Durability of Mitral Valve Repair Performed Before the Age of 5 Years
Article ID: CJ-15-0372

Details
Article ID: CJ-15-0372
Background: Intricate repairs performed for adult mitral valve disease may not be feasible in young children because of their small annulus, future growth and also fragile tissue.
Methods and Results: Mitral valve repair was performed in 51 patients (1980–2011) aged younger than 5 years. The median follow-up was 3.0 (maximum, 24.2) years. Commissural annuloplasty technique was performed solely in 19 of 37 patients with coexisting cardiac disease. In 2 patients, Alfieri’s edge-to-edge technique was used. Repairs for the remaining 30 patients used one of the following procedures: commissural closure (8), closure of the accessory cleft or hole (7), sliding leaflet technique (6), artificial chordal placement (6) and chordal shortening technique (3). There were 3 deaths. The postoperative degree of mitral regurgitation was mild or less in 41 patients (80.4%); 9 patients required reoperation for mitral regurgitation or stenosis. Freedom from reoperation for patients with isolated mitral regurgitation and those with other congenital heart disease at 10 years was 91.7±68.0% and 68.4±9.4%, respectively. Actuarial survival was 97.0±3.0% and 85.1±9.7%, respectively.
Conclusions: Excellent survival rates were achieved after mitral valve repair in patients younger than 5 years. The incidence of both reoperation and significant regurgitation was acceptable.
The basic principles of mitral valve repair (MVR) have evolved from the adult practice.1,2 The first of these is restoration of the physiologic saddle-shape and the normal size of the annulus, which is principally achieved by using a prosthetic ring.3,4 The second is restoration of the geometric abnormality of the leaflets and chords, in this case achieved by either using artificial chords or resection and suturing of the leaflets. There are also other unique techniques such as Alfieri’s edge-to-edge repair.5
These intricate repairs, however, may not be feasible in young children because of their small annulus, future growth, fragile tissue and various other reasons. The goal of MVR in children is ideally life-long prevention of regurgitation. Descriptive information, nonetheless, is limited for exploring the optimal surgical strategy for these patients. The purpose of this study was to provide relevant information concerning MVR in children aged less than 5 years.
The study was approved by the Institutional Review Board of Sakakibara Heart Institute and the procedures were in accordance with institutional guidelines for protection of patient confidentiality. The need for patient consent was waived.
PatientsBetween September 1980 and March 2012, 51 patients younger than 5 years of age underwent MVR. Patients with atrioventricular sepal defects were excluded. During this time period, 27 patients in the same age range underwent prosthetic replacement as the initial surgical intervention for the MV. Also, there were no patients undergoing MVR for stenosis. There were 25 female and 26 male patients. The median age and body weight were 1.0 (range 0.1–4.7) years and 7.6 (range 2.7–16.0) kg, respectively. A total of 24 patients (47.1%) were infants (age <1 year).
In 38 of these patients there were coexisting congenital cardiac defects, including ventricular sepal defect (22), functionally single ventricle (6), double-outlet right ventricle (3), atrial sepal defect (2), coarctation complex (2), transposition of the great arteries (1) and tetralogy of Fallot (1). The other 14 patients had isolated congenital MV disease with regurgitation. For patients with congenital heart diseases and 2 ventricles, complete repair was performed simultaneously with MVR. For those with a functionally single ventricle, cavopulmonary anastomosis (4), Fontan operation (1) and aortopulmonary anastomosis (1) were simultaneously performed. The MV annulus, measured on the preoperative echocardiogram, ranged from 12.4 to 28 (median: 18) mm. In 3 patients, the annulus was >25 mm.
Follow-up was completed in all survivors. The median time to follow-up was 3.0 (maximum, 24.2) years. The degree of regurgitation was evaluated as none to trivial, mild, moderate and severe, according to the area of the regurgitation jet relative to the left atrium on the 4-chamber view. The endpoint of the analysis included the time to develop mitral regurgitation of a moderate degree or more, reoperation and mortality.
