro H, et al. Long-term efficacy and safety of tocilizumab in refractory Takayasu arteritis: Final results of the randomized controlled phase 3 TAKT study. Rheumatology (Oxford) 2020; 59: 2427–2434, doi:10.1093/rheumatology/kez630.




