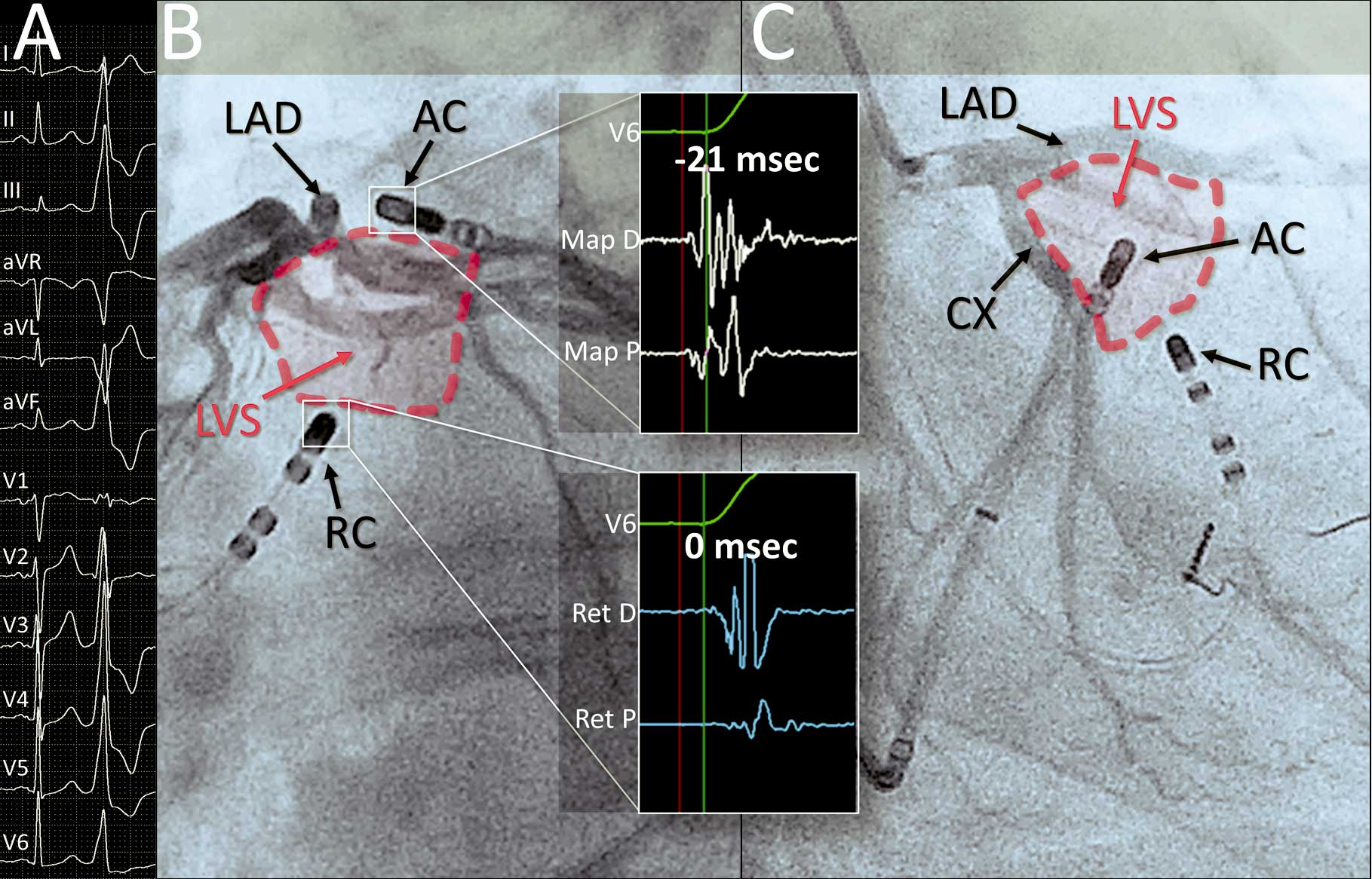
Bipolar radiofrequency catheter ablation (RFCA) is an emerging option for treatment of arrhythmias resistant to standard unipolar attempts. A 43-year-old man was referred for bipolar ablation after 2 previously unsuccessful RFCA for symptomatic premature ventricular complexes (PVC) originating from the left ventricular summit (LVS;
Figure A). Previous RFCA from the distal coronary venous system and from the anatomically adjacent endocardium failed. Mapping of the great cardiac vein performed with an irrigated 3.5-mm ablation catheter (AC) showed the earliest activation in the epicardial area of LVS. A second 4-mm AC, which served as a return catheter (RC), was introduced into LV outflow tract to the area of earliest endocardial PVC activation, and was connected to the modified purpose-made switchbox in order to connect the tip electrode (instead of dispersive patch) to the RF generator, and to transfer temperature data to the second RF generator, in order to provide simultaneous temperature monitoring from the RC at the time of RFCA. Regular left anterior oblique views commonly used for ablation of PVC arising from LVS were insufficient to visualize the distance between the ablation site and the left anterior descending artery (LAD) and circumflex artery (CX;
Figure B). Therefore, modified right anterior oblique (RAO)/caudal views were used, because only these views provided sufficient images for simultaneous visualisation of the AC, RC, LAD and CX (Figure C;
Movie S1). Baseline impedance between the AC and RC oscillated between 190 and 220 Ω. Five bipolar endo-epicardial applications up to a maximum of 27 W, followed by continuous impedance drop to 140–180 Ω, led to successful elimination of PVC, with no recurrence during follow-up.