Statistical AnalysisPatients were stratified into groups with congenital heart disease or isolated mitral regurgitation, in order to analyze the variance in outcomes. Data are presented as median with range. Student’s t-test or 1-way analysis of variance was used to analyze intergroup differences in the continuous variables. Categorical variables were compared using Pearson’s χ2 test, Statistical analysis was performed with JMP® software for Macintosh, 10.0.2 (SAS Institute Inc, Cary, NC, USA).
In this patient group, a modified Kay and Wooler6,7 commissural annuloplasty technique was most frequently used. The stitch might be placed along the entire commissural leaflet (Figure 1A). When the stitch was placed more posteriorly, it would simultaneously approximate the posterior leaflet to the anterior leaflet and reduce the length of the posterior annulus (Figure 1B). The orifice size was essentially reduced to the normal size of the MV annulus relative to the patient’s body surface area. On the other hand, in some cases the patient underwent an annuloplasty of the posterior annulus (posterior annuloplasty). In 3 patients, interrupted annuloplasty stitches were placed along the entire posterior annulus at even intervals (Figure 2), allowing growth of the remaining portions. In 2 patients, the posterior annulus was fixed by a pericardial strip. In the remaining 2 patients, an artificial ring was used. In the first patient, described later as a mortality case, a 25-mm flexible ring (Duran AnCore® Annuloplasty System; Medtronic Inc, Minneapolis, MN, USA) was cut to an appropriate size to fit the posterior annulus. In the second patient, a 26-mm Physio Annuloplasty Ring® (Edwards Lifescience Inc, Irvine, CA, USA) was used.

Schematic of commissural annuloplasty technique. The stitch is essentially placed along the entire commissural leaflet (A). The stitch may be placed more posteriorly to stretch and bring the posterior leaflet towards the anterior leaflet (B).

Posterior annuloplasty technique using multiple pledgetted stitches.
When the regurgitation was peripheral, or near the commissure, the zone of apposition might be closed completely using interrupted stitches.
Artificial Chordal PlacementThe technique has been already described in detail.8 A CV5or 6 ePTFE suture (L. Gore & Associates, Inc, Flagstaff, AZ, USA), reinforced with a pledget, was placed in the corresponding papillary muscle. Two needles were then passed through the prolapsing segment of the leaflet. A small tourniquet was used to hold the suture at an appropriate length. After evaluating the leaflet coaptation by saline injection testing, the ePTFE suture was gently held at the lower end of the tourniquet with a right-angled clamp. The tourniquet was then removed and the suture tied.
Closure of Accessory Cleft or Hole on the LeafletWhen there was an accessory cleft or hole on the anterior leaflet causing regurgitation, this was closed using interrupted stitches.
Chordal Shortening TechniqueShortening of the elongated tendinous chords were performed in 3 patients. All the elongated chords were inserted into the middle portion of the anterior leaflet. This technique was used only if the chord was deemed to possess sufficient width and strength to withhold the tension caused by a plication suture. In all 3 cases, commissural annuloplasty was simultaneously performed in order to reduce the tension on the chord.
Sliding Leaflet Technique (Figure 3)The prolapsing segment was firstly resected in a quadrangular fashion, confirming that both ends of the remnant leaflets had sufficient thickness and strength. The adjacent leaflet tissue was then detached from the annulus, over approximately a half-length of the resected gap. The 2 leaflet ends were brought together by compression sutures placed on the annulus and sutured together. Pledgetts were used to reinforce sutures whenever the leaflet tissue was deemed fragile.

Schematic of sliding leaflet technique. First, the prolapsing segment is resected in a quadrangular fashion. Next, the adjacent leaflet is detached from the annulus for approximately a half-length of the gap (A). The 2 ends of the remaining leaflets are approximated by compression sutures placed on the annulus, and sutured together (B).
