Images in Cardiovascular Medicine
Potential Benefits of Non-Gated Computed Tomography for an Early Invasive Strategy in Ventricular Fibrillation
2024 Volume 88 Issue 4 Pages 614-

Details
2024 Volume 88 Issue 4 Pages 614-
A man in his 70s attending another hospital for hypertrophic cardiomyopathy (HCM) was transferred because of out-of-hospital cardiac arrest (OHCA) with an estimated no-flow time of 1 min and low-flow time of 6 min. After electrical defibrillation for ventricular fibrillation (VF), he was hemodynamically stable and oriented with no chest pain. ECG showed no ST-segment elevation (Figure A), and echocardiography showed left ventricular wall thickening without asynergy. The troponin I level was not elevated 30 min after the OHCA. Non-gated computed tomography (CT) showed a perfusion defect at the subendocardial left ventricular anteroseptum (Figure B), suggesting a lesion of the left anterior descending artery (LAD) responsible for acute myocardial infarction. Without retesting for cardiac enzymes, we performed urgent coronary angiography (CAG), which revealed severe obstructive stenosis of the LAD (Figure C,D). Despite several episodes of VF during CAG, there was no recurrence after revascularization. Peak creatine kinase/creatine kinase-MB and troponin I levels were 1,703/186 IU/L and >50,00 ng/mL, respectively.
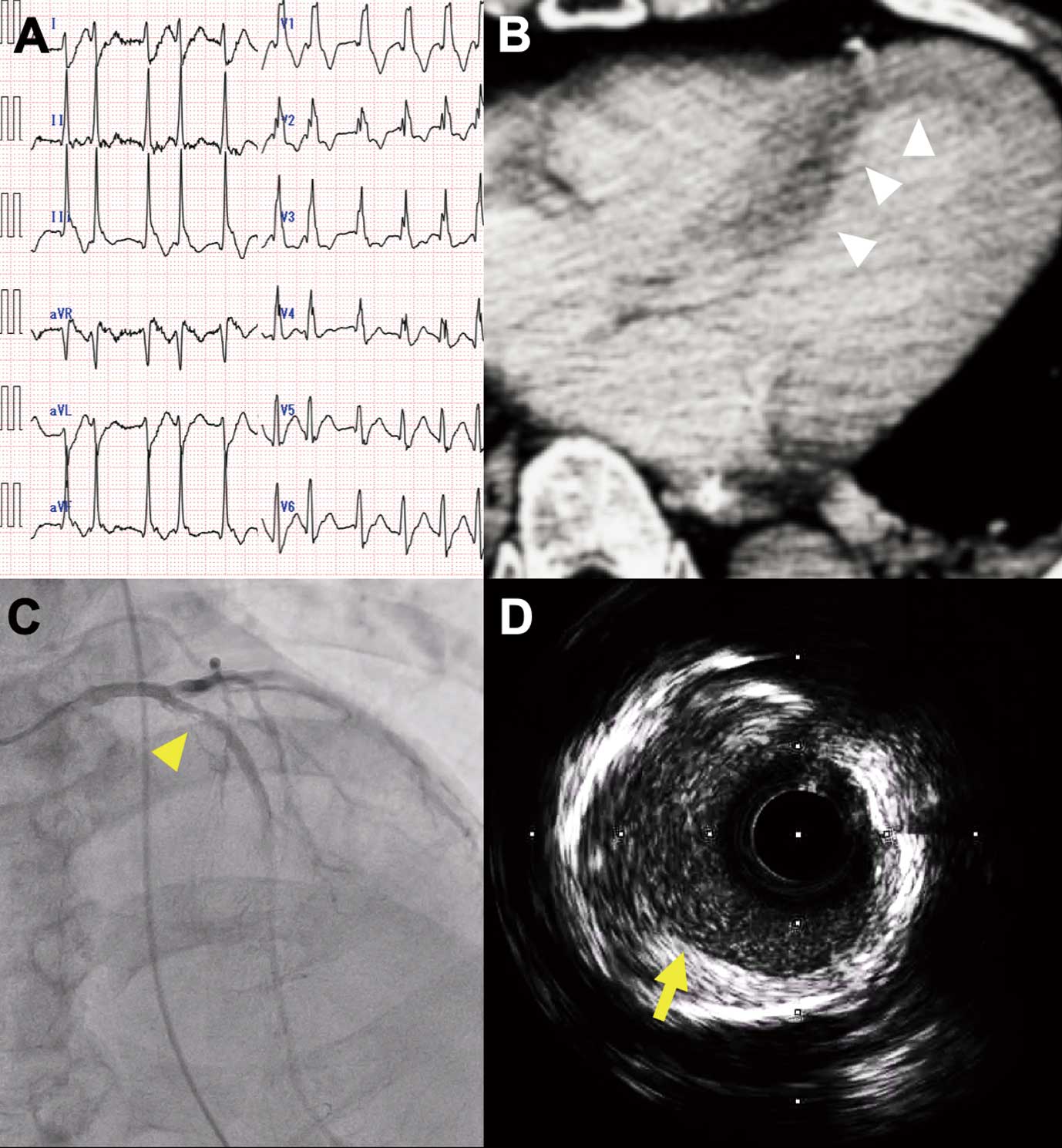
(A) ECG showing atrial fibrillation and complete right bundle-branch block without ST-segment elevation. (B) Contrast-enhanced computed tomography scan showing perfusion defect (arrowheads) in the subendocardial left ventricular anteroseptum. (C) Severe stenosis of the left anterior descending artery (LAD) on coronary angiogram (arrowhead). (D) Intravascular ultrasound shows plaque ruptures in the proximal LAD (arrow).
Because there are many mechanisms of VF in HCM,1 it can be difficult to initially confirm that the fibrillation is resulting from ischemia. The ECG abnormality of HCM and troponin-negative status in the superacute phase increase that difficulty. However, routine early CAG is not beneficial in OHCA patients without ST-segment elevation,2 but may benefit those patients with ongoing ischemia that revascularization can improve.3 Although non-gated CT does not fully assess myocardial ischemia, especially difficult in OHCA patients, in certain cases it can be considered when facing a challenging decision regarding early CAG when ongoing ischemia can be detected prior to retesting cardiac enzymes.
Grammarly, Inc. for English proofreading.