The complex anatomy of the LVS may play a significant role in effective lesion formation.1
These anatomical conditions include the presence of very thick myocardium and epicardial fat. Thus, alternative energy delivery methods, enabling creation of true transmural lesions, may be required. The bipolar method, first established for posteroseptal accessory pathways ablation, was recently used for treatment of PVC originating from the septal area of outflow tracts,2
as well as to cure atrial flutter,3
and its use for ablation of arrhythmias originating from the LVS has been suggested.4,5
Lesions created by bipolar energy have more concentrated structure than those created by unipolar energy, because the bipolar ablation affects the vector of RF current, redirecting it towards deep myocardium, and this feature may also limit the collateral damage. This may result in more effective ablation6
and reduce the risk of complications. Possible damage to coronary arteries within the bipolar RF circuit, however, remains the main limitation of this technique, and the proximity of the LAD and CX may limit bipolar RFCA in LVS. Modified RAO/caudal views may be helpful in appropriate placement of catheters and in achieving safe distance from the coronary arteries surrounding the LVS. Other methods that may be of value in the ablation of difficult-to-treat arrhythmias originating from the LVS may include prolonged ablation from the opposite LV endocardium7
or simultaneous unipolar ablation.4
In conclusion, bipolar endo-epicardial RFCA can be used to treat PVC originating from the LVS resistant to standard unipolar RF ablation, and modified fluoroscopic views may increase the safety of this emerging approach.
Disclosures
The authors declare no conflict of interest.
Supplementary Files
Supplementary File 1
Movie S1.
Bipolar ablation: Fluoroscopic recordings of the left ventricular summit (LVS) in left anterior oblique (32°) projection and right lateral oblique (42°) and caudal (20°) projection.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-17-0782
References
- 1.
Santangeli P, Marchlinski FE, Zado ES, Benhayon D, Hutchinson MD, Lin D, et al. Percutaneous epicardial ablation of ventricular arrhythmias arising from the left ventricular summit: Outcomes and electrocardiogram correlates of success. Circ Arrhythm Electrophysiol 2015; 8: 337–343.
- 2.
Teh AW, Reddy VY, Koruth JS, Miller MA, Choudry S, D’Avila A, et al. Bipolar radiofrequency catheter ablation for refractory ventricular outflow tract arrhythmias. J Cardiovasc Electrophysiol 2014; 25: 1093–1099.
- 3.
Futyma P, Futyma M, Maciołek M, Kułakowski P. Bipolar radiofrequency ablation of typical atrial flutter. J Cardiovasc Electrophysiol 2016; 27: 874–875.
- 4.
Yamada T, Maddox WR, McElderry HT, Doppalapudi H, Plumb VJ, Kay GN. Radiofrequency catheter ablation of idiopathic ventricular arrhythmias originating from intramural foci in the left ventricular outflow tract: Efficacy of sequential versus simultaneous unipolar catheter ablation. Circ Arrhythm Electrophysiol 2015; 8: 344–352.
- 5.
Heeger CH, Hayashi K, Kuck KH, Ouyang F. Catheter ablation of idiopathic ventricular arrhythmias arising from the cardiac outflow tracts: Recent insights and techniques for the successful treatment of common and challenging cases. Circ J 2016; 80: 1073–1086.
- 6.
Nagashima K, Watanabe I, Okumura Y, Ohkubo K, Kofune M, Ohya T, et al. Lesion formation by ventricular septal ablation with irrigated electrodes: Comparison of bipolar and sequential unipolar ablation. Circ J 2011; 75: 565–570.
- 7.
Yamada T, Yoshida N, Doppalapudi H, Litovsky SH, McElderry HT, Kay GN. Efficacy of an anatomical approach in radiofrequency catheter ablation of idiopathic ventricular arrhythmias originating from the left ventricular outflow tract. Circ Arrhythm Electrophysiol 2017; 10: e004959.