For patients who had residual regurgitation after attempts with other techniques, the Alfieri’s edge-to-edge technique was used as a salvage procedure. The anterior and posterior leaflets were sutured together at the midpoint.
The pathologic feature of the leaflet (Table 1), the main site of regurgitation (Table 2) and the main procedure used (Table 3) in patients with congenital heart disease and isolated mitral regurgitation are listed. As shown, commissural annuloplasty was performed without other combined techniques in 19 of 37 patients (51.4%) having a coexisting cardiac defect. The pathologic features of the valve in these 19 patients included annular dilatation in 10, leaflet prolapse in 6, and local dysplasia of the leaflet in 5. On the other hand, none of the cases of isolated MV disease was repaired with annuloplasty technique alone, and another technique for the leaflet or subvalvular apparatus was always used. This intergroup difference (the percentage having commissural annuloplasty in patients with isolated MR and congenital heart disease) was significant (P=0.0007).
| Congenital heart disease | Isolated mitral regurgitation | |
|---|---|---|
| Leaflet prolapse | 14 | 11 |
| Anterior | 12 | 5 |
| Anterior+posterior | 1 | 1 |
| Posterior | 1 | 5 |
| Annular dilatation | 10 | 1 |
| Local dysplasia or sclerosis | 7 | 1 |
| Accessory cleft | 5 | 1 |
| Hole in the leaflet | 1 | 0 |
A torn chord was not identified in any of the cases.
| Congenital heart disease | Isolated mitral regurgitation | |
|---|---|---|
| Central | 16 | 9 |
| Lateral | 15 | 4 |
| Cleft or hole | 6 | 1 |
| Congenital heart disease | Isolated mitral regurgitation | |
|---|---|---|
| Commissural annuloplasty | 19 | 0 |
| Commissural closure | 5 | 3 |
| Accessory cleft closure | 5 | 1 |
| Artificial chordal placement | 3 | 3 |
| Sliding leaflet technique | 0 | 6 |
| Chordal shortening | 3 | 0 |
| Edge-to-edge | 1 | 1 |
| Hole closure | 1 | 0 |
There were 3 deaths. The first was a 9-month female who had severe MV regurgitation and underwent chordal placements and a posterior annuloplasty. Immediately following the repair, MV replacement was performed for residual MV regurgitation. She was subsequently supported by extracorporeal membrane oxygenation, but died on postoperative day 9. The second patient was a 2-month female diagnosed with Marfan syndrome, multiple ventricular septal defects and moderate MV regurgitation. Commissural annuloplasty stitches reduced the regurgitation to a trivial level, but depressed ventricular function persisted, possibly because of multiple patch placements on the septal defects and prolonged myocardial ischemic time. Cardiac function progressively deteriorated and death occurred on day 27. The final patient was an 8-month male diagnosed with severe MV regurgitation and acute myocarditis. He underwent artificial chordal placements and a ring annuloplasty. At the time of MV replacement for recurrent MV regurgitation, the patient developed severe ventricular dysfunction that failed to recover, and death occurred 1 year after the initial repair.
The postoperative degree of MV regurgitation was mild or less in 41 patients (80.4%) and moderate or more in 9. In the 1 patient requiring extracorporeal membrane oxygenation, echocardiographic assessment was not performed. A total of 9 patients required reoperation for MV regurgitation or stenosis. The cardiac diagnoses of these patients included functionally single ventricle in 4, ventricular septal defect in 3, double-outlet right ventricle with aortic coarctation in 1 and isolated MR in 1. The patients with double-outlet right ventricle in particular had a small mitral annulus resulting in mitral stenosis after the repair. MV replacement was performed in 6 patients, and repeat MVR in 3. Freedom from reoperation was 78.8±6.7% at 1 year and 75.9±7.1% after 2.7 years. None required reoperation after this time period. Actuarial survival was 92.9±4.0% at 1 year and no mortality cases occurred after this time period. Freedom from MV regurgitation of a moderate degree or more was 86.2±5.7% at 1 year and 80.4±6.7% after 3.3 years. There was 1 patient who developed MV stenosis after an edge-to-edge repair. On echocardiogram, the 2 orifices were stretched, hindering a smooth valve leaflet motion and a round-shaped opening at diastole. This patient required MV replacement at 28 days. Comparison of the outcomes in patients having congenital heart disease and those with isolated mitral regurgitation are shown in Figure 4 and Figure 5, respectively.

Kaplan-Meier estimates of freedom from reoperation for patients with congenital heart disease (red line) or isolated mitral regurgitation (blue line). Numbers in parenthesis indicate patients at risk. The percentage was 72.7±8.4 at 1 year and 68.4±9.4, respectively, after 5 years for congenital heart disease, and 91.7±8.0% after 1 year for isolated mitral regurgitation. The P value for this difference (log-rank test) was 0.1363.
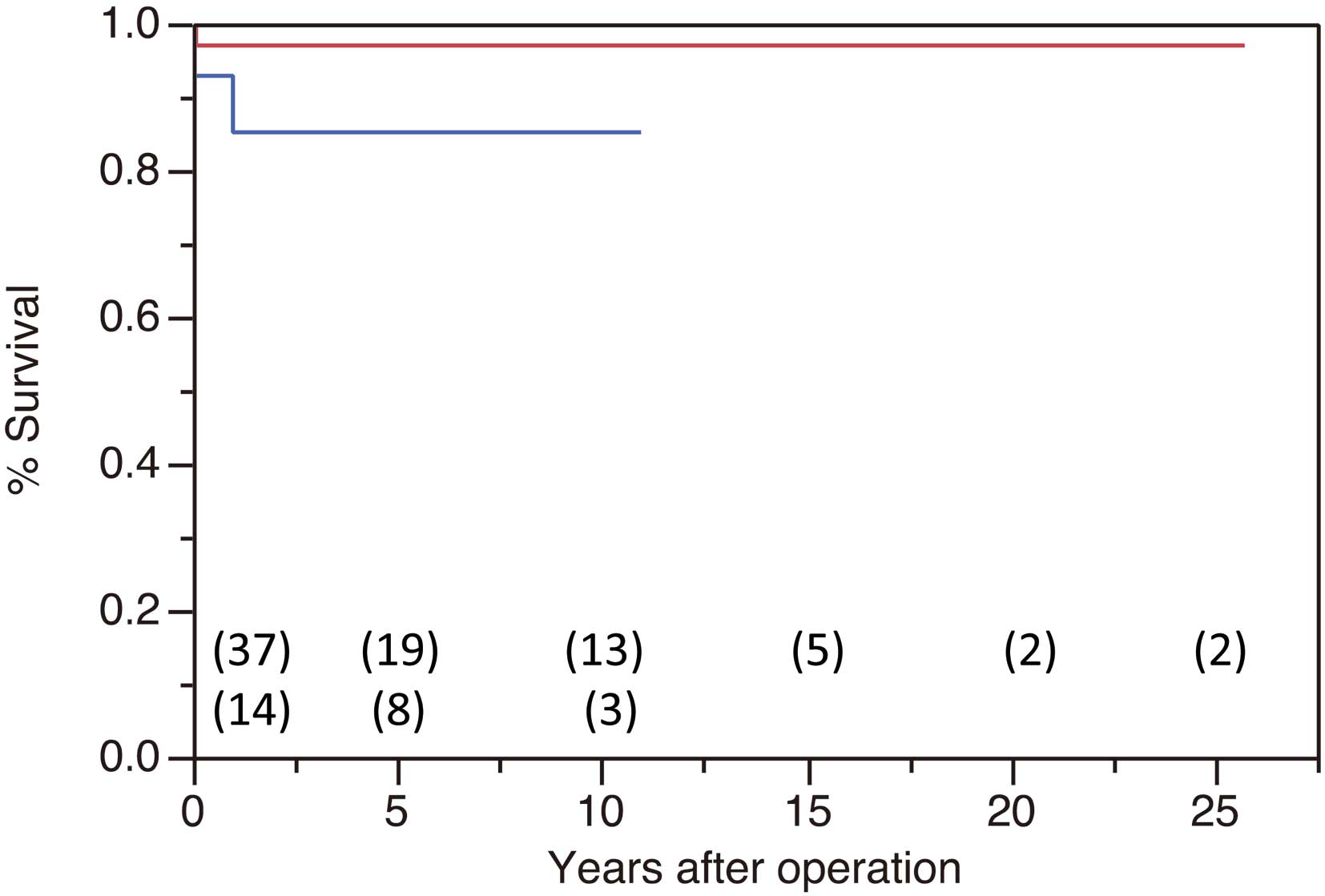
Kaplan-Meier estimates of survival for patients with congenital heart disease (red line) or isolated mitral regurgitation (blue line). Numbers in parenthesis indicate patients at risk. The percentage was 97.0±3.0 after 0.08 year for congenital heart disease, and 85.1±9.7% after 0.98 year for isolated mitral regurgitation. The P value for this difference (log-rank test) was 0.1693.
MV regurgitation may be related to a congenitally abnormal MV or occur in association with other cardiac abnormalities.9–11 Considering the future growth of pediatric patients, MVR is the preferred treatment.12 The minimum requirement of MVR in children is to allow growth of the patient, without causing irreversible myocardial damage, to an age when a prosthesis can be implanted. The ideal goal is, indisputably, life-long prevention of regurgitation.
Carpentier described a functional classification of MV regurgitation from type I to III,13 considering the mechanisms of regurgitation. Deciphering the mechanism of MV regurgitation is crucial in successful repair. It is well known that dilation of the annulus principally occurs around the posterior leaflet. In adult practice, prosthetic rings are often used to restore the saddle-shape and the normal size of the posterior annulus, and also to decrease the tension on the valve components.14 However, prosthetic rings are in general not usable in young children because of their small annulus and future growth potential. In fact, only 3 of the present patients had an annulus >25 mm. In some patients in this series, a technical modification was made to reduce the posterior annulus (posterior annuloplasty) while assuring its growth; that is, placement of multiple intermittent annuloplasty stitches and fixation of the annulus using fresh pericardium. There are reports that pericardial fixation of the posterior annulus helps maintain valve geometry15 while allowing annular growth.16 It is, however, also possible that pericardium may become rigid and calcified.17 Presently, we do not consider this technique to be the best choice for young children with a small annulus.
Suture commissural annuloplasty, plicating the annular part of the commissure, improves coaptation of the leaflets. Also, by mobilizing the posterior leaflet to the commissural portion using the suture, the leaflet can be stretched and brought towards the anterior leaflet.7 This technique may be used as an adjunct to others, targeting the leaflet or subvalvular apparatus. The commissural annuloplasty technique may aid in reducing the tension on the valve components, and thus in part generate a similar effect as an artificial ring.
It is well known that closure of an atrial septal defect leads to normalization of the sepal curvature and left ventricular geometry, and thus reduces the degree of MV prolapse and regurgitation.18,19 In patients with a ventricular septal defect, the cause of MV regurgitation is considered attributable to the annular dilatation.20,21 These patients may have near-normal MV morphology. Commissural annuloplasty, therefore, may result in a favorable outcome for these patients, as the volume reduction and geometric changes of the left ventricle multiply the effect of the repair.22 In fact, in the present study the MV was repaired exclusively with commissural annuloplasty in approximately half of the patients with coexisting cardiac diseases, whereas repairs for isolated MV disease always involved other techniques. Our results, however, showed worse outcomes for MVR in terms of the reoperation rate for patients with congenital heart disease. This was obviously related to the fact that 4 of them had a functionally single ventricle, which is known to be notoriously difficult to repair, and also to the patient with a double-outlet right ventricle and small annulus who developed mitral stenosis after the repair. The survival rate was, however, similar between the 2 groups. The principal reason for this is the small number of deaths (3). Specifically, in the 2 cases of isolated MV regurgitation, the patients had a severe degree of regurgitation before the repair, and in the third case the patient had myocarditis.
In some patients, an eccentric regurgitation jet may originate from a region close to the commissure. In a large series of surgical repair for commissural prolapse, closure of the prolapsing segment (commissure closure) was used in approximately 50%,23 and we consider this the procedure of choice in this context. When the prolapsing segment of the anterior leaflet is remote from the commissure or around the center point, our method of choice has been to use an artificial chord even in children. Also, shortening of the elongated chord may be the best choice if it appears to have sufficient strength to withhold the tension of the suture. Reports on artificial chordal placements, used for leaflet prolapse in children, are limited. Some report a favorable late outcome that may be attributable to an age-proportional growth of the papillary muscle.24 For prolapse of the posterior middle scallop, on the other hand, a sliding leaflet technique has been our method of choice. This technique was first reported by Carpentier’s group,25 followed by other variations.26,27 In young children, there is a concern of suture dehiscence because of the fragile tissue. This did not occur in our series and none of the patients required reoperation after repair using this technique.
An accessory cleft, dividing the anterior leaflet of the MV, is a distinct morphologic entity different from the cleft of the left-sided valve of an atrioventricular septal defect. It is known that direct suturing of the cleft results in an excellent midterm result,28 and our results were consistent with that.
Alfieri’s edge-to-edge technique is reported to be effective even for young children.29 However, 1 of our patients developed MV stenosis after repair using this technique. The MV essentially has a bileaflet structure, and suturing the 2 leaflets might hinder smooth leaflet opening of the double orifice. This is in contrast with the same technique applied for a tricuspid valve (suturing of the anterior and sepal leaflets) and a common atrioventricular valve with a single ventricle (2 bridging leaflets) where unhindered opening of the 2 orifices can be expected.30 Presently, we make every effort to avoid using this technique unless the patient has a sufficiently enlarged MV annulus.
In 1 of our mortality cases the patients had acute myocarditis resulting in severe MV regurgitation. Surgical results of this patient group are poor;31 however, repair was conducted in this patient because of the intractable heart failure. In another mortality case, the patient had Marfan syndrome, which could affect the outcome of repair. Presently there is consensus that MVR is justified in children with Marfan syndrome.32 In the present case, the cause of death seemed to be ensuing heart failure caused by multiple patch placements for ventricular sepal defects.
This study encompassed over 24 years of institutional experience with MVR in young children. There have been some transitions in the procedural choice, and our current treatment policy can be summarized as follows. Regurgitation through an accessory cleft or hole is most likely abolished by simple closure. The region of eccentric regurgitation close to the commissure is often closed. For anterior leaflet prolapse remote from the commissure, artificial chordal placement or a chordal shortening technique is used. For prolapse of the posterior middle scallop, a sliding leaflet technique is the preferred choice. Commissural annuloplasty may be performed when there is no or only minor structural abnormality. This procedure, however, has never been adopted independently for isolated MV disease. It can be also used as an adjunct to other procedures targeting the subvalvular apparatus or the leaflet. Entire fixation of the posterior annulus is considered only when the MV annulus exceeds adult size. Edge-to-edge repair has not been performed recently because of the potential for postoperative MV stenosis. The choice of procedure may be influenced by the presence of coexisting congenital heart disorder, as left ventricular loading and geometry are likely to be optimized by the repair. Under these treatment policies, an excellent survival rate has been achieved after MVR in patients younger than 5 years. The incidence of both reoperation and significant (moderate or more) regurgitation was acceptable, albeit not ideal